If you live with ulcerative colitis or Crohn’s disease, you already know the daily reality of IBD, the unpredictable flares, the abdominal pain that interrupts sleep, the anxiety of managing symptoms around work and social life, the mounting medical visits, and in many cases the exhausting trial-and-error through medications that may only partially work or carry serious side effects of their own.
Pennsylvania’s medical marijuana program includes inflammatory bowel disease as an explicit qualifying condition. But the evidence landscape for cannabis in IBD has a nuance that matters enormously for setting realistic expectations and one that almost every cannabis website either misunderstands or omits entirely.
This page covers what actually qualifies, what the research shows for both ulcerative colitis and Crohn’s disease, the critical distinction between feeling better and the gut actually healing, drug interactions with the medications most IBD patients are already taking, and how to get your PA MMJ card.
Does IBD Qualify for Medical Marijuana in Pennsylvania?
Yes. Inflammatory bowel disease is an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016) and is recognized by the Pennsylvania Department of Health. Both major forms of IBD qualify:
- Ulcerative colitis (UC) — qualifies under the IBD condition
- Crohn’s disease (CD) — qualifies under both the IBD condition and its own separate qualifying condition entry
Pennsylvania is one of the few states that lists both IBD and Crohn’s disease as distinct qualifying conditions. This means patients with Crohn’s disease have two statutory pathways. In practice, this makes no functional difference to obtaining your MMJ card, a certifying physician can use either or both conditions on your certification but it reflects the legislature’s recognition that Crohn’s disease carries a distinct clinical profile.
There is no requirement that IBD be severe, treatment-resistant, or a specific stage of disease. A confirmed diagnosis of ulcerative colitis, Crohn’s disease, or another IBD diagnosis is sufficient.
- Source: Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Source: 28 Pa. Code Appendix A – Serious Medical Conditions
What Is IBD? UC vs. Crohn’s Disease — Why the Distinction Matters for Cannabis
Inflammatory bowel disease is an umbrella term for two distinct, immune-mediated chronic inflammatory conditions of the gastrointestinal tract. They share a treatment philosophy but differ significantly in their biology, location, and behaviour and the cannabis evidence, while overlapping, does not treat them identically.
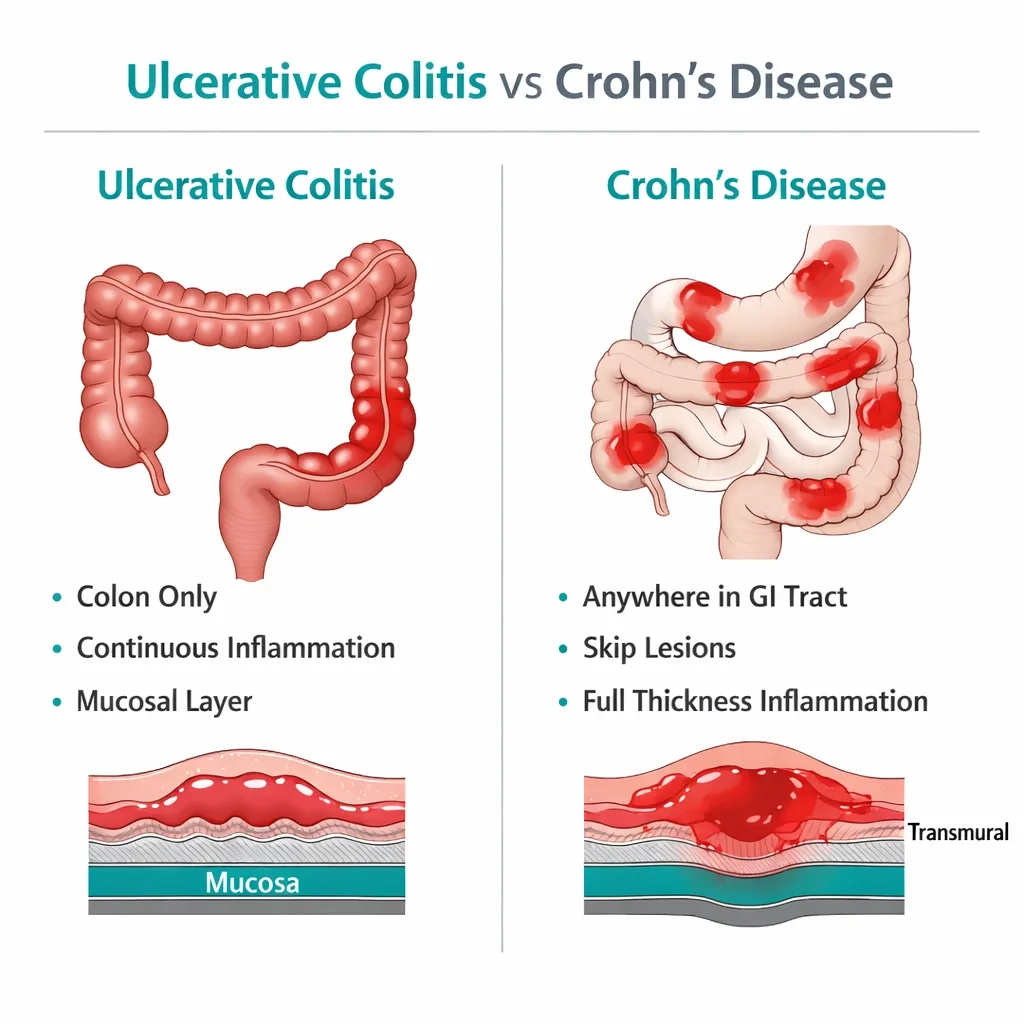
Ulcerative colitis (UC) is characterised by continuous, superficial inflammation confined to the colon’s mucosal lining, always starting at the rectum and extending proximally. Symptoms include bloody diarrhoea, urgency, tenesmus, and cramping. The disease course alternates between flares and remission. In severe or refractory UC, the ultimate surgical option is colectomy, removal of the colon.
Crohn’s disease (CD) can affect any part of the GI tract from mouth to anus, but most commonly the terminal ileum and colon. Unlike UC, Crohn’s involves transmural (full-thickness) inflammation, can create fistulas and strictures, and carries a high lifetime surgical rate. Up to 90% of Crohn’s patients have relapsing disease, and roughly 38% require surgery within ten years.
Both conditions share the core clinical burden that cannabis most directly addresses: abdominal pain, nausea, reduced appetite, diarrhoea, fatigue, sleep disruption, and anxiety related to chronic illness.
The Endocannabinoid System and the Gut: Why the Biology Makes Sense
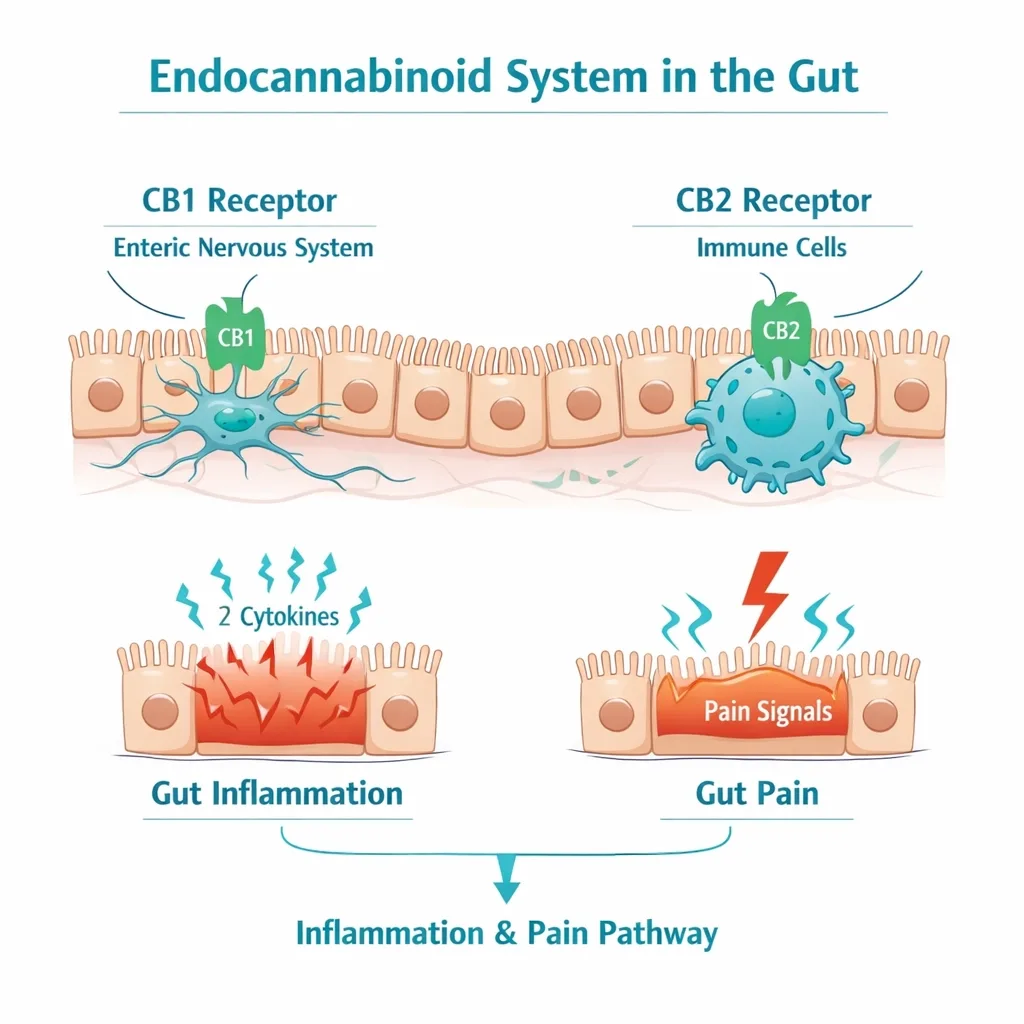
The gastrointestinal tract is one of the most cannabinoid receptor-dense organs in the body. CB1 receptors are abundant throughout the enteric nervous system, the gut’s own neural network, where they modulate pain signalling, motility, secretion, and visceral sensitivity. CB2 receptors are concentrated on immune cells in the gut lamina propria, where they regulate inflammatory cytokine production.
In IBD, the endocannabinoid system is dysregulated. Research has documented reduced endocannabinoid tone in the inflamed mucosa of both UC and CD patients, specifically, reduced levels of anandamide (AEA) and altered CB2 receptor expression in inflamed versus non-inflamed gut tissue. Restoring endocannabinoid tone is the theoretical basis for cannabis’s effects in IBD.
Preclinical evidence is compelling. In experimental colitis models, cannabinoid receptor agonists consistently reduce inflammation, decrease pro-inflammatory cytokine production (including TNF-α and IL-6), improve gut barrier function, and reduce visceral hyperalgesia. CB2-selective agonists appear particularly relevant for the inflammatory component without the psychoactive effects of CB1 activation.
The critical question is whether this preclinical biology translates into measurable disease modification in human trials and this is where the evidence picture becomes more nuanced than most cannabis websites acknowledge.
The Most Important Thing to Understand: Clinical vs. Endoscopic Response
This is the central nuance of the cannabis-IBD evidence base and the point most completely absent from competing medical marijuana websites. Understanding it is essential for setting appropriate expectations before pursuing a PA MMJ card for IBD.
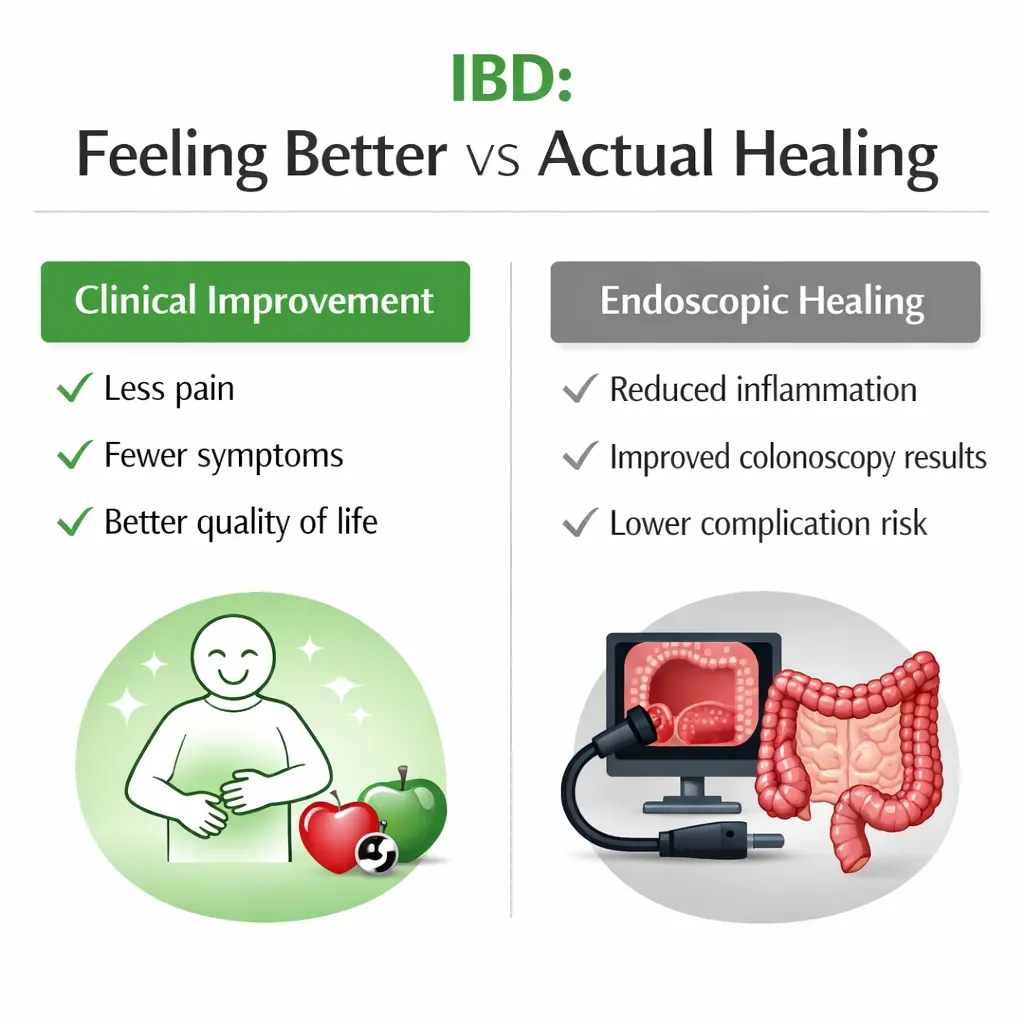
Clinical response means patients report feeling better: less pain, fewer bowel movements, improved quality of life. This is patient-reported.
Endoscopic response means the gut’s mucosal inflammation has actually healed, confirmed by colonoscopy, or by blood/stool inflammatory markers (C-reactive protein, fecal calprotectin). This is the objective, disease-modifying standard.
Modern IBD management aims for treat-to-target outcomes that include both clinical and endoscopic remission (sometimes called “mucosal healing”), because endoscopic remission predicts lower long-term complication rates, reduced surgery risk, and better quality of life.
Across almost every controlled study of cannabis in IBD, patients report meaningful clinical improvement but objective endoscopic and inflammatory marker data do not consistently follow. Patients feel better. Their colonoscopies often do not show corresponding mucosal healing.
This finding appeared clearly in the landmark 2021 Naftali randomised, placebo-controlled trial of cannabis in ulcerative colitis (published in PLoS ONE). THC-rich cannabis cigarettes significantly reduced the Lichtiger disease activity index in UC patients from 10.9 to 5 (compared to a smaller reduction of 11 to 8 in placebo, p=0.006 between groups). Quality of life improved. But Mayo endoscopic scores, C-reactive protein, and fecal calprotectin, the objective inflammation measures — did not change significantly between the cannabis and placebo groups. The gut’s subjective experience and its objective inflammation diverged.
The same clinical-not-endoscopic pattern appears across Crohn’s disease RCTs (including the Naftali 2013 and 2021 CBD trials) and is confirmed in the 2025 Brodaric scoping review of 40 IBD-cannabis studies: “RCTs of cannabinoids reported mild reductions in disease activity and variable endoscopic inflammation improvement.”
The overall conclusion of the 2022 Vinci meta-analysis of RCTs was that “cannabinoid supplementation as adjuvant therapy may increase the chances of success for standard therapy of Crohn’s disease, although evidence is still weak. On the other hand, its usage in ulcerative colitis is not to be recommended”, specifically as a disease-modifying agent.
What this means for PA patients: Cannabis in IBD works primarily as a symptom manager, not a disease modifier. It reduces the lived experience of IBD, pain, urgency, nausea, poor sleep, anxiety. It does not reliably reduce endoscopic inflammation, normalise inflammatory markers, or substitute for biologics, immunosuppressants, or 5-ASA agents in maintaining mucosal remission.
Understanding this framing prevents the dangerous scenario of feeling better on cannabis while the gut continues to deteriorate, an inflammation-symptom mismatch that can delay necessary escalation of medical treatment.
- Source: PLoS ONE – Cannabis is Associated with Clinical but Not Endoscopic Remission in Ulcerative Colitis: RCT (Naftali et al., 2021)
- Source: PubMed – Cannabinoids for Inflammatory Bowel Disease: A Scoping Review (Brodaric et al., 2025)
- Source: PMC – Cannabinoid Therapeutic Effects in IBD: Systematic Review and Meta-Analysis of RCTs (Vinci et al., 2022)
What the Research Shows: Condition by Condition
Ulcerative Colitis
The RCT evidence — four trials included in the 2024 Kumar meta-analysis, shows statistically significant improvements in disease activity indices and quality of life in the cannabinoid group versus placebo (SMD -1.78 for disease activity; SMD -1.70 for QoL). These are meaningful effects on how patients feel. The caveat from that same meta-analysis: “their impact on endoscopic indices was not statistically significant.”
The most recent and largest RCT (Naftali 2021) specifically captured the clinical-not-endoscopic split in 32 active UC patients. Clinical activity scores improved significantly in the cannabis group. Endoscopic and inflammatory biomarker data did not.
Real-world data over 18 months comes from the UK Medical Cannabis Registry (UKMCR), which published two analyses of IBD patients prescribed cannabis products. The 2024 updated analysis of 116 IBD patients (including 38 with UC) followed over 18 months found sustained improvements in IBD-specific quality of life (SIBDQ scores), sleep quality, and overall health-related QoL.
In the UC subgroup specifically, improvements were seen in IBD-specific symptoms, sleep, and pain/discomfort but not in anxiety measures or general HRQoL at the same statistical threshold as the Crohn’s patients. Twenty-five percent of all IBD patients achieved a minimal clinically important difference in their SIBDQ score at 18 months.
- Source: JHSMR – Therapeutic Effects of Cannabinoids on Ulcerative Colitis: Systematic Review and Meta-Analysis of RCTs (Kumar et al., 2024)
- Source: PubMed – UK Medical Cannabis Registry: Updated Analysis for IBD over 18 Months (2024)
Crohn’s Disease
Crohn’s disease has the more developed cannabinoid evidence base within IBD, though the same clinical-not-endoscopic pattern applies.
The pioneering Israeli work by Naftali et al. established the clinical signal. An observational study of 30 CD patients found average Harvey-Bradshaw Index (HBI) scores dropping from 14 to 7 with cannabis use, with improvement sustained over a median of two years.
A subsequent double-blind RCT of 21 CD patients unresponsive to other treatments found that cannabis cigarettes produced significantly better CDAI (Crohn’s Disease Activity Index) scores versus placebo (152 vs 306 at study end, p<0.05), without changes in CRP or other inflammatory markers.
The 2025 Brodaric scoping review also identified meaningful population-level associations in cohort data: cannabis users with IBD were significantly less likely to require parenteral nutrition (3.0% vs 4.7%), gastrointestinal surgery (43.9% vs 50.4%), and colectomy (4.4% vs 9.7%). These are striking figures that deserve cautious interpretation, the cannabis users in these datasets are self-selected and likely a healthier cohort to begin with. The association does not establish causation.
The 2024 UKMCR analysis of 78 CD patients showed improvements in IBD-specific QoL, anxiety (GAD-7), sleep quality, and general health-related QoL sustained over 18 months, a more comprehensive improvement profile than the UC subgroup.
A 2025 Irish Journal of Medical Sciences meta-analysis of IBD cannabis RCTs (cited in this project’s Crohn’s disease page) found higher rates of clinical remission in cannabis-treated patients compared to placebo. Across studies, THC alone or THC with CBD produced significant CDAI reductions of over 100 points, a clinically meaningful threshold.
- Source: Journals.Sagepub – Cannabinoids for Inflammatory Bowel Disease: A Scoping Review (Brodaric et al., 2025)
- Source: PubMed – UK Medical Cannabis Registry: Updated Analysis for IBD over 18 Months (2024)
Quality of Life, Pain, Sleep, and Anxiety — The Strongest Clinical Case
Across both UC and CD, and across RCT and real-world evidence, the most consistent and robust finding is improvement in patient-reported quality of life outcomes. This includes:
- Abdominal pain: Consistent reductions across studies. CB1 receptor activation in the enteric nervous system reduces visceral pain signalling — this is the most mechanistically direct effect of cannabis in IBD.
- Nausea: THC is a well-documented antiemetic via brainstem CB1 receptors; nausea is a common IBD symptom and a side effect of several IBD medications.
- Sleep: Both the 2023 and 2024 UKMCR datasets showed significant sleep quality improvements in IBD patients on cannabis. This is clinically meaningful given the well-documented sleep disruption in active IBD.
- Anxiety: IBD carries a substantially elevated anxiety burden. The 2023 UKMCR analysis showed GAD-7 improvements in CD patients at three months. This may be one of the strongest real-world use cases for cannabis in IBD.
- Appetite and nutrition: THC’s appetite-stimulating properties are directly relevant for CD patients with weight loss, malnutrition, or treatment-related appetite suppression.
For PA patients, this means the realistic and clinically sound reason to pursue a PA MMJ card for IBD is symptom management and quality of life, not replacing disease-modifying therapy or expecting colonoscopy results to improve.
The Surgery-Association Confound: A Data Point PA Patients Should Know
The 2025 Brodaric scoping review included an important finding from cohort data: patients prescribed cannabis for IBD were significantly more likely to have had prior IBD surgery (14.5% vs 4.7%), be on corticosteroids (18.1% vs 10.4%), use opioids (27.7% vs 6.4%), and report lower quality of life than non-cannabis users.
This does not mean cannabis causes surgery or worsening disease. It means that cannabis use in IBD is heavily concentrated in the sickest patients, those with refractory disease, multiple prior treatments, and significant surgical history. They are turning to cannabis because conventional options have not been adequate.
This context explains why some Canadian long-term survey data found increased surgery rates among cannabis users, the causality runs the other way. These patients were already on a trajectory toward surgery, and cannabis was a late-stage symptom management tool, not a cause of deterioration.
The practical implication: The patient profile most likely to benefit from cannabis in IBD is one with refractory symptoms, adequate conventional treatment in place, and realistic expectations about symptom relief rather than disease modification.
- Source: PubMed – Cannabinoids for Inflammatory Bowel Disease: A Scoping Review (Brodaric et al., 2025)
Drug Interactions: Cannabis and IBD Medications
The drug interaction profile of cannabis in IBD is largely reassuring for the most commonly used medications but has specific areas requiring attention. This section, absent from every competing PA MMJ page, covers the actual medications IBD patients take.
5-Aminosalicylates (5-ASA): Mesalamine, Sulfasalazine — LOW RISK
Mesalamine (Asacol, Pentasa, Lialda, Apriso) and sulfasalazine are the backbone maintenance therapies in UC. These medications are not significantly metabolised through CYP3A4 or other cannabinoid-interacting pathways. Published evidence to date does not identify clinically significant pharmacokinetic interactions between cannabis and 5-ASA agents. These are among the lowest-risk IBD medications for cannabis co-administration.
Biologics (TNF Inhibitors, Vedolizumab, Ustekinumab) — REASSURINGLY LOW RISK
This is the critical finding for the many IBD patients on advanced biologic therapy. Infliximab (Remicade), adalimumab (Humira), vedolizumab (Entyvio), ustekinumab (Stelara), and related biologics are monoclonal antibodies. Monoclonal antibodies are metabolised by proteolytic catabolism, not by CYP450 enzymes. They do not interact with the cannabinoid CYP pathway.
A review of rheumatology drug interactions with cannabinoids, directly applicable to shared IBD medications, found “no predictable interactions between cannabinoids and adalimumab, methotrexate, hydroxychloroquine, sulfasalazine, mycophenolate mofetil, mesalazine, etanercept, abatacept, infliximab or rituximab.” This is one of the most reassuring statements in the IBD-cannabis interaction landscape.
For the substantial proportion of IBD patients on biologic monotherapy, the cannabis drug interaction risk is low. Patients on vedolizumab or ustekinumab, the newer gut-selective or IL-12/23-blocking biologics, share this same low interaction profile.
Thiopurines: Azathioprine, 6-Mercaptopurine — GI MOTILITY CONCERN
Azathioprine (Imuran) and 6-mercaptopurine are immunomodulators used in IBD both as monotherapy and in combination with biologics. These drugs are not primarily CYP3A4 substrates, so the direct pharmacokinetic interaction concern is lower than with many other immunosuppressants.
However, THC has a documented effect on GI motility, it slows motility by activating CB1 receptors in the enteric nervous system. This same mechanism that reduces cramping and diarrhoea can also alter the GI absorption of antimetabolite drugs like azathioprine. Delayed gastric emptying and altered small intestinal transit may affect how much azathioprine is absorbed and when peak blood levels occur.
The clinical significance of this is not well-characterised and is unlikely to represent a dangerous interaction for most patients. However, patients on azathioprine experiencing unexplained changes in their IBD control or azathioprine metabolite levels (6-TGN levels on standard therapeutic drug monitoring) after starting cannabis should discuss this with their gastroenterologist.
Corticosteroids: Prednisone, Budesonide — MODERATE INTERACTION POSSIBLE
Corticosteroids are commonly used for IBD flare induction. THC can inhibit CYP3A4, the primary enzyme metabolising many corticosteroids, potentially increasing corticosteroid plasma levels at standard doses. The interaction is not well-characterised clinically for IBD-specific corticosteroid doses but warrants mention for patients on prednisone or other systemic steroids.
Budesonide (Entocort, Uceris), the locally-acting corticosteroid preferred in IBD for its lower systemic absorption, carries less systemic interaction risk. Patients adding cannabis during a corticosteroid taper should be alert for amplified steroid effects.
JAK Inhibitors: Tofacitinib, Upadacitinib, Filgotinib — VARIABLE RISK
JAK inhibitors are a newer oral small-molecule class for moderate-to-severe IBD. Tofacitinib (Xeljanz) is metabolised by CYP3A4, meaning that THC’s CYP3A4 inhibitory activity could theoretically increase tofacitinib plasma levels.
Upadacitinib (Rinvoq) similarly has partial CYP3A4 metabolism. Given the significant safety monitoring requirements for JAK inhibitors (including infection risk, cardiovascular risk, and malignancy surveillance), any potential increase in plasma levels warrants discussion with the treating gastroenterologist before adding cannabis.
Opioids — OPIOID-SPARING POTENTIAL, SEDATION CAUTION
A significant proportion of IBD patients with refractory pain are on opioids. Cannabis and opioids have pharmacodynamic synergy — combined, they produce greater analgesia and greater sedation than either alone. This dual-effect means cannabis may allow reduced opioid doses for pain management (the opioid-sparing effect, which has its own evidence base), while simultaneously creating a risk of excessive sedation at doses of each drug that were previously tolerable individually.
IBD patients transitioning from opioids toward cannabis for pain management should do so with gradual adjustment of opioid doses under physician supervision, not abrupt discontinuation.
PA Dispensary Product Guidance for IBD
For abdominal pain and cramping
THC-dominant oral tinctures or capsules provide the most sustained relief through the gastrointestinal tract. Oral products taken 30–60 minutes before meals or at times of anticipated pain have the most consistent effect. Start low (2.5–5 mg THC equivalent) and titrate slowly, as GI bioavailability of oral cannabis is variable. Taking cannabis products with a fat-containing food improves absorption substantially.
For nausea
Low-dose THC tinctures taken sublingually have a faster onset than capsules for acute nausea. CBD alone does not reliably reduce nausea in the same way; THC-dominant or balanced products are more appropriate for this target.
For sleep disruption
Moderate THC doses (5–10 mg equivalent) taken 1–2 hours before sleep via oral formats are commonly effective. Higher THC doses can cause morning grogginess or next-day anxiety in some patients.
For anxiety related to IBD
CBD-dominant products at meaningful doses (20–40 mg CBD) have the most evidence for anxiety relief in the broader research literature. For IBD patients whose primary goal is anxiety management rather than GI symptom control, CBD-dominant products with low THC are appropriate.
For active flare management
Do not attempt to manage an IBD flare with cannabis while stopping or reducing disease-modifying medications. Cannabis addresses the symptom experience of a flare (pain, urgency, nausea) but does not treat the underlying mucosal inflammation driving it. Continue prescribed IBD medications during flares; cannabis is adjunctive.
For patients on biologics
Product selection is relatively unrestricted by interaction concerns. Start with standard low doses and titrate based on symptom response.
For patients on tofacitinib or other JAK inhibitors
Discuss cannabis co-administration with your gastroenterologist before starting, particularly if using THC-dominant products at moderate or higher doses.
How to Get Your Pennsylvania Medical Marijuana Card for IBD
Step 1 — Notify Your Gastroenterologist
Before or after getting your PA MMJ card, inform your gastroenterologist that you are using cannabis. This is important for two specific IBD reasons. First, your GI doctor needs to know because cannabis use can mask symptom worsening from ongoing mucosal inflammation, if they are monitoring you primarily by symptoms rather than fecal calprotectin or colonoscopy, cannabis symptom relief could lead to delayed recognition of a worsening flare. Second, if you are on azathioprine or a JAK inhibitor, your GI doctor can advise on monitoring needs.
Step 2 — Physician Certification (Telehealth)
Schedule a telehealth appointment with a PA DOH-registered medical marijuana physician. The evaluation typically takes 10–15 minutes. Bring your IBD diagnosis documentation (recent records, current medications list including every IBD drug, dose, and frequency). The certifying physician can certify under IBD, Crohn’s disease (if applicable), or both simultaneously.
Step 3 — State Registration
After certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com) with your certification, a valid PA driver’s license or state-issued ID, and the $50 annual registration fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 4 — Dispensary Visit
At the dispensary, tell the pharmacist you have IBD and describe your primary symptom targets. Bring your IBD medication list. A dispensary pharmacist can suggest appropriate product formats and dose ranges for your symptom profile. If you are on a JAK inhibitor, mention it specifically.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Anxiety Disorder
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: I have ulcerative colitis, not Crohn’s. Does IBD still qualify me?
Q: Will cannabis replace my biologic or immunosuppressant?
Q: My gastroenterologist told me cannabis isn’t a treatment for IBD. Are they right?
Q: I’m on infliximab (Remicade). Do I need to worry about drug interactions?
Q: Cannabis helped my symptoms so much I skipped my colonoscopy. Should I?
Q: I have Crohn’s disease. Should I certify under IBD, Crohn’s disease, or both?
IBD Support Resources in Pennsylvania
Crohn’s & Colitis Foundation (crohnscolitisfoundation.org) is the leading US patient advocacy and research organisation for IBD. Their website provides patient education on both conditions, treatment options, and clinical trial opportunities. The Philadelphia Chapter and Pittsburgh Chapter both serve Pennsylvania patients with local support groups and educational events.
Penn Medicine IBD Program and UPMC IBD Program are among the academic centres in Pennsylvania providing specialist IBD care. Patients seeking IBD specialist management for complex or refractory disease can seek referrals through either academic health system.
IBD Relief (ibdrelief.com) is a UK-based but internationally relevant patient education platform with high-quality, evidence-based guides on IBD medications, combination therapy, and lifestyle management including cannabis.
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) at niddk.nih.gov provides authoritative patient-facing information on IBD pathophysiology and treatment.
NOTE: IBD is one of the qualifying conditions where the evidence for cannabis most clearly splits into two distinct tracks: robust evidence for symptom relief and quality of life improvement, and weak-to-absent evidence for disease modification or mucosal healing. For Pennsylvania patients with UC or Crohn’s disease, the PA MMJ card represents legitimate access to a tool that can meaningfully reduce the daily symptom burden — pain, urgency, nausea, sleep disruption, anxiety, while conventional IBD therapy continues to address the underlying gut inflammation that cannabis alone cannot reliably reach.
That combination — cannabis for the lived experience, disease-modifying therapy for the biology, is the honest and evidence-based framework for using a PA MMJ card well when you have inflammatory bowel disease.