
Epilepsy is one of Pennsylvania’s original qualifying conditions under the Medical Marijuana Act and it is also one of the conditions where the relationship between cannabis and clinical care is most nuanced. More than anywhere else in the PA MMJ program, epilepsy patients and caregivers need to understand a distinction that almost no cannabis website explains clearly: the difference between FDA-approved pharmaceutical CBD and the cannabis products available at Pennsylvania dispensaries.
Getting this wrong has real consequences. This page gives you an honest account of both pathways, what the evidence actually shows, the drug interactions that matter most for epilepsy patients, and how to access the PA MMJ program if it’s the right choice for you or your child.
Does Epilepsy Qualify for Medical Marijuana in Pennsylvania?
Yes. Epilepsy is an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016) and recognized by the Pennsylvania Department of Health (DOH) for patients of all ages, including minors. There is no requirement that epilepsy be treatment-resistant, severe, or a specific syndrome to qualify. A confirmed epilepsy diagnosis is sufficient.
Pennsylvania also separately lists intractable seizures as a distinct qualifying condition, covering patients with seizure disorders that have not responded to medications, regardless of formal epilepsy diagnosis. Patients with drug-resistant epilepsy may qualify under either or both categories.
- Source: Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Source: Pennsylvania Medical Marijuana Act – Act 16 of 2016
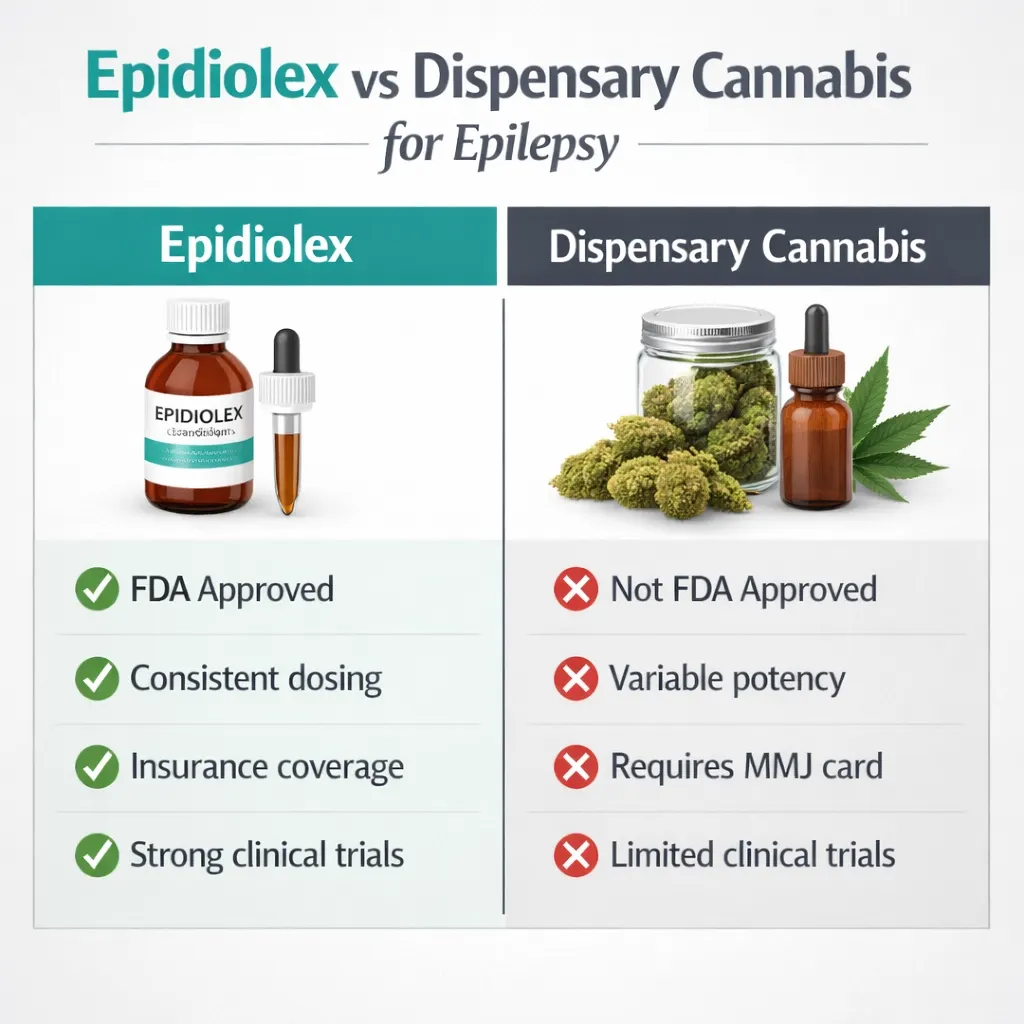
The Most Important Thing to Understand First: Epidiolex vs. Dispensary Cannabis
Before reviewing any evidence, this distinction must be clearly understood because it affects what you should actually do if you have drug-resistant epilepsy.
Epidiolex is pharmaceutical-grade, highly purified cannabidiol (CBD) oral solution manufactured by Jazz Pharmaceuticals. It is FDA-approved by prescription for seizures associated with three specific conditions:
- Lennox-Gastaut syndrome (LGS) in patients 1 year and older
- Dravet syndrome (DS) in patients 1 year and older
- Tuberous sclerosis complex (TSC) in patients 1 year and older
Epidiolex requires a prescription from any licensed physician, no MMJ card, no PA DOH registration, no dispensary. It is the most rigorously studied cannabinoid medicine in history, with multiple phase III randomized controlled trials supporting its FDA approval. It is covered by some insurance plans. It undergoes pharmaceutical quality control to ensure consistent potency.
Dispensary cannabis — the oils, tinctures, and other products available at Pennsylvania MMJ dispensaries, is different in every practical way. It is not FDA-approved for epilepsy. It is not subject to pharmaceutical quality control. Potency and formulation vary between products and batches. It requires a PA MMJ card. It is not covered by insurance.
What this means for you:
If you have Lennox-Gastaut syndrome, Dravet syndrome, or tuberous sclerosis complex, talk to your neurologist about Epidiolex first. It is available by regular prescription at any pharmacy and has stronger, more consistent evidence than any dispensary product for these specific syndromes. Your PA MMJ card gives you access to a different and less regulated category of cannabinoid products.
If you have drug-resistant epilepsy of a type not covered by Epidiolex’s approved indications or if your neurologist has already considered and declined Epidiolex, your PA MMJ card becomes the relevant pathway to CBD-dominant cannabis products.
If your epilepsy is managed adequately by standard AEDs, the case for adding cannabis is weaker and the drug interaction risks (detailed below) deserve careful consideration before proceeding.
This is not a reason to avoid the PA MMJ program. It is a reason to approach it with the right clinical framing.
- Source: Epidiolex – FDA-Approved Clinical Study Results
- Source: PMC – Consensus Panel Recommendations for Epidiolex Treatment Optimization (Wechsler et al., 2024)
What Is Epilepsy?
Epilepsy is a neurological condition characterized by recurrent, unprovoked seizures caused by abnormal electrical activity in the brain. According to the Pennsylvania DOH, epilepsy is the third most common neurological condition in the Commonwealth, affecting approximately 2% of residents. Worldwide, epilepsy affects roughly 65 million people.
Seizures can take many forms — from brief absence episodes (blank stares) to tonic-clonic convulsions. They can be focal (arising from one area of the brain) or generalized (involving the entire brain simultaneously). The classification of seizure type and epilepsy syndrome guides treatment.
Approximately one-third of all epilepsy patients around 30–35% have drug-resistant epilepsy, defined as failure to achieve sustained seizure freedom despite adequate trials of two appropriate antiseizure medications (ASMs). This population is the primary target for cannabinoid intervention in epilepsy. Standard ASMs, of which there are over 30 now available, simply do not work adequately for these patients. Their seizure burden remains high, their quality of life is significantly impaired, and their risk of sudden unexpected death in epilepsy (SUDEP) is substantially elevated.
- Source: NIH – Epilepsy: What We Know
- Source: Epilepsy Foundation – About Epilepsy
The Scientific Basis: How CBD Works Against Seizures
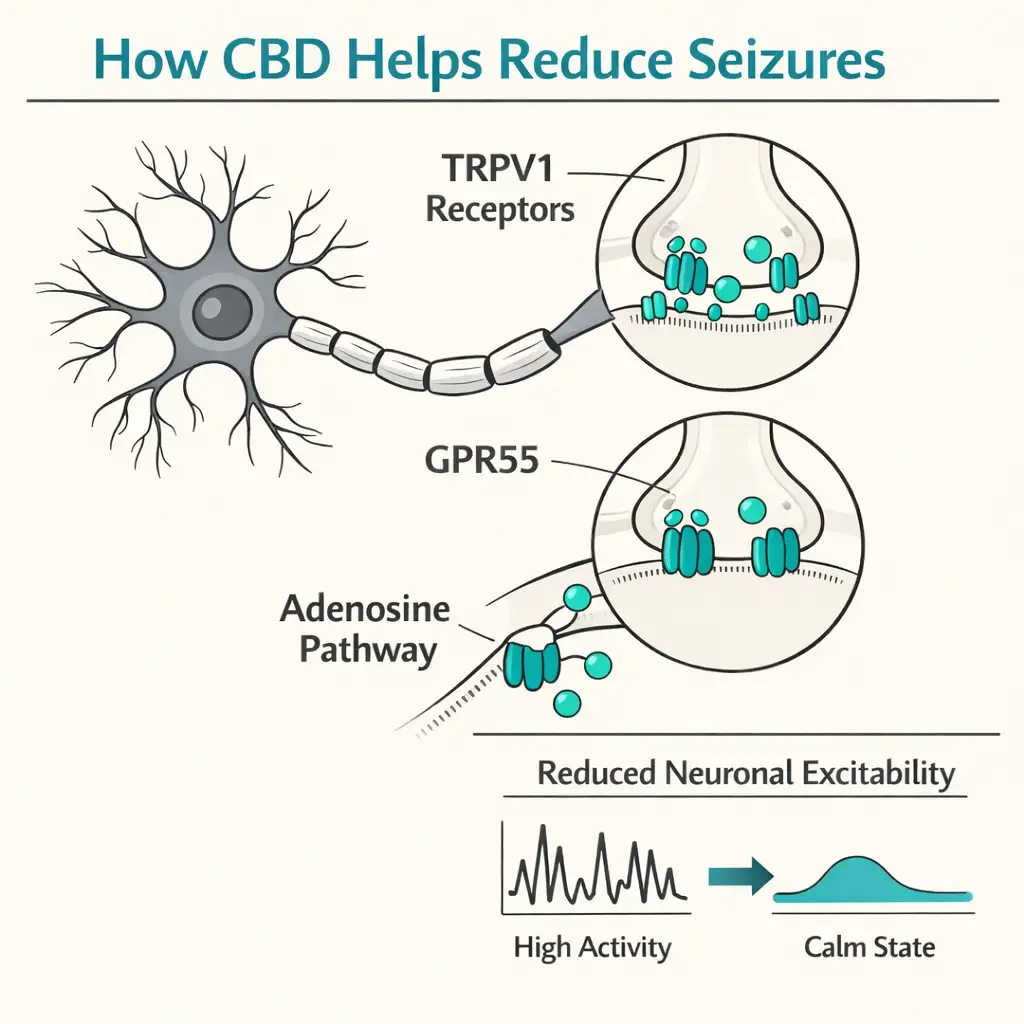
CBD’s antiseizure mechanism is fundamentally different from most conventional antiseizure medications. Rather than acting on sodium channels or GABAergic systems (the primary targets of most ASMs), CBD exerts its anticonvulsant effects through multiple distinct pathways:
- TRPV1 receptor activation — reducing neuronal excitability and calcium-mediated excitotoxicity
- Adenosine reuptake inhibition — increasing adenosine signaling, which has inhibitory effects on neuronal activity
- GPR55 antagonism — reducing intracellular calcium in neurons
- 5-HT1A receptor interaction — relevant to the mechanism in Dravet syndrome specifically, where preclinical evidence shows blocking this receptor eliminates CBD’s anticonvulsant effect
- Enhancement of endocannabinoid signaling via FAAH inhibition
This multi-target mechanism is considered a significant advantage: CBD may be effective in seizure types that are resistant to single-mechanism drugs. It is also why CBD has shown antiseizure activity across a range of epilepsy syndromes beyond just the three FDA-approved indications because its mechanism does not depend on a syndrome-specific biology.
Critically, the evidence for CBD in epilepsy is specifically about CBD, not THC. High-THC products have inconsistent and potentially proconvulsant effects at higher doses in some patients. The epilepsy evidence base is built on CBD-dominant or CBD-only formulations.
- Source: Frontiers in Pharmacology – Epilepsy, Neuroinflammation and Cannabidiol (2025)
- Source: PMC – Cannabidiol in the Treatment of Epilepsy: A Focused Review (2020)
The Clinical Evidence: What the Research Shows
Dravet Syndrome — The Landmark NEJM Trial
The most important single study in cannabinoid epilepsy research is the 2017 phase III randomized, double-blind, placebo-controlled trial of CBD for Dravet syndrome published in the New England Journal of Medicine (Devinsky et al.).
120 children and young adults with Dravet syndrome and drug-resistant seizures were randomized to CBD oral solution (20 mg/kg/day) or placebo, added to their existing antiseizure regimens. The primary outcome was change in convulsive seizure frequency over 14 weeks.
The results: the median frequency of convulsive seizures decreased from 12.4 to 5.9 per month in the CBD group, compared to a decrease from 14.9 to 14.1 in the placebo group. The adjusted median difference between groups was −22.8 percentage points (p < 0.001). Three patients in the CBD group became completely seizure-free. This trial formed a central part of the FDA approval package for Epidiolex.
Lennox-Gastaut Syndrome — The Phase III LGS Trials
Two phase III RCTs established Epidiolex’s efficacy in LGS. In the pivotal trial (Thiele et al., published in The Lancet), 225 patients were randomized to CBD 20 mg/kg/day, 10 mg/kg/day, or placebo. Drop seizure frequency reductions were 41.9% for the 20 mg/kg group and 37.2% for the 10 mg/kg group, versus 17.2% for placebo — statistically significant differences with clinical meaningfulness in a population where seizure reduction of any degree represents a major advance.
Tuberous Sclerosis Complex — TSC Approval
In 2020, the FDA expanded Epidiolex’s approval to cover TSC-associated seizures, supported by a phase III RCT in 224 patients receiving CBD at 25 or 50 mg/kg/day or placebo for 16 weeks. Both CBD doses significantly reduced TSC-associated seizure frequency versus placebo, adding to the breadth of CBD’s demonstrated antiseizure efficacy.
Beyond Dravet, LGS, and TSC — Drug-Resistant Epilepsy of Any Cause
This is the most clinically relevant area for Pennsylvania MMJ patients, because most epilepsy patients do not have Dravet, LGS, or TSC. The question is whether CBD helps in drug-resistant epilepsy from other causes and the accumulating real-world evidence is encouraging.
A 2023 multicenter retrospective study from six German epilepsy centers (Neurological Research and Practice) enrolled 108 patients with refractory focal-onset, genetic generalized, and other epilepsies treated with CBD off-label. Meaningful seizure reduction was observed across epilepsy types, without the treatment response being limited to the three approved syndromes.
A 2023 real-world study from Colombian epilepsy centers (Seizure: European Journal of Epilepsy, Espinosa-Jovel et al.) enrolled 78 patients with drug-resistant epilepsy not related to LGS, Dravet, or TSC, a median age of 24 years, using a median of 3 concurrent ASMs, with a median of 30 monthly seizures at baseline. After a median 14 months of CBD treatment, mean seizure reduction was 67.8%, with 68.8% of patients achieving at least 50% seizure reduction and 11.5% achieving seizure freedom. Efficacy was independent of whether patients were taking clobazam.
A 2023 retrospective multicenter study from 16 epilepsy centers (Epilepsia Open, Kühne et al.) included 311 patients, including both children and adults, with a wide spectrum of epilepsy syndromes. The study found CBD efficacy across epilepsy types beyond the approved indications, with approximately 35–65% of patients across different syndrome categories achieving at least 50% seizure reduction.
A 2025 real-world case series (Frontiers in Neuroscience) documented 19 patients with drug-resistant epilepsy who achieved seizure freedom of at least 90 days during cannabis-based product treatment. Crucially, the seizure-free patients were not limited to LGS and Dravet, confirming CBD’s potential efficacy across a broad spectrum of drug-resistant epilepsy beyond the FDA-approved indications.
- Source: Neurological Research and Practice – Off-Label CBD for Refractory Focal, Genetic Generalised, and Other Epilepsies (2025)
- Source: Seizure Journal / PubMed – CBD for Drug-Resistant Epilepsy Not Related to LGS, Dravet, or TSC (Espinosa-Jovel et al., 2023)
- Source: PMC – Real-World Data on CBD Across Epilepsy Subtypes: Multicenter Study (Kühne et al., 2023)
- Source: Frontiers in Neuroscience – 19 Patients Report Seizure Freedom with Cannabis-Based Product Treatment (2025)
The Honest Limits: Where Evidence Is Still Weak
Adult focal epilepsy: Most of the evidence comes from pediatric populations and developmental epileptic encephalopathies. Data on CBD for common adult focal epilepsy is limited. One placebo-controlled trial of a topical CBD gel in 188 adults with intractable focal epilepsy (no clobazam) found no significant seizure reduction. Adult focal epilepsy remains a gap in the evidence base.
THC-containing products: The evidence for THC in epilepsy is inconsistent and concerning at higher doses in some models. Low-dose THC combined with CBD has shown some benefit in preclinical work, but high-THC products are generally not recommended for epilepsy patients and carry theoretical proconvulsant risk at high doses. CBD-dominant products are the appropriate choice for seizure management.
Dispensary products vs. pharmaceutical CBD: No dispensary cannabis product has been tested in the rigorous phase III RCTs that support Epidiolex. Real-world reports of benefit with dispensary products exist, but their consistency and reliability are lower than pharmaceutical-grade CBD. Product potency and purity vary significantly between dispensary items.
The Drug Interactions You Cannot Ignore
This section is arguably the most important clinical section on this page and the one least covered by competing websites. CBD has significant pharmacokinetic interactions with the antiseizure medications most commonly used in drug-resistant epilepsy. These interactions are not theoretical; they are documented in FDA labeling, published clinical trials, and real-world monitoring data.
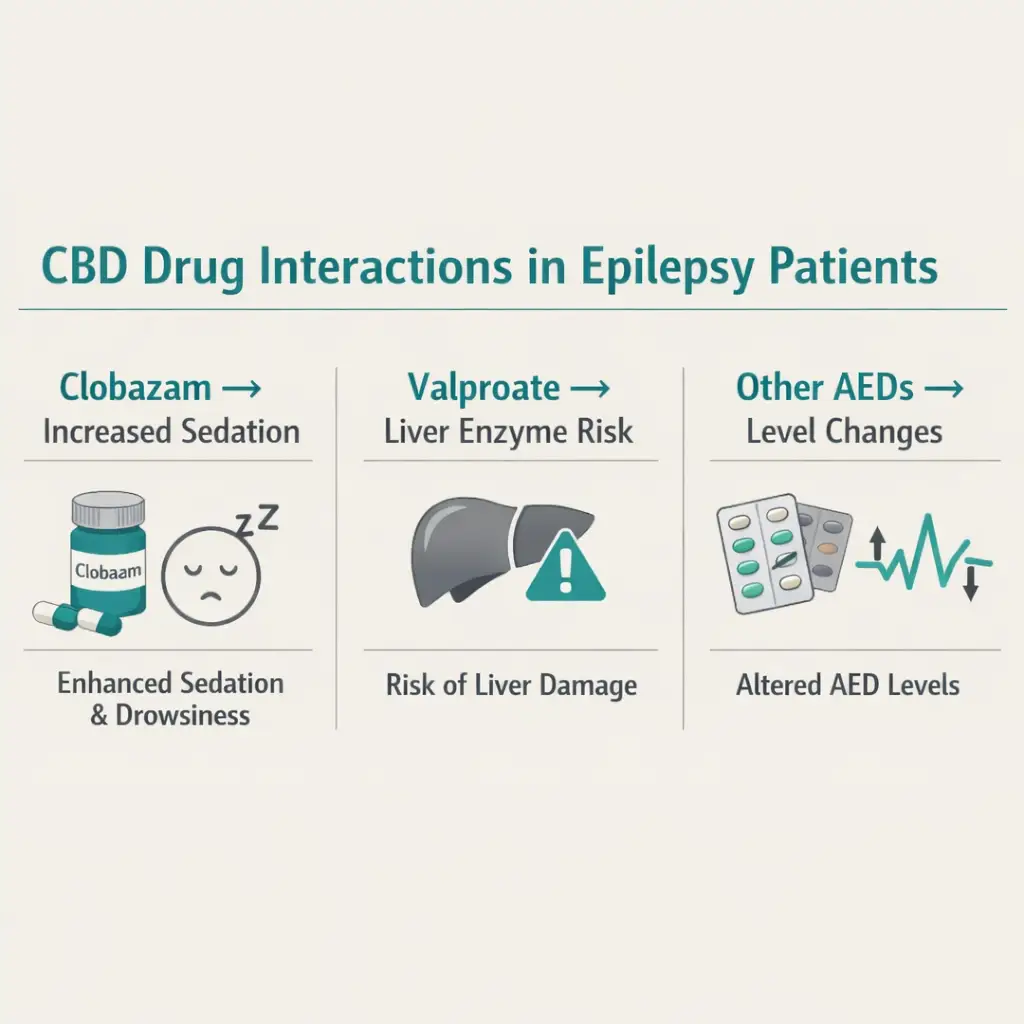
Clobazam (Onfi) — The Most Clinically Significant Interaction
Clobazam is one of the most commonly used add-on AEDs in drug-resistant epilepsy, particularly in LGS and Dravet. CBD inhibits CYP2C19, the primary enzyme that metabolizes clobazam’s active metabolite N-desmethylclobazam (N-CLB). The result: when CBD is added to clobazam, N-CLB levels can increase up to 3–5 fold or more. Elevated N-CLB produces the same effects as excessive clobazam, sedation, somnolence, ataxia, and respiratory depression.
In clinical practice, this interaction is manageable but requires active monitoring. Clobazam doses typically need to be reduced by 25–50% when CBD is added. Therapeutic drug monitoring of clobazam and N-CLB levels is recommended. This interaction is explicitly documented in the Epidiolex FDA prescribing information.
Importantly, this interaction may also explain some of CBD’s antiseizure efficacy in clobazam-treated patients, the CBD is partly working by increasing effective clobazam exposure. Whether this is beneficial or concerning depends on the clinical picture, but it should be understood rather than ignored.
- Source: PubMed – Drug-Drug Interaction Between Clobazam and Cannabidiol in Children with Refractory Epilepsy (Geffrey et al., 2015)
- Source: FDA – Epidiolex Prescribing Information (accessdata.fda.gov)
Valproate (Depakote, Depakene) — Liver Enzyme Elevation Risk
Valproate is widely used in generalized epilepsies. When CBD is added to valproate, there is a significantly increased risk of elevated liver transaminases (ALT/AST). In the Epidiolex clinical trials, the incidence of ALT elevations greater than three times the upper limit of normal was:
- 30% in patients taking both valproate and clobazam with CBD
- 21% in patients taking valproate (without clobazam) with CBD
- 3–4% in patients taking neither valproate nor clobazam with CBD
Valproate co-administration requires baseline and ongoing liver function monitoring when adding CBD. In most cases, transaminase elevations resolve with dose reduction or discontinuation, but in some patients, valproate dose reduction or discontinuation becomes necessary. This is a well-characterized, clinically managed risk, not an absolute contraindication but it must be explicitly discussed with the treating neurologist before starting any CBD product.
- Source: FDA – Epidiolex Prescribing Information
- Source: PMC – Interactions Between CBD and Commonly Used AEDs (Gaston et al., 2017)
Other Documented AED Interactions
CBD also significantly increases plasma levels of:
- Rufinamide (Banzel) — dose adjustment may be needed
- Topiramate (Topamax) — increases in topiramate levels have been documented
- Zonisamide and eslicarbazepine — significant increases in adults
- Stiripentol — co-administration increases CBD plasma levels substantially
Enzyme-inducing AEDs (carbamazepine, phenytoin, phenobarbital, primidone) work in the opposite direction: they induce CYP enzymes that metabolize CBD, potentially reducing CBD plasma levels and effectiveness. Patients on these medications may need higher CBD doses to achieve therapeutic effect.
The non-negotiable clinical rule: Before adding any CBD product, Epidiolex or dispensary-sourced, to an existing AED regimen, the prescribing neurologist or epileptologist must review every concurrent medication. This is not optional, and it is the reason the certifying physician for your PA MMJ card will ask for your complete medication list.
THC and Seizures: A Specific Warning
Unlike CBD, THC’s effects on seizure activity are inconsistent and potentially harmful at higher doses. Multiple animal models have shown that high-dose THC can be proconvulsant. In human observational data, some patients report worsening seizure control with THC-containing products.
For epilepsy patients using PA dispensary products, CBD-dominant formulations are strongly preferred. Products with high THC content should generally be avoided unless specifically discussed with and approved by your neurologist. This includes products marketed as “balanced” (1:1 THC:CBD), these may be appropriate for other conditions but represent a significant uncertainty in seizure management.
The Epilepsy Foundation’s position is that pharmaceutical-grade CBD (Epidiolex) is preferred over botanical cannabis products for seizure management because of the consistency of dosing, quality control, and the evidence base it carries.
Practical Guidance: PA MMJ Products for Epilepsy
Pennsylvania’s approved forms include oils and tinctures, capsules and pills, vaporizable dry leaf (vaporizer only, smoking is not permitted), liquid solutions and metered-dose inhalers, patches, and topicals.
For seizure management, CBD-dominant oral oils and tinctures are the most appropriate dispensary format. They allow measured dosing, have predictable absorption when taken with food (fat enhances CBD absorption significantly, taking CBD on an empty stomach can reduce absorption by up to 14-fold), and provide longer, more stable duration than inhaled forms.
When selecting a product at a PA dispensary:
- Ask specifically for CBD-dominant products with known CBD:THC ratios — ideally 20:1 or higher CBD to THC
- Ask whether the product has a Certificate of Analysis (COA) from a third-party laboratory confirming cannabinoid content
- Start with the lowest available dose and increase slowly to reduce the risk of drug interaction effects on existing AEDs
- Take CBD products with food — fat content substantially increases bioavailability
Do not make any changes to existing antiseizure medications based on cannabis use without your neurologist’s involvement. Never reduce or stop an AED because seizures appear better controlled after adding cannabis. Abrupt AED withdrawal can trigger severe rebound seizures and status epilepticus.
How to Get Your Pennsylvania Medical Marijuana Card for Epilepsy
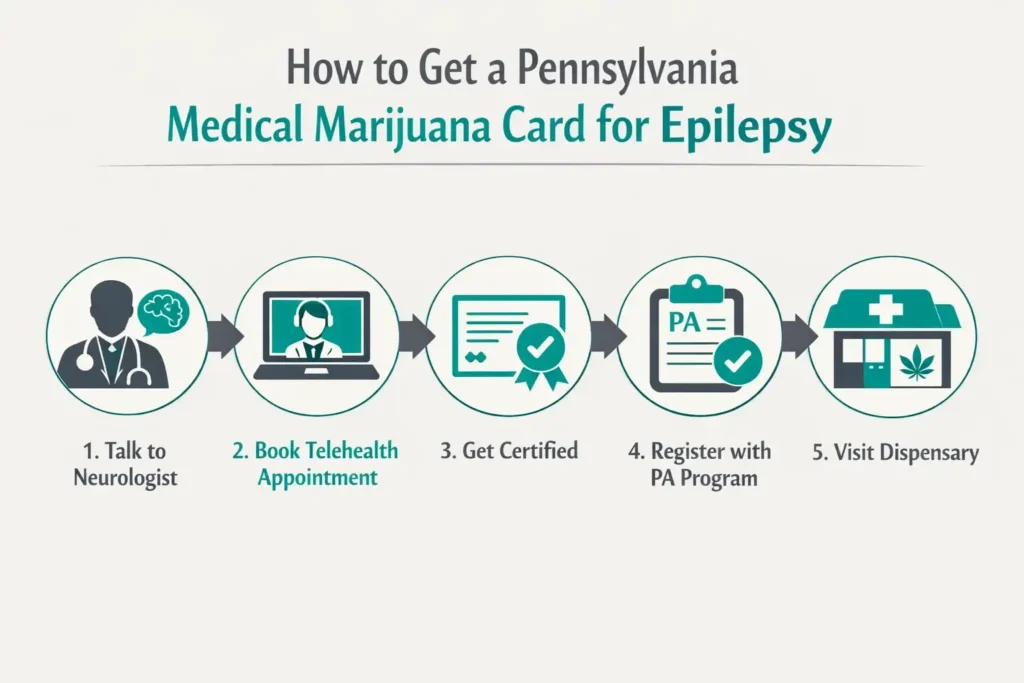
Step 1 — Talk to Your Neurologist First
This is the step that differentiates epilepsy from almost every other qualifying condition on Pennsylvania’s list. Before pursuing a PA MMJ card, have an explicit conversation with your neurologist or epileptologist about:
- Whether Epidiolex (prescription CBD) is appropriate for your specific diagnosis
- Which of your current AEDs have known interactions with CBD (particularly clobazam and valproate)
- Whether baseline liver function tests should be ordered before starting any CBD product
- What monitoring should be in place after starting cannabis
This conversation protects you and enables the certifying physician for your PA MMJ card to make appropriate recommendations.
Step 2 — Physician Certification (Telehealth)
Schedule a telehealth appointment with a PA DOH-registered medical marijuana physician. The evaluation typically takes 10–15 minutes. The certifying physician needs to confirm your epilepsy diagnosis and discuss your symptom profile. Most critically: bring your complete medication list including every current AED at its current dose. The certifying physician will review interaction considerations as part of the evaluation.
For minor patients: a parent or legal guardian registers as the designated caregiver. The certifying physician must be comfortable with pediatric patients, confirm this when scheduling.
Step 3 — State Registration
After certification is issued, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com) with your certification, a valid PA driver’s license or state-issued ID, and the $50 annual fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 4 — Dispensary Visit
At the dispensary, tell the pharmacist you have epilepsy and specifically ask for CBD-dominant products. Share your AED list, a dispensary pharmacist can provide product-level guidance on formulations and ratios. Do not purchase high-THC products for seizure management.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Anxiety Disorder
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: My child has Dravet syndrome. Should I get a PA MMJ card or ask for Epidiolex?
Q: My epilepsy is well-controlled on levetiracetam. Should I add cannabis?
Q: I’m on valproate. Is it safe to use CBD?
Q: Can cannabis cause seizures?
Q: Will cannabis affect my driving ability?
Epilepsy Support Resources
Epilepsy Foundation (epilepsy.com) is the leading national patient advocacy organization for people with epilepsy and seizure disorders. Their medical marijuana and epilepsy resource page on website is regularly updated and provides one of the most authoritative patient-facing summaries of the evidence.
Epilepsy Foundation Greater Pennsylvania (epilepsypa.org) provides local resources including support groups, educational events, and navigation assistance for PA patients.
Citizens United for Research in Epilepsy (CURE) (cureepilepsy.org) focuses on funding research into drug-resistant epilepsy and maintains patient resources on emerging treatments including cannabidiol.
NIH / NINDS – Epilepsy Information at ninds.nih.gov provides authoritative clinical information on epilepsy types, treatment options, and ongoing research.
NOTE: Epilepsy is one of the qualifying conditions where cannabis medicine has produced its most rigorous and transformative clinical evidence — the FDA approval of Epidiolex for three devastating epilepsy syndromes is a landmark in the history of cannabinoid medicine. For the much larger population of drug-resistant epilepsy patients who don’t have LGS, Dravet, or TSC, the real-world evidence for CBD is growing in a consistent direction, even while formal RCT data outside those three syndromes remains limited.
The PA MMJ card gives you legal access to CBD-dominant cannabis products through Pennsylvania’s dispensary system. Whether that access is the right choice depends on your specific epilepsy type, your current medications, your neurologist’s position, and what symptoms you are trying to address. For epilepsy more than any other PA qualifying condition, the answer to “should I get a MMJ card” requires a clinical conversation — not just a certification appointment.