
Anxiety disorders are the most common mental health condition in the United States. They affect approximately 40 million American adults every year — roughly 19% of the adult population — and nearly one in three Americans will experience an anxiety disorder at some point in their lifetime. Behind those numbers are real people: lying awake at 3 a.m., unable to enter a room full of people, gripped by a racing heartbeat that won’t stop, consumed by worry that feels impossible to control.
Pennsylvania added anxiety disorders to its medical marijuana qualifying conditions list on July 20, 2019 — and the decision transformed the entire program. By 2021, anxiety disorders had become the single most common reason Pennsylvanians were certified for medical marijuana, accounting for more than 60% of all certifications. No other condition comes close.
But most PA MMJ websites serving anxiety patients do something irresponsible: they either oversell cannabis as an anxiety cure or fail to explain the single most important fact in this entire field — that high-dose THC can make anxiety significantly worse. The very same plant that can relieve anxiety in one person can trigger a panic attack in another. Understanding why, and how to navigate it, is the difference between cannabis helping your anxiety and making it worse.
This page gives you the complete picture: what qualifies in Pennsylvania, all the types of anxiety disorders covered, the biological mechanism through which cannabis affects anxiety, the honest evidence for CBD and for THC respectively, the dose-dependence rule that everyone using cannabis for anxiety must understand, product guidance grounded in the science, drug interaction considerations with common anxiety medications, and a clear step-by-step path to your PA MMJ card.
Does Anxiety Disorder Qualify for Medical Marijuana in Pennsylvania?
Yes — anxiety disorders became a qualifying condition on July 20, 2019, and quickly became the #1 qualifying condition in Pennsylvania’s MMJ program.
Anxiety disorders are an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act, as approved by the Pennsylvania Department of Health (PA DOH). A confirmed diagnosis of any recognized anxiety disorder qualifies a Pennsylvania resident for a medical marijuana card.
The PA DOH Secretary’s Guidance When Anxiety Was Added
When former PA Health Secretary Rachel Levine approved anxiety disorders as a qualifying condition in July 2019, she issued specific guidance that remains relevant today. She stated:
- Medical marijuana is NOT first-line treatment for anxiety disorders and should not replace traditional therapies
- Cannabis should be used in conjunction with conventional treatments when recommended by a physician
- Short-term use of medical marijuana with low THC and high CBD content has been shown most effective for anxiety disorders
- Medical marijuana is NOT recommended for children, adolescents, or pregnant women with anxiety disorders
This guidance — embedded in the original qualifying decision — is more clinically accurate than most PA MMJ websites acknowledge. It reflects the genuine state of the evidence: CBD at appropriate doses shows anxiolytic promise, high THC is a real risk, and cannabis is most appropriate as an adjunct to, not a replacement for, evidence-based anxiety treatment.
Which Anxiety Disorders Qualify?
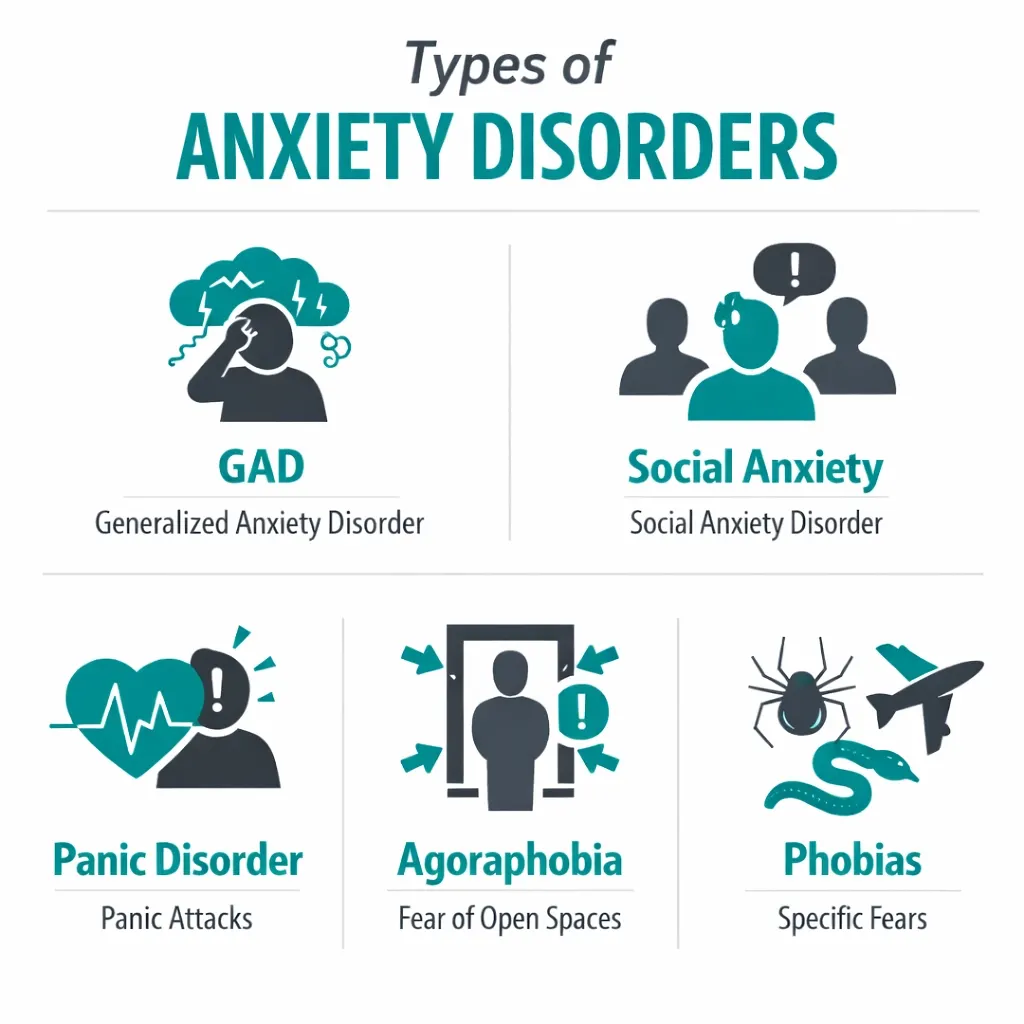
Pennsylvania’s qualifying language covers ‘anxiety disorders’ as a category, which encompasses the full spectrum of clinically recognized anxiety diagnoses under the DSM-5. All of the following qualify:
- Generalized Anxiety Disorder (GAD) — chronic, excessive worry about multiple life domains
- Social Anxiety Disorder (SAD) — intense fear of social situations and scrutiny
- Panic Disorder — recurrent unexpected panic attacks with persistent worry about future attacks
- Agoraphobia — fear and avoidance of situations where escape might be difficult during a panic attack
- Specific Phobias — intense fear of specific objects or situations causing significant functional impairment
- Separation Anxiety Disorder — excessive fear concerning separation from attachment figures
- Selective Mutism — consistent failure to speak in specific social situations
- Adjustment Disorder with Anxious Mood — anxiety developing in response to identifiable stressor
Conditions that overlap with anxiety and may qualify under either anxiety disorders or a separate qualifying condition include:
- PTSD (Post-Traumatic Stress Disorder) — Pennsylvania lists PTSD as a separate qualifying condition; patients with PTSD may qualify under either category
- OCD (Obsessive-Compulsive Disorder) — closely related to anxiety disorders; patients should discuss diagnosis-specific qualifying with the certifying physician
Sources:
- Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- PA Code Appendix A – Serious Medical Conditions
- Pennsylvania Bulletin – Notice of Addition of Anxiety Disorders to Qualifying Conditions (Vol. 49, No. 29)
Anxiety Disorders in Context: Who This Page Is Written For
The scale of anxiety disorders in the United States is staggering — and Pennsylvania patients are not alone in seeking alternatives to conventional treatment.
According to the National Institute of Mental Health (NIMH), an estimated 19.1% of U.S. adults have any anxiety disorder in a given year, and 31.1% will experience an anxiety disorder at some point in their lives. Among individual disorders: Generalized Anxiety Disorder (GAD) affects 6.8 million adults; Social Anxiety Disorder affects 15 million adults; Panic Disorder affects 6 million adults; and Specific Phobias affect 19.3 million adults. Women are nearly twice as likely as men to be affected by anxiety disorders across most subtypes.
Despite this prevalence, treatment gaps are substantial. For GAD specifically, only 43.2% of affected adults receive any treatment. For Social Anxiety Disorder, 36% of people report experiencing symptoms for 10 or more years before seeking help. Conventional treatments — SSRIs, SNRIs, buspirone, benzodiazepines, and psychotherapy — are effective for many patients but leave a significant portion inadequately treated or dealing with side effects that compromise their quality of life.
It is within this treatment gap that most Pennsylvanians with anxiety disorders are seeking a PA MMJ card. Understanding what cannabis realistically can and cannot do for anxiety — and how to use it safely — is the purpose of this page.
Sources:
- NIMH – Any Anxiety Disorder Statistics
- NIMH – Generalized Anxiety Disorder Statistics
- ADAA – Anxiety Disorders: Facts & Statistics
The Endocannabinoid System and Anxiety: The Biology
To understand why cannabis affects anxiety — and why it can both relieve and worsen it — requires understanding how the endocannabinoid system (ECS) is involved in fear and anxiety regulation.
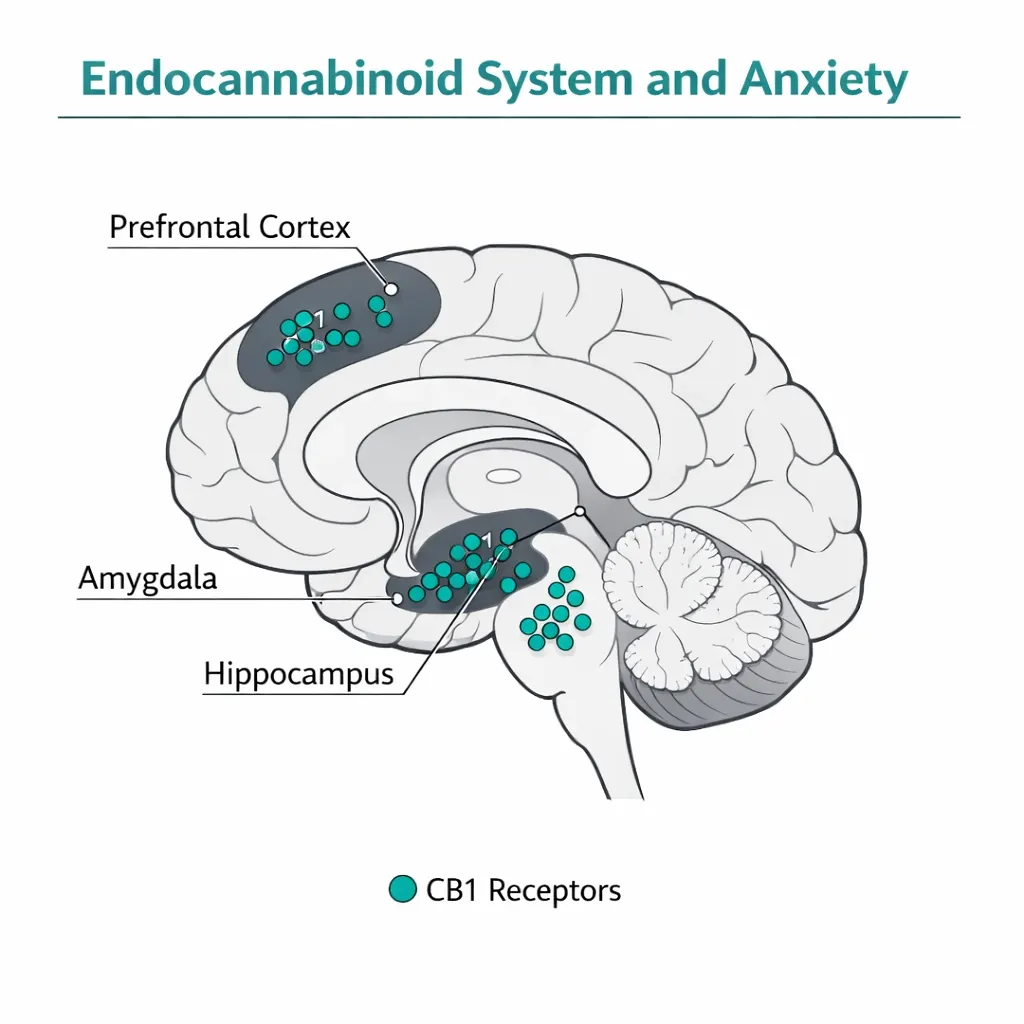
The ECS plays a central role in the neural circuits that process fear and anxiety. CB1 receptors are distributed throughout the brain’s anxiety circuit: the amygdala (the brain’s fear center), the prefrontal cortex (the region that regulates emotional responses), the hippocampus (involved in contextual fear memory), and the hypothalamus (the stress response hub). Endocannabinoids — anandamide and 2-AG — are released in response to stress and act retrograde to dampen the activity of anxiety-driving neural circuits.
In other words, the ECS is the brain’s built-in anxiety management system. Research has shown that people with anxiety disorders often have reduced endocannabinoid tone — lower anandamide levels and reduced CB1 receptor activity in fear-processing regions. This is the biological basis for why cannabis may be therapeutically relevant for anxiety: external cannabinoids can modulate the same system the brain uses to regulate fear.
THC and the Amygdala: Why High Doses Cause Anxiety
THC (delta-9-tetrahydrocannabinol) is a partial agonist at CB1 receptors. Its effects on anxiety are dose-dependent and anatomically complex:
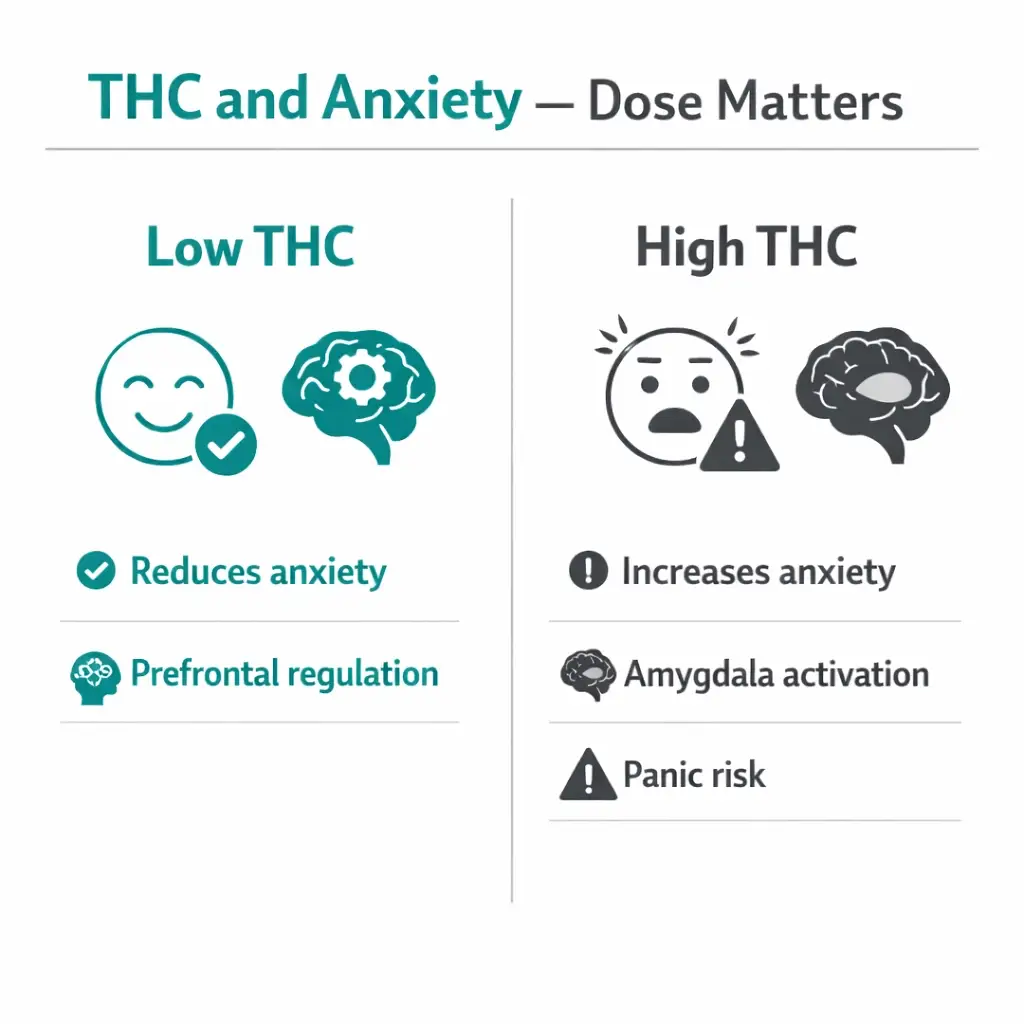
- At low doses, THC activates CB1 receptors in the prefrontal cortex and limits amygdala reactivity, producing anxiolytic (anxiety-reducing) effects
- At higher doses, THC excessively activates CB1 receptors in the amygdala itself, which paradoxically increases amygdala activity and drives anxiogenic (anxiety-inducing) responses including racing heart, paranoia, and panic
A neuroimaging study published in Scientific Reports directly documented this: the anxiogenic effects of THC in humans were specifically related to its effect on neural activity in the amygdala and to the local density of CB1 receptors in that region. This is not a subjective observation — it is a measurable biological mechanism. The dose-dependence is real, the individual variability is real, and the amygdala is the anatomical explanation for both.
This is the foundational reason why high-THC products are not the evidence-supported choice for anxiety patients.
CBD and Serotonin: Why It Works Differently
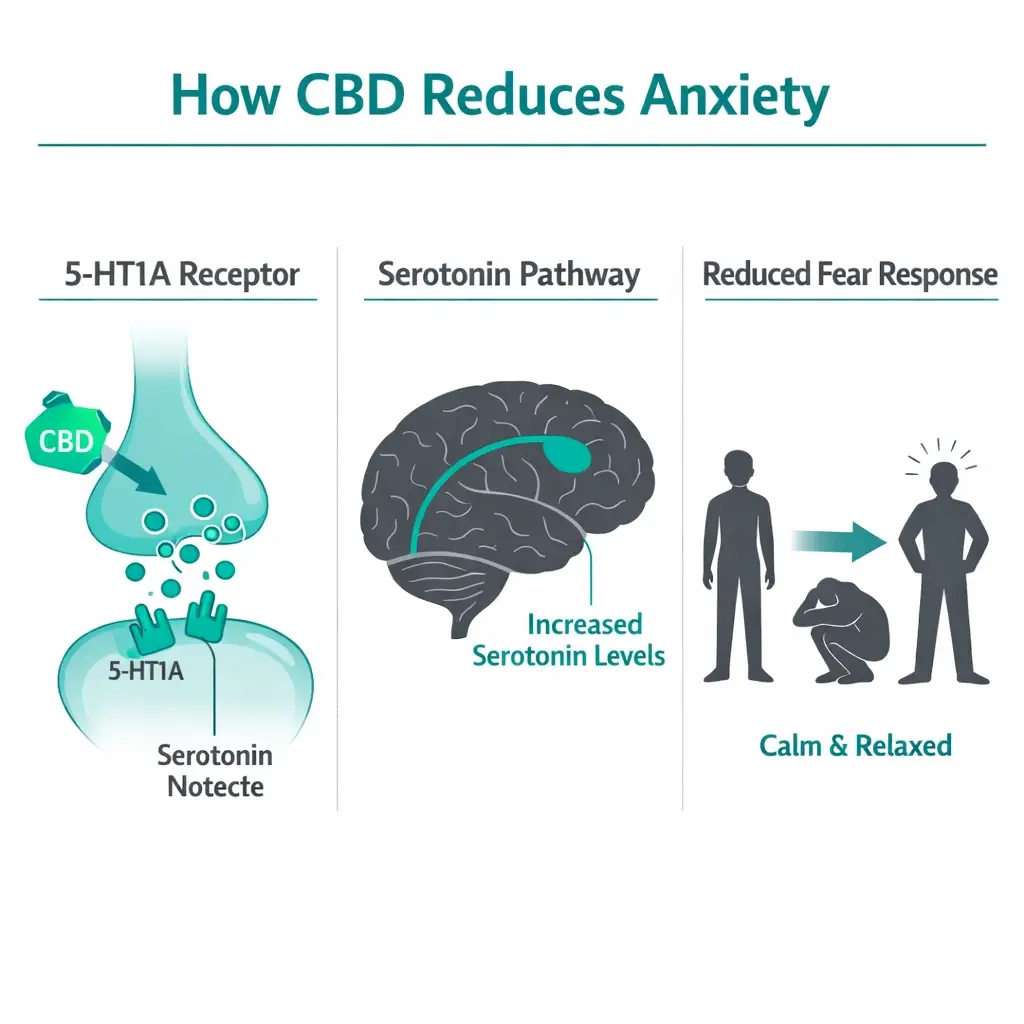
CBD (cannabidiol) does not act primarily through CB1 receptors. Its anxiolytic mechanism is fundamentally different from THC and does not carry THC’s anxiogenic risk at higher doses. CBD’s anxiety-relevant mechanisms include:
- 5-HT1A partial agonism: CBD partially activates serotonin receptor 5-HT1A, the same receptor targeted by buspirone (an approved anxiolytic medication). This is the primary mechanism through which CBD reduces anxiety, and it mirrors the mechanism of existing pharmacological treatments.
- Negative allosteric modulation of CB1 receptors: CBD modifies CB1 receptor activity in a way that may counteract THC’s anxiogenic effects. This is why CBD-dominant products with low THC consistently show better anxiety outcomes than high-THC products.
- TRPV1 activation: Reduces sensitivity to aversive stimuli
- Anandamide reuptake inhibition: Increases the brain’s own endocannabinoid tone, essentially supporting the system that is often deficient in anxiety disorders
CBD does not produce the psychoactive high associated with THC, does not cause dependence, and does not have abuse liability. These properties make it pharmacologically suitable for anxiety management in a way that high-THC products are not.
Sources:
- Scientific Reports – Acute Induction of Anxiety in Humans by THC Related to Amygdalar CB1 Receptors
- PMC – THC, CBD, and Anxiety: A Review of Recent Findings (2022)
- PMC – Cannabis and Anxiety: A Critical Review (Med Cannabis Cannabinoids, 2024)
The Most Important Rule for Cannabis and Anxiety: Dose Dependence
The Dose-Dependence Rule: The Single Most Critical Fact for Anxiety Patients
Cannabis has a biphasic, dose-dependent relationship with anxiety. Low doses of THC are anxiolytic (reduce anxiety). High doses of THC are anxiogenic (cause or worsen anxiety). This is established in multiple systematic reviews, neuroimaging studies, and clinical trials. It is not controversial. Every anxiety patient using cannabis must understand this rule before starting.
1. Low THC dose → anxiety reduction through prefrontal cortex CB1 activation
2. High THC dose → anxiety increase, panic, paranoia through amygdala CB1 overactivation
3. CBD at all studied doses → anxiolytic (not dose-dependent in the same way; does not cause anxiety at high doses)
4. The threshold between anxiolytic and anxiogenic THC differs significantly between individuals
This dose-dependence is why the PA DOH Secretary specifically recommended ‘low THC, high CBD’ products when anxiety was added as a qualifying condition. It is why most research in anxiety disorders uses CBD rather than THC. And it is why a patient who uses high-potency THC products for anxiety and finds their symptoms worsen is not having an unusual experience — they are encountering a well-documented pharmacological reality.
Sources:
- PMC – Cannabis and Anxiety: A Critical Review (Med Cannabis Cannabinoids, 2024)
- Psychiatric Services – Evidence for Use of Cannabinoids in Mood Disorders, Anxiety Disorders, and PTSD
What the Clinical Research Shows: CBD and Anxiety
The evidence base for CBD in anxiety disorders has grown substantially in recent years. Multiple systematic reviews, meta-analyses, and clinical trials have evaluated CBD’s anxiolytic effects. Here is what the research actually shows.
The 2024 Meta-Analysis: Significant Effect Across Anxiety Disorders
A systematic review and meta-analysis published in Psychiatry Research (Han et al., 2024, Stanford University and co-authors) analyzed 8 eligible studies out of 1,550 screened, encompassing 316 participants. The meta-analysis found a substantial, statistically significant impact of CBD on anxiety with a considerable effect size (Hedges’ g = -0.92, 95% CI -1.80 to -0.04). The review specifically addressed GAD, Social Anxiety Disorder (SAD), and PTSD, and concluded that CBD shows meaningful anxiolytic effects across multiple anxiety disorder subtypes.
The 2024 Systematic Review of RCTs
A separate systematic review of randomized controlled trials published in Life (MDPI, 2024) searched three databases for all RCTs of CBD in anxiety disorders published between 2013 and 2023, identifying 11 eligible studies. The review confirmed CBD’s anxiolytic mechanism through 5-HT1A receptor partial agonism and CB1 negative allosteric modulation. It concluded that CBD shows potential as an anxiolytic through a mechanism that may specifically attenuate the anxiogenic effects of THC — explaining why CBD-dominant or CBD-only products consistently outperform high-THC products in anxiety research.
Social Anxiety Disorder: Neuroimaging Evidence
Crippa et al. conducted a neuroimaging study of CBD in patients with generalized Social Anxiety Disorder. CBD administration produced significant anxiolytic effects compared to placebo, with neuroimaging confirming activity changes in the exact brain regions involved in anxiety processing — the limbic and paralimbic cortex. This was a landmark study because it provided biological confirmation of CBD’s mechanism, not just self-report data.
GAD Real-World Study: 4-Week CBD Results
A quasi-randomized study published in Cannabis and Cannabinoid Research (2024, reported by NORML) examined individuals with generalized anxiety symptoms who used CBD-dominant cannabis 3–4 days per week. Results: participants reported reduced anxiety and improved symptoms over the study period. The CBD-dominant strain was associated with the greatest reduction in anxiety-related states both acutely and over four weeks. The study authors concluded that CBD-dominant cannabis may translate acute anxiolytic effects into longer-term anxiety reductions in naturalistic use.
Double-Blind RCT: CBD vs. Placebo in Mild-Moderate Anxiety
A multicenter, double-blind RCT (ScienceDirect, 2024) evaluated nanodispersible CBD oral solution in mild-to-moderate anxiety subjects. Primary outcomes (GAD-7 and HAM-A scales) and secondary outcomes (CGI, PHQ-9, PSQI) all showed statistically significant improvement in the CBD group compared to placebo (p < 0.0001). This was one of the most rigorous trials to date showing CBD’s efficacy for anxiety disorders.
Open-Label Study at McLean Hospital (2025)
A 2025 open-label pilot study at McLean Hospital enrolled 12 patients meeting DSM-5 criteria for current generalized anxiety disorder and administered a hemp-derived, full-spectrum, high-CBD sublingual solution (30 mg/day) for 6 weeks. The study found improvements in anxiety severity, supported by clinical outcome measures. While open-label design limits conclusions, this study is notable for using real-world hemp-derived CBD products similar to those available in PA dispensaries.
Evidence Summary: CBD and Anxiety Disorders
Multiple systematic reviews, meta-analyses, and controlled trials demonstrate that CBD has clinically meaningful anxiolytic effects in GAD, Social Anxiety Disorder, and related conditions. The effect is primarily mediated through serotonin (5-HT1A) receptor agonism, not CB1 activation. CBD does not cause anxiety at higher doses. The evidence for CBD in anxiety is substantially stronger than for THC, and stronger than most PA MMJ websites acknowledge.
What the Research Shows: THC and Anxiety — The Honest Picture
The THC and anxiety evidence deserves its own honest section because it is where many patients make decisions that worsen their condition. The evidence is clear and should be stated directly.
Multiple systematic reviews and experimental studies confirm that:
- Acute THC administration consistently produces anxiogenic effects in controlled laboratory settings, particularly at higher doses, affecting a significant minority (approximately 33%) of healthy participants
- High-potency, high-THC cannabis products are associated with greater anxiety and panic in observational data
- Regular, heavy cannabis use (predominantly high-THC products) is associated with increased rates of anxiety disorders in longitudinal studies, though causality is complicated by self-medication
- Daily cannabis use is associated with increased anxiety symptoms in some population-level studies
The Population-Level Concern Every Anxiety Patient Should Know
A major national study cited by the National Academies of Sciences, Engineering, and Medicine found that regular cannabis use is likely to increase the risk for developing social anxiety disorder. This finding does not mean cannabis cannot help anxiety — it means that unguided, high-frequency, high-THC use likely makes anxiety disorders worse on average, even if some individuals benefit. This is why product selection, dosing, and medical guidance are not optional for anxiety patients.
The self-medication hypothesis offers important context: multiple studies have found that 55–89% of people with cannabis use disorder who also have anxiety disorders report that their anxiety symptoms began before their cannabis use, suggesting they began using cannabis to manage pre-existing anxiety. This supports the idea that the relationship is bidirectional — anxiety drives cannabis use, and high-THC cannabis use can worsen anxiety — rather than simply causal in one direction.
Sources:
- PMC – THC, CBD, and Anxiety: A Review of Recent Findings (2022)
- PMC – Cannabis and Anxiety: A Critical Review (2024)
- PMC – The Impact of CBD Treatment on Anxiety Disorders: Systematic Review of RCTs (2024)
- ScienceDirect – Therapeutic Potential of CBD in Anxiety Disorders: Systematic Review and Meta-Analysis (2024)
- NORML – Clinical Trial: Cannabis Consumption Associated with Reduced Anxiety (2024)
PA Dispensary Product Selection for Anxiety: Evidence-Based Guidance

This is the section that most PA MMJ websites skip. Product selection for anxiety disorders is more evidence-driven and more consequential than for almost any other qualifying condition. Choosing the wrong product can worsen the very condition you are trying to treat.
The Evidence-Based Product Hierarchy for Anxiety Disorders
| Product Type | Evidence & Guidance |
|---|---|
| CBD-dominant (10:1 CBD:THC or higher) | Strongest evidence base. CBD’s anxiolytic mechanism is well-established through 5-HT1A agonism. No anxiogenic risk at higher doses. Appropriate for daytime use. First choice for most anxiety patients, especially those new to cannabis. |
| Balanced THC:CBD (1:1 or 2:1 CBD:THC) | Moderate evidence. The CBD component may partially offset THC’s anxiogenic effects. Some patients find this ratio provides better sleep and additional symptom relief. Not appropriate for high anxiety baseline. Use cautiously, at low doses, initially at night. |
| Low-dose THC with moderate CBD | For experienced users who tolerate THC. Start with 2.5 mg THC maximum. The CBD component is essential. Titrate extremely slowly. |
| High-THC, low-CBD products | NOT evidence-supported for anxiety. High risk of worsening anxiety, panic, paranoia. The amygdala activation mechanism is well documented. Avoid for anxiety management. |
Dosing Principles for Anxiety
Based on the clinical evidence and dose-dependence rule:
- Start with CBD-dominant products at low doses (10–25 mg CBD per dose) and titrate upward slowly over weeks
- Evidence supports CBD in the 150–800 mg/day range for anxiety disorders in clinical studies; however, lower doses (25–150 mg/day) are appropriate starting points for most patients
- For products containing any THC: start at 2.5 mg THC or less per dose and do not increase by more than 2.5 mg per week
- Daytime dosing for anxiety: CBD-dominant products without sedating terpenes are best to avoid functional impairment during work or social situations
- Nighttime dosing for sleep-related anxiety: modest THC addition (1:1 or 2:1 CBD:THC) may improve sleep onset while the CBD component modulates anxiogenic risk
- If you experience increased anxiety, racing heart, paranoia, or panic after any cannabis product, the THC content is the most likely cause. Switch to a CBD-only or CBD-dominant product.
Formulation Guidance by Anxiety Type
Generalized Anxiety Disorder: CBD-dominant sublingual tinctures provide reliable, consistent dosing and moderate onset (15–45 minutes). Twice-daily dosing (morning and evening) is consistent with clinical trial protocols. Oral capsules provide longer duration. Appropriate for ongoing daily anxiety management.
Social Anxiety Disorder: CBD-dominant products taken 1–1.5 hours before anticipated social situations may provide acute benefit based on Crippa et al.’s SAD neuroimaging data. Avoid any significant THC component for social situations — the last thing a socially anxious person needs is THC’s potential paranoia or increased self-consciousness.
Panic Disorder: CBD-dominant products for baseline management. High THC products are strongly contraindicated — they can directly trigger panic attacks. Vaporized CBD (faster onset) may be useful during acute anxiety escalation, but high-THC vaporized products should be avoided entirely.
Specific Phobias and Agoraphobia: CBD-dominant products for anticipatory anxiety management. CBT (Cognitive Behavioral Therapy) remains the evidence-based first-line treatment; cannabis as an adjunct should not replace exposure-based therapy.
Anxiety with prominent insomnia: A CBD:THC balanced product (2:1 or 1:1) at bedtime, starting at the lowest dose, can address both anxiety and sleep disruption. The CBD component moderates the anxiogenic risk of the THC component during sleep.
The Terpene Factor
Beyond cannabinoid ratio, terpenes in whole-plant cannabis products influence anxiety response. Two terpenes are particularly relevant for anxiety patients:
- Myrcene and linalool (linalool also found in lavender): produce sedating, calming effects. These terpenes complement CBD’s anxiolytic mechanism and are appropriate for anxiety management.
- Limonene: some evidence suggests citrus-derived terpenes have anxiolytic properties and are found in certain cannabis strains.
- Avoid products high in terpenes associated with stimulating or energizing effects (such as certain pinene-dominant strains) if your anxiety tends toward the activated, racing-mind variety rather than the sluggish, fatigued variety.
Ask your dispensary pharmacist to help identify products by terpene profile, not just by THC/CBD ratio.
Drug Interactions: Cannabis and Anxiety Medications
⚠ Tell Your Prescriber Before Adding Cannabis to Anxiety Medications
Many anxiety medications are metabolized through CYP enzyme pathways that CBD inhibits. Adding CBD to existing anxiety medications can raise drug levels significantly. This requires physician awareness, and in some cases, dose adjustment.
SSRIs (sertraline, escitalopram, fluoxetine, paroxetine): CBD inhibits CYP2D6 and CYP3A4, enzymes responsible for metabolizing many SSRIs. Fluoxetine and paroxetine are particularly dependent on CYP2D6. Adding CBD may increase SSRI blood levels. Monitor for enhanced SSRI side effects (nausea, headache, sexual dysfunction, increased heart rate). Alert your prescribing physician before starting CBD at moderate to high doses.
SNRIs (venlafaxine, duloxetine): Both are CYP2D6 substrates. Same interaction risk as SSRIs. Physician disclosure required.
Buspirone: Buspirone is metabolized by CYP3A4. CBD inhibits CYP3A4, potentially increasing buspirone levels. Monitor for enhanced buspirone effects (dizziness, headache, sedation). Physician disclosure required.
Benzodiazepines (alprazolam, clonazepam, lorazepam, diazepam): Benzodiazepines are primarily CYP3A4 substrates. CBD at significant doses can increase benzodiazepine blood levels. Additionally, CBD and benzodiazepines are both CNS depressants — combining them increases sedation risk. For patients using benzodiazepines for anxiety, cannabis should be started at the absolute lowest dose and physician involvement is essential. Do not use high-THC products with benzodiazepines.
Beta-blockers (propranolol for situational anxiety): No major CYP interaction with CBD. Both may lower blood pressure and heart rate — monitor for excessive effects (dizziness, fainting on standing).
TCAs (amitriptyline, nortriptyline): Metabolized by CYP2D6. CBD inhibition of CYP2D6 can increase TCA levels, raising risk of cardiac arrhythmia. Physician disclosure is essential; this interaction requires clinical monitoring.
Cannabis Should Complement, Not Replace, Evidence-Based Anxiety Treatment
This point deserves its own section because it is the most consistently underemphasized aspect of PA MMJ certification for anxiety — and the one most relevant to patient outcomes.
Cognitive Behavioral Therapy (CBT) is the most evidence-supported treatment for anxiety disorders. Its effectiveness across GAD, Social Anxiety Disorder, and Panic Disorder is demonstrated in hundreds of controlled trials. Exposure-based therapies have the best evidence for phobias and Panic Disorder specifically. SSRIs and SNRIs have strong evidence for long-term anxiety management. Buspirone is non-addictive and effective for GAD.
Cannabis for anxiety — particularly CBD — has growing and meaningful evidence for symptom management, particularly for patients with inadequate response to conventional treatments or those who cannot tolerate existing medications. It is not, however, a substitute for therapy or established pharmacotherapy in terms of evidence volume or long-term outcome data.
The PA DOH Secretary’s original guidance remains clinically sound: cannabis should be used in conjunction with conventional anxiety treatments, not instead of them. Patients who are not currently in therapy or not trying evidence-based first-line treatments for anxiety should consider those avenues alongside or before cannabis.
That said, the reality is that many anxiety patients have tried conventional treatments and found them inadequate, intolerable, or inaccessible. For those patients, cannabis represents a legitimate and legally recognized adjunct option in Pennsylvania.
How to Get Your Pennsylvania Medical Marijuana Card for Anxiety
Getting a PA MMJ card for anxiety is straightforward, but the anxiety qualifying condition has attracted scrutiny about certification quality in Pennsylvania. This section helps you navigate the process responsibly.
Step 1 — Ensure You Have a Clinical Anxiety Diagnosis
Pennsylvania requires a confirmed diagnosis of a qualifying medical condition. For anxiety disorders, this means a clinical diagnosis from a licensed healthcare provider (primary care physician, psychiatrist, psychologist, or therapist). While PA MMJ certifying physicians can accept patient self-report and medical history, having documented evidence of an anxiety disorder diagnosis strengthens your certification and represents the responsible standard of care.
Be prepared to share: your anxiety disorder diagnosis, any current or past treatments, current medications, and the specific symptoms you hope cannabis will help address.
Step 2 — Inform Your Primary Care Provider or Prescribing Physician
Tell your primary care physician, psychiatrist, or therapist that you are pursuing a PA MMJ card for anxiety. This matters because:
- Drug interactions between cannabis and anxiety medications require physician oversight (see above)
- Your mental health provider should know all interventions you are using so they can monitor your overall anxiety management
- Some medications may need dose adjustment if CBD significantly inhibits their metabolism
Step 3 — PA MMJ Physician Certification (Telehealth)
Book a telehealth appointment with a PA DOH-registered medical marijuana physician. These 10–15 minute video appointments can be completed from home. The certifying physician will review your anxiety diagnosis, current treatments, and specific symptom targets. Be specific about which anxiety symptoms you are hoping cannabis will address: sleep disruption, social situations, panic attacks, generalized worry, or other targets.
✨ Ready to get your PA MMJ card for anxiety?Our PA DOH-registered physicians understand the anxiety disorder evidence base and can help you identify CBD-dominant products most appropriate for your specific anxiety type and symptom profile.➡ [BOOK YOUR PA MMJ CERTIFICATION HERE — Insert booking link]
Step 4 — State Registration
After your physician certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com) with your certification, valid PA driver’s license or state-issued ID, and the $50 annual fee. Fee waivers are available for Medicaid, PACE/PACENET, CHIP, SNAP, or WIC recipients.
Step 5 — First Dispensary Visit
Tell the dispensary pharmacist you have an anxiety disorder. Be specific about your type (GAD, social anxiety, panic disorder, etc.), which symptoms are most disabling, your current medications, and whether you have any previous cannabis experience. Request CBD-dominant products. Ask about terpene profiles. Start with the lowest possible dose.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: Can I get a PA MMJ card for anxiety if I haven’t tried other treatments first?
Q: Will cannabis make my anxiety worse?
Q: My anxiety includes depression. Will cannabis help with both?
Q: I’m currently on an SSRI. Can I add CBD?
Q: I use benzodiazepines for anxiety. Is cannabis safe to add?
Q: Are there anxiety subtypes where cannabis is more effective?
Q: I’m under 18 with diagnosed anxiety. Can I qualify?
Anxiety Support and Mental Health Resources in Pennsylvania
NAMI Pennsylvania (National Alliance on Mental Illness): Provides education, peer support, and advocacy for mental health conditions including anxiety disorders. Helpline: 1-800-950-NAMI (6264).
Anxiety and Depression Association of America (ADAA): Comprehensive educational resources, therapist finder (specializing in anxiety and depression), and treatment information. adaa.org.
SAMHSA National Helpline: 1-800-662-HELP (4357) — Free, confidential, 24/7 mental health and substance use treatment referral service.
Psychology Today Therapist Finder: Search for CBT therapists in Pennsylvania who specialize in anxiety disorders at psychologytoday.com/us/therapists. CBT is the evidence-supported first-line treatment for most anxiety disorders.
PA DOH Mental Health Resources: Provides information on mental health services across Pennsylvania.
Crisis Support: If you are experiencing a mental health crisis, call or text 988 (Suicide & Crisis Lifeline), available 24/7. Crisis Text Line: text HOME to 741741.
Conclusion
Anxiety disorders are the most common qualifying condition in Pennsylvania’s medical marijuana program for good reason: they are the most common mental health condition in America, and millions of people are inadequately served by existing treatments. Cannabis — specifically CBD at appropriate doses — has a growing and meaningful evidence base for anxiolytic effects, supported by multiple systematic reviews, meta-analyses, and controlled trials showing significant reductions in GAD, Social Anxiety Disorder, and related conditions.
At the same time, the THC-anxiety relationship demands honest acknowledgment: high-dose THC is a proven anxiogenic substance in controlled conditions, and high-THC products used without guidance represent a real risk of worsening anxiety disorders rather than improving them. This is not a theoretical concern — it is a well-documented pharmacological reality with neuroimaging evidence behind it.
For Pennsylvania anxiety patients, the path to safe and effective cannabis use runs through three principles: choose CBD-dominant products, start at the lowest effective dose, and use cannabis as a complement to — not a replacement for — the evidence-based treatments (therapy, appropriate medications) that remain the foundation of anxiety disorder care. A PA MMJ card provides legal access to Pennsylvania’s dispensary system and the opportunity to work with dispensary pharmacists who can help you navigate product selection based on your specific anxiety type and treatment goals.