
Neuropathy. It is one of the most common, most undertreated, and most misunderstood pain conditions in medicine. Patients describe it as burning, stabbing, electric shocks, pins and needles, or a feeling that their skin is being scraped raw — sensations that conventional medications often fail to adequately control. For the roughly 20 million Americans living with peripheral neuropathy, and the millions more affected by diabetic, chemotherapy-induced, HIV-related, and other forms of nerve damage, the daily reality of neuropathic pain is exhausting.
Pennsylvania recognized neuropathies as a qualifying condition for medical marijuana from the very first version of Act 16 in 2016 — and for scientifically sound reasons. The endocannabinoid system is not a peripheral player in pain signaling. It is deeply embedded in the exact neural pathways that neuropathy disrupts. Cannabis-based medicines have more randomized controlled trial evidence for neuropathic pain than for almost any other condition on Pennsylvania’s qualifying list.
This page gives neuropathy patients and their families the complete picture: what qualifies under Pennsylvania law, the full scope of neuropathy types covered, how cannabinoids work on nerve pain at a biological level, what 22 randomized controlled trials across 20 years of research actually show, neuropathy-type-specific evidence, product guidance, the drug interaction considerations your current prescriber needs to know, and a clear path to getting your PA MMJ card. No generic content. No overselling. The full evidence, honestly presented.
Does Neuropathy Qualify for Medical Marijuana in Pennsylvania?
Yes — and it qualifies as one of the broadest categories on Pennsylvania’s list.
Neuropathies is an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016). Unlike some conditions that require a specific severity threshold or proof of treatment failure, the neuropathies category in Pennsylvania covers the full spectrum of nerve damage diagnoses.
What this means in practice: you do not need to have advanced or end-stage neuropathy. You do not need to prove that gabapentin, pregabalin, duloxetine, or other standard treatments have failed. A confirmed diagnosis of a neuropathy from a qualified physician is the qualification.
Pennsylvania also lists ‘Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity and other associated neuropathies’ as a separate qualifying condition — meaning patients with CNS-origin neuropathies (such as multiple sclerosis-related neuropathy) may qualify under either or both categories.
The following neuropathy diagnoses all fall within the qualifying scope:
- Peripheral neuropathy (any cause)
- Diabetic peripheral neuropathy (DPN)
- Chemotherapy-induced peripheral neuropathy (CIPN)
- HIV-associated sensory neuropathy
- Postherpetic neuralgia (shingles-related nerve pain)
- Idiopathic polyneuropathy
- Alcoholic neuropathy
- Hereditary neuropathies including Charcot-Marie-Tooth disease
- Autoimmune neuropathies including CIDP and Guillain-Barré syndrome sequelae
- Small fiber neuropathy
- Traumatic nerve injury with persistent neuropathic pain
- Toxic neuropathy (heavy metals, medications)
If you have a diagnosis of any form of neuropathy documented in your medical records, you have the medical foundation to qualify for a PA MMJ card.
Sources:
- Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Marijuana Policy Project – Act 16 Research and Evidence on Qualifying Conditions
What Are Neuropathies? Understanding the Full Scope
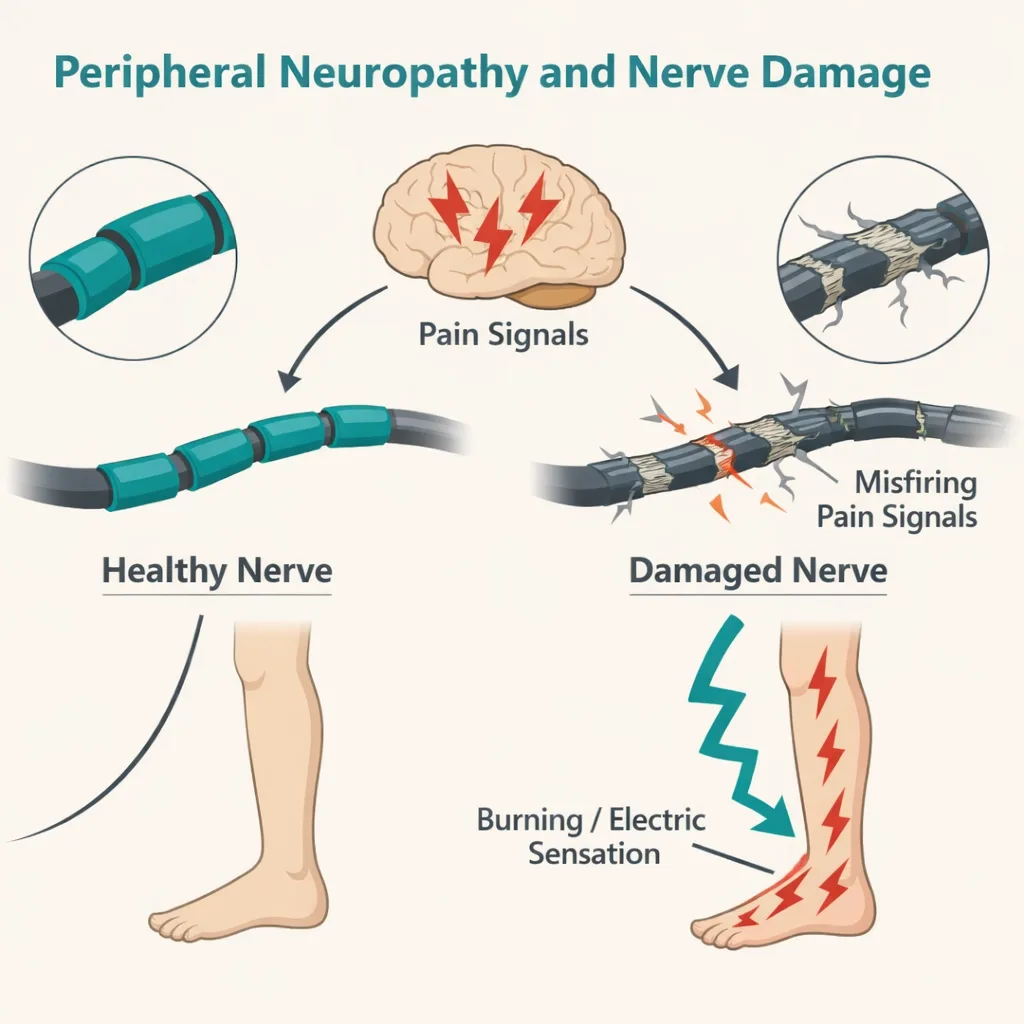
The word ‘neuropathies’ is a category, not a single disease. It refers to any condition in which peripheral nerves — the vast network of nerves outside the brain and spinal cord — are damaged, dysfunctional, or destroyed. The result is a disruption in the nerve’s ability to transmit accurate signals, producing the characteristic symptoms of neuropathy: burning pain, numbness, tingling (paresthesia), hypersensitivity to touch (allodynia), weakness, and loss of coordination.
According to NIH StatPearls, approximately 2.4% of the world population is affected by peripheral nerve disorders, with the prevalence rising to 8% in older populations. In the United States, an estimated 20 million people live with some form of peripheral neuropathy. The Foundation for Peripheral Neuropathy estimates 190 million people worldwide are affected.
The Major Neuropathy Types Covered Under PA’s Qualifying Criteria
| Neuropathy Type | What It Is & Who Gets It |
|---|---|
| Diabetic Peripheral Neuropathy (DPN) | The most common form. Affects 50–70% of people with diabetes over their lifetime. High blood sugar damages nerve fibers, producing burning pain, numbness, and tingling — typically starting in the feet and progressing upward. |
| Chemotherapy-Induced Peripheral Neuropathy (CIPN) | Affects 30–40% of cancer patients receiving chemotherapy. Platinum agents, taxanes, and vinca alkaloids are most frequently responsible. Often persists long after treatment ends. |
| HIV-Associated Sensory Neuropathy | Occurs in approximately 33% of HIV/AIDS patients. Caused both by the virus itself and by older antiretroviral medications. Characterized by burning or stabbing pain in the feet. |
| Postherpetic Neuralgia | Nerve pain persisting after a shingles (herpes zoster) outbreak. One of the most persistent and treatment-resistant neuropathic pain conditions. |
| Idiopathic Polyneuropathy | No identifiable cause found despite thorough investigation. Accounts for up to 25% of all polyneuropathy cases, particularly in older adults. |
| Small Fiber Neuropathy | Affects the small nerve fibers responsible for pain and temperature sensation. Often missed on standard nerve conduction studies; requires skin punch biopsy for diagnosis. |
| CIDP / Autoimmune Neuropathy | Chronic inflammatory demyelinating polyneuropathy and related autoimmune nerve disorders. Treated with immunotherapy but frequently leaves residual neuropathic pain. |
| Hereditary Neuropathy (e.g., CMT) | Charcot-Marie-Tooth disease is the most common inherited peripheral neuropathy, affecting approximately 1 in 2,500 people worldwide. |
| Alcoholic Neuropathy | Caused by long-term alcohol use, which is directly toxic to nerves and impairs B-vitamin absorption. Results in painful polyneuropathy predominantly in the lower extremities. |
What these diverse conditions share is the final common pathway: damaged peripheral nerves sending abnormal, dysregulated pain signals to the brain. This shared mechanism is why a single pharmacological approach — modulating the endocannabinoid system — can have therapeutic relevance across neuropathy types.
Sources:
- NCBI StatPearls – Neuropathy
- Foundation for Peripheral Neuropathy – Types of Risk Factors
- PMC – Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes
- PMC – The Global Burden of Polyneuropathy
Why Neuropathic Pain Is So Difficult to Treat — And Why Cannabis Is Different
Standard pain medications — NSAIDs, acetaminophen, and opioids — are largely ineffective for neuropathic pain. This is not a dosing problem. It is a mechanistic one. These drugs are designed for nociceptive pain (the pain signal from tissue damage), not for the dysregulated central sensitization and aberrant nerve signaling that defines neuropathy.
The standard first-line treatments for neuropathic pain — gabapentinoids (gabapentin/pregabalin), serotonin-norepinephrine reuptake inhibitors (duloxetine/venlafaxine), and tricyclic antidepressants (amitriptyline) — work better than opioids but still leave a significant percentage of patients with inadequate pain control. A key figure from the clinical literature: in neuropathic pain studies, a ‘30% pain reduction’ is considered a clinically meaningful outcome threshold — meaning researchers consider it a success if patients achieve just a one-third reduction in their pain. This is how hard neuropathic pain is to treat.
Cannabis works through an entirely different mechanism: the endocannabinoid system.
How Cannabinoids Address Neuropathic Pain: The Biology
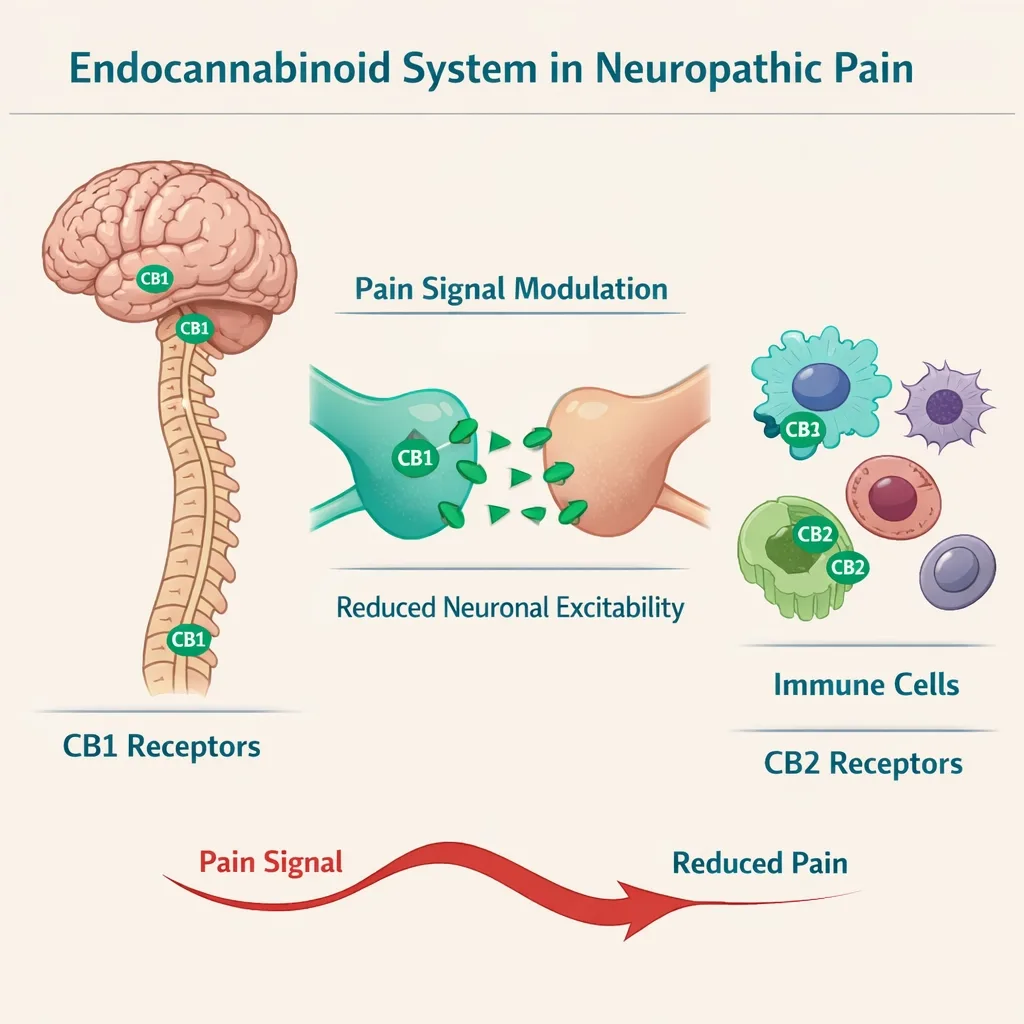
The endocannabinoid system (ECS) plays a central, well-documented role in pain modulation. CB1 receptors are distributed throughout the entire pain pathway — in peripheral sensory nerve endings, the dorsal root ganglion, the spinal cord’s dorsal horn (the first synapse in the pain relay), and key brain regions that process pain including the thalamus, amygdala, and periaqueductal gray matter. CB2 receptors are expressed on immune and glial cells throughout the nervous system and upregulate specifically in response to inflammation and nerve injury.
When a peripheral nerve is damaged, the ECS responds: CB1 receptors upregulate in the spinal cord, and activated microglia (the brain’s immune cells) significantly increase their production of endogenous cannabinoids (anandamide and 2-AG) as part of the pain-dampening response. The ECS is, in a very real sense, the body’s own attempt to brake neuropathic pain.
External cannabinoids — THC and CBD from cannabis — act on this same system through several distinct mechanisms:
- CB1 receptor activation by THC suppresses calcium conductance and inhibits potassium conductance at nerve terminals, reducing neuronal excitability and the release of pain-signaling neurotransmitters
- CB2 receptor activation reduces neuroinflammation by decreasing microglial production of pro-inflammatory cytokines — a key driver of central sensitization in neuropathic pain
- Cannabinoids modulate TRPV1 (vanilloid) receptors — the ‘capsaicin receptor’ — which are heavily involved in heat and pain signaling in damaged nerves
- CBD inhibits anandamide reuptake, effectively increasing the body’s own endocannabinoid levels at pain-relevant sites
- The combination of peripheral and central ECS modulation produces analgesia through multiple pathways simultaneously — which is why cannabinoids can succeed where single-mechanism drugs fail
This is not speculative. These mechanisms are established in peer-reviewed neuropharmacology literature from leading institutions including Nature Neuropsychopharmacology, PMC/NIH, and Frontiers in Pharmacology.
Sources:
- PMC – Applications of Cannabinoids in Neuropathic Pain: An Updated Review
- Frontiers in Neural Circuits – Cannabinoids in Chronic Pain: Therapeutic Potential Through Microglia Modulation
- PMC – Cannabinoids as Pharmacotherapies for Neuropathic Pain: From the Bench to the Bedside
- Nature Neuropsychopharmacology – The Endogenous Cannabinoid System: Targets for Neuropathic Pain
- Frontiers in Pharmacology – Cannabinoids and Pain: New Insights From Old Molecules
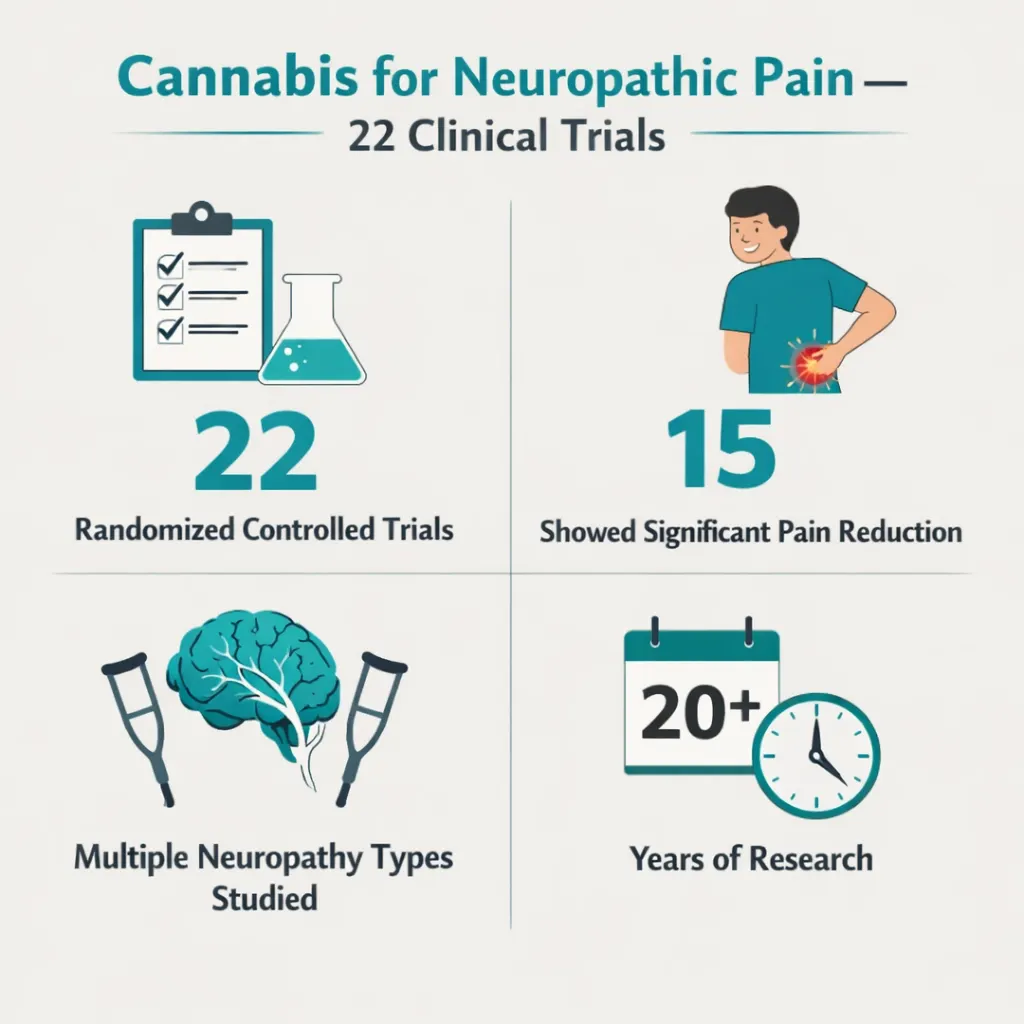
What the Clinical Research Shows: 22 Randomized Controlled Trials
Neuropathic pain is the single most-studied indication for cannabis-based medicines in the clinical trial literature. This gives Pennsylvania neuropathy patients something most qualifying conditions cannot offer: a substantial, multi-decade body of controlled human trial evidence — not just preclinical data.
The Landmark 2025 Systematic Review: 22 RCTs, 20 Years of Evidence
A comprehensive systematic review published in 2025 (MDPI Biomolecules) searched PubMed, MEDLINE, and Web of Science from January 2003 to December 2024 and identified 22 randomized controlled trials evaluating cannabis-based medicines specifically for neuropathic pain. The finding: significant pain reductions were reported in 15 of the 22 studies — covering multiple sclerosis, spinal cord injuries, diabetic neuropathy, postherpetic neuralgia, HIV-associated sensory neuropathy, peripheral neuropathic pain, complex regional pain syndrome, chronic radicular neuropathic pain, and peripheral neuropathy of the lower extremities.
The weight of evidence is clear and consistent: cannabinoids containing THC reduce neuropathic pain across multiple etiologies in controlled trials. The key findings from the research body, organized by neuropathy type:
Diabetic Peripheral Neuropathy (DPN)
DPN trials represent some of the strongest evidence in the neuropathic pain literature. A randomized, double-blind, placebo-controlled crossover study by Wallace et al. evaluated cannabis inhalation at three THC doses (1%, 4%, and 7%) in 16 patients with at least 6 months of neuropathic foot pain from diabetes. All THC doses produced significant pain reductions compared to placebo, with higher doses producing greater analgesia lasting the full 4-hour test duration.
A 2025 Phase III randomized double-blind trial of transdermal cannabis (a THC:CBD:CBN formulation) in 100 patients with painful DPN over 12 weeks found statistically significant improvements in pain scores compared to placebo — making it one of the most recent and methodologically rigorous DPN cannabis trials to date. A 2024 scoping review confirmed that THC-containing preparations showed better DPN pain improvements than chemotherapy-induced or multiple sclerosis-related neuropathy, particularly with vaporized whole-plant cannabis.
Chemotherapy-Induced Peripheral Neuropathy (CIPN)
CIPN represents an enormous unmet need — affecting 30–40% of cancer patients and often persisting long after treatment ends with no FDA-approved treatment specifically indicated for prevention. Cannabis-based medicines have been studied as both treatment and preventive agents.
A pilot randomized placebo-controlled trial (2024) evaluated topical CBD for established CIPN and found improvements in pain and sensory symptoms. THC:CBD combinations have also shown reductions in CIPN pain in controlled trials, with oral mucosal cannabinoid extract studied specifically for chemotherapy-induced neuropathic pain.
Important Context for CIPN PatientsIf you are an active cancer patient using chemotherapy, cannabis may interact with certain chemotherapy drugs through CYP enzyme metabolism pathways. This interaction is dose- and drug-dependent and does not mean cannabis is contraindicated — but it does mean your oncologist must know you are using it. Discuss cannabis use with your oncology team before, during, and after chemotherapy.
HIV-Associated Sensory Neuropathy
HIV-associated neuropathy has some of the oldest and most definitive cannabis trial evidence. A landmark randomized, placebo-controlled crossover trial by Abrams et al. (2007, published in Neurology) found that smoked cannabis was well tolerated and effectively relieved chronic neuropathic pain from HIV-associated sensory neuropathy — with findings comparable to oral drugs commonly used for chronic neuropathic pain. A separate trial by Ellis et al. confirmed significant pain reduction with vaporized cannabis compared to placebo in HIV neuropathy patients.
Postherpetic Neuralgia and General Peripheral Neuropathic Pain
Multiple controlled trials have evaluated cannabis-based medicines for peripheral neuropathic pain from mixed or general etiologies. A meta-analysis by Andreae et al. evaluated 5 randomized controlled trials in 178 patients with neuropathy of at least 3 months duration and found that 1 in every 5 to 6 patients treated with cannabis had at least a 30% pain reduction — a result comparable to other established neuropathic pain medications. Separate analyses have found that actively treated patients were consistently more likely to achieve a 30% improvement in neuropathic pain compared to placebo.
What the Evidence Tells Us About Which Cannabinoids Work
The Evidence Hierarchy for Neuropathic Pain
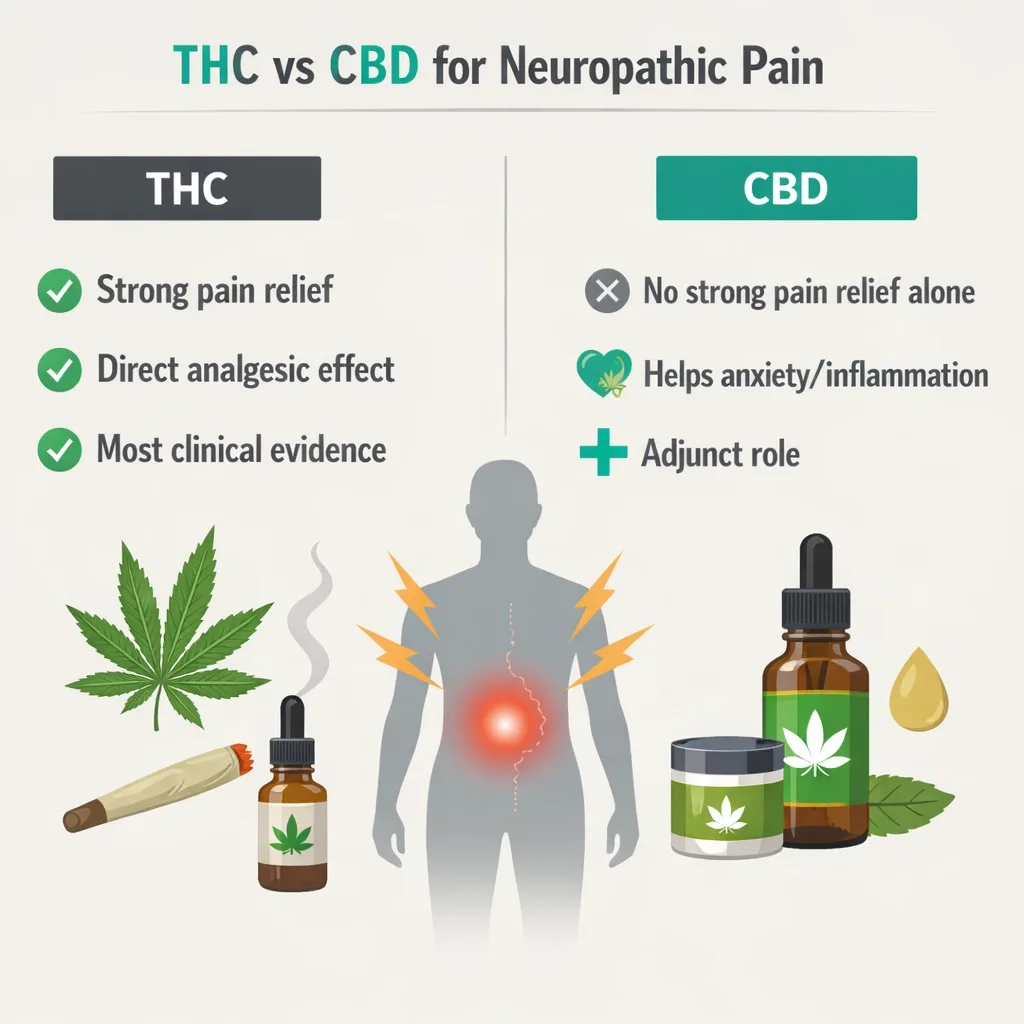
THC-dominant preparations: strongest and most consistent clinical evidence across neuropathy types. Ten studies using phytocannabinoid preparations containing THC showed the most evidence for pain relief.THC:CBD combination products: four studies showed reductions in pain scores, though not all reached statistical significance.
The oromucosal spray (Sativex) approach has been evaluated in several neuropathic pain trials.CBD alone: two clinical studies in neuropathic pain showed no analgesic effect over placebo. Note: these were small, short-duration studies, and CBD’s anti-inflammatory properties may still benefit neuropathy through non-pain pathways.Cannabidivarin (CBDV): one study showed no analgesic effect over placebo for neuropathic pain.
Bottom line: THC is the primary active analgesic cannabinoid for neuropathic pain in human trials. CBD may contribute to inflammation reduction but is not independently established as an analgesic for nerve pain.
The 2025 updated systematic review in Annals of Internal Medicine (covering trials to July 2025, with 64% of patients having neuropathic pain) found that oral synthetic/purified high THC-to-CBD and oromucosal extracted comparable THC-to-CBD ratio products both produced statistically significant pain severity reductions on the 0–10 scale, though with increased risk of adverse events including dizziness, dry mouth, and somnolence.
Sources:
- MDPI Biomolecules – Are Cannabis-Based Medicines a Useful Treatment for Neuropathic Pain? A Systematic Review (2025)
- PMC – Efficacy and Safety of Transdermal Medical Cannabis for Painful Diabetic Peripheral Neuropathy (Phase III, 2025)
- PubMed – Phytocannabinoids for Treatment of Neuropathic Pain: Scoping Review of RCTs 2012–2023
- Cleveland Clinic Journal of Medicine – Cannabis for Peripheral Neuropathy: The Good, the Bad, and the Unknown
- Annals of Internal Medicine – Cannabis-Based Products for Chronic Pain: Updated Systematic Review (2025)
- NORML – MPP Act 16 Research & Evidence: Neuropathic Pain
Beyond Pain: Other Benefits Cannabis Offers Neuropathy Patients
Neuropathic pain does not exist in isolation. It disrupts sleep, generates anxiety, drives depression, and degrades quality of life across every domain. Cannabis addresses several of these secondary burdens, and PA dispensary products can be selected to target them specifically.
Sleep disruption: Neuropathic pain is frequently worst at night, causing severe sleep disruption. THC at modest doses reliably reduces sleep onset latency, increases total sleep time, and reduces nighttime awakenings. A dosing strategy of placing the highest-dose administration at bedtime serves both pain relief and sleep quality simultaneously.
Anxiety and psychological burden: Living with chronic pain of any type carries a high psychological toll. CBD-dominant formulations at appropriate doses have well-established anxiolytic properties and can serve as a daytime complement to THC-based pain management without psychoactive impairment.
Co-existing muscle spasm or spasticity: Many neuropathy patients, particularly those with CIPN or HIV neuropathy, also experience muscle spasms or spasticity. Cannabis has established evidence for spasticity relief (supported across multiple sclerosis trials), making it a genuinely multi-target therapy for these patients.
Opioid reduction: A series of randomized clinical trials found that vaporized marijuana significantly augmented the analgesic effect of opioids in chronic pain patients, with one study concluding the combination may allow for opioid treatment at lower doses with fewer side effects. For neuropathy patients on opioid therapy, cannabis may support opioid dose reduction — a significant safety benefit given opioid risks.
PA Dispensary Product Selection for Neuropathy Patients
The clinical evidence points to very specific product guidance for neuropathy. Here is what the science recommends for each neuropathy symptom target — not generic dispensary advice.

For Neuropathic Pain Relief (Primary Target)
THC-dominant oral formulations — tinctures, capsules, or tablets — represent the most evidence-aligned choice for ongoing neuropathic pain management. Oral formulations provide a longer duration of action (4–8 hours) compared to vaporized forms (2–4 hours), which better matches the persistent, around-the-clock nature of neuropathic pain.
Starting dose: For a patient new to cannabis, begin with 2.5–5 mg THC oral dose. Titrate upward by 2.5 mg every 3–5 days, assessing pain reduction against side effects. Most neuropathic pain patients find an effective dose between 5 and 20 mg THC per administration.
For breakthrough pain: Vaporized cannabis provides faster onset (within 5–15 minutes) and is appropriate for acute flares or breakthrough episodes, used alongside oral maintenance dosing.
For Sleep-Related Neuropathic Pain
THC-dominant tincture or capsule administered 1–1.5 hours before bedtime. Higher evening dosing than daytime dosing is a validated strategy consistent with clinical guidance for chronic pain conditions using cannabis.
Adding a modest amount of CBD (a 1:1 or 2:1 THC:CBD ratio product at bedtime) can reduce THC-associated anxiety and prolong sleep duration in some patients.
For Daytime Anxiety and Psychological Burden
CBD-dominant products (10:1 CBD:THC or higher) dosed during the day provide anxiolytic benefit without significant psychoactive impairment. These products complement THC-based nighttime pain dosing and address the psychological component of chronic neuropathic pain.
Formulation Considerations by Neuropathy Type
- Diabetic neuropathy patients: Oral capsules or tinctures preferred. Monitor blood glucose carefully, as cannabis may influence insulin sensitivity in some individuals. Inform your endocrinologist or primary care physician.
- CIPN patients (active chemotherapy): Consult oncologist first. Topical CBD formulations for localized symptoms may be preferable during active treatment to minimize systemic exposure. Oral formulations appropriate post-chemotherapy.
- HIV neuropathy patients: Review antiretroviral drug interactions before beginning cannabis (see below).
- Postherpetic neuralgia: Topical cannabis formulations — creams, gels, or transdermal patches — applied to the affected dermatome represent an underutilized but evidence-supported approach that avoids systemic effects.
- Elderly patients or those with cognitive concerns: Lower starting doses, longer titration periods, CBD-dominant products for daytime use, and close monitoring by a caregiver or family member.
Drug Interaction Warning: What Neuropathy Patients Must Know
This section is the most frequently omitted by competing PA MMJ sites, and it is the section that could genuinely harm patients if ignored. Cannabis interacts with several medication classes commonly used by neuropathy patients.
⚠ Critical: Tell Your Prescriber Before Starting Cannabis
Cannabis — particularly CBD — is a significant inhibitor of the CYP2C9, CYP2C19, and CYP3A4 enzyme pathways through which many medications are metabolized. This means cannabis can raise blood levels of drugs that are broken down by these pathways, increasing the risk of side effects, or lower blood levels of drugs that induce these pathways, reducing their effectiveness. Always inform your prescribing physician before starting cannabis.
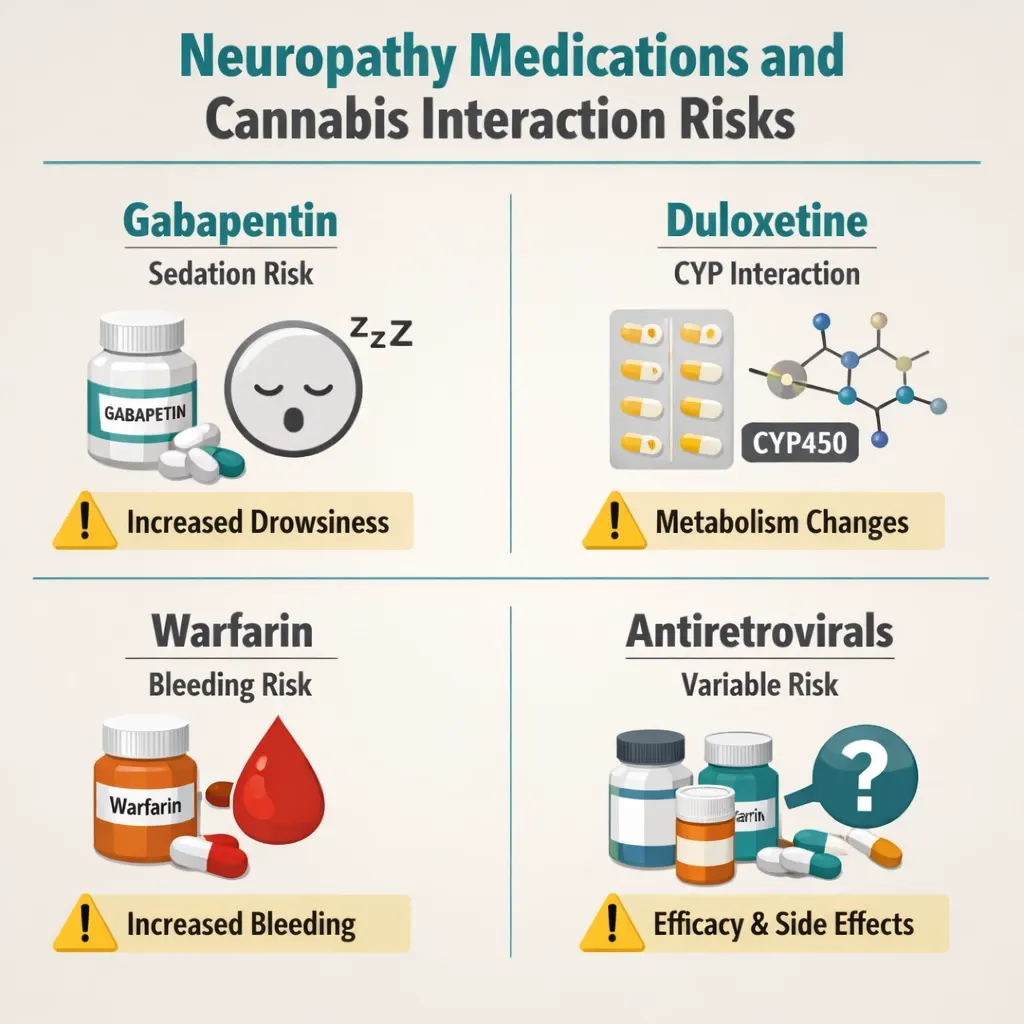
Gabapentin and pregabalin: No major pharmacokinetic interaction is expected, as these drugs are renally excreted rather than CYP-metabolized. Cannabis and gabapentinoids can be used concurrently, though additive CNS sedation should be monitored, especially in elderly patients or at high doses.
Duloxetine and antidepressants: CBD inhibits CYP2D6, through which several antidepressants are metabolized. This can increase duloxetine blood levels. Alert your prescribing physician.
Blood thinners (warfarin): CBD is a known inhibitor of CYP2C9, the primary enzyme responsible for warfarin metabolism. Cannabis use can significantly raise warfarin blood levels, increasing bleeding risk. If you take warfarin, this requires explicit physician involvement and potentially more frequent INR monitoring.
Antiretrovirals (HIV patients): Cannabis interactions with HIV medications are drug-class dependent. Protease inhibitors (ritonavir, cobicistat) can increase cannabis blood levels. Cannabis can reduce atazanavir levels below therapeutic range. NNRTIs including efavirenz and etravirine may increase cannabis exposure. Review hiv-druginteractions.org with your HIV physician before starting cannabis.
Diabetic medications: Cannabis does not consistently lower blood glucose, and in some individuals may worsen glycemic control due to increased appetite. Patients with diabetes should monitor blood glucose closely after beginning cannabis and coordinate with their endocrinologist or primary care provider.
The general rule: cannabis should be treated as a new medication added to your regimen, with the same disclosure standard as any prescription drug. Your prescribing physicians need to know you are using it.
How to Get Your Pennsylvania Medical Marijuana Card for Neuropathy
The process is simpler than most patients expect, can be completed entirely from home, and typically takes less than a week from certification to having your digital MMJ card. Here is the step-by-step path for neuropathy patients specifically.
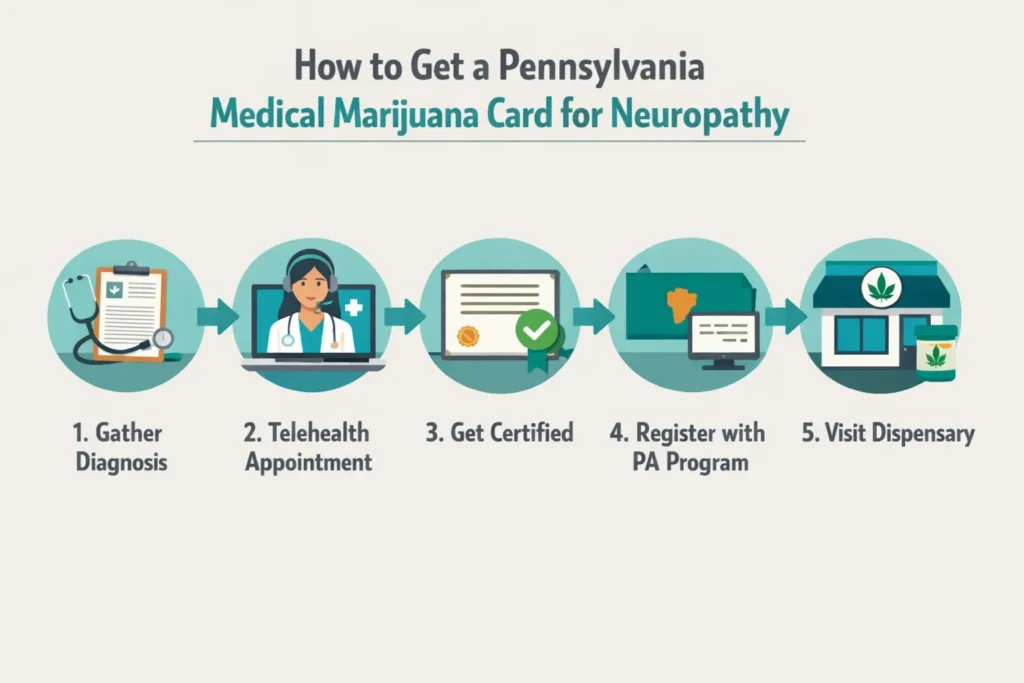
Step 1 — Gather Your Medical Records
Before your certification appointment, locate documentation of your neuropathy diagnosis. This typically includes:
- A letter or visit notes from your neurologist, primary care physician, or endocrinologist confirming your diagnosis
- Any nerve conduction studies, EMG reports, or skin punch biopsy results if available
- Your current medication list — especially any neuropathy medications (gabapentin, pregabalin, duloxetine, etc.)
Having these records ready shortens your certification appointment and ensures the certifying physician has the complete picture needed to certify you and provide appropriate product guidance.
Step 2 — Inform Your Treating Physician
Tell your neurologist or primary care physician that you are pursuing a PA MMJ card for your neuropathy. This serves two purposes: (1) they need to know for the drug interaction reasons outlined above, and (2) their awareness ensures your neuropathy care and cannabis use are coordinated rather than siloed.
Step 3 — PA MMJ Physician Certification (Telehealth)
Book a telehealth appointment with a PA DOH-registered medical marijuana physician. These appointments are typically 10–15 minutes, conducted via video from your home. The certifying physician will review your neuropathy diagnosis and symptoms, discuss your treatment goals, and provide a written certification to the PA DOH registry.
✨ Ready to get your PA MMJ card for neuropathy?
Our PA DOH-registered physicians understand neuropathic pain, can discuss which cannabis products are most evidence-supported for your specific neuropathy type, and will certify you in a comfortable 15-minute telehealth appointment.➡ [BOOK YOUR PA MMJ CERTIFICATION HERE — Insert booking link]
Step 4 — State Registration
After physician certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com). You will need:
- Your physician certification
- Valid PA driver’s license or state-issued ID
- $50 annual registration fee (fee waivers available for Medicaid, PACE/PACENET, CHIP, SNAP, or WIC recipients)
Your digital PA MMJ card is typically accessible within a few business days of completing registration.
Step 5 — First Dispensary Visit
Tell the dispensary pharmacist you have neuropathy. Be specific about the type (diabetic, CIPN, HIV-related, postherpetic, etc.), your primary symptoms (pain intensity, sleep disruption, anxiety), and your current medications. A knowledgeable dispensary pharmacist will help you select the right formulation, cannabinoid ratio, and dosing approach for your specific situation.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Multiple Sclerosis
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
Frequently Asked Questions
Q: I have diabetic neuropathy but my pain is currently managed with gabapentin. Do I still qualify?
Q: Can I use cannabis alongside gabapentin or pregabalin safely?
Q: I have small fiber neuropathy. My standard nerve conduction studies were normal. Do I still qualify?
Q: Will CBD oil alone help my neuropathy?
Q: I’m a cancer patient with CIPN. Is it safe to use cannabis during chemotherapy?
Q: My neuropathy is hereditary (Charcot-Marie-Tooth). Does that qualify?
Q: Does cannabis use show up on drug tests even with a PA MMJ card?
Neuropathy Support Resources
Foundation for Peripheral Neuropathy: The leading national organization for peripheral neuropathy patients, providing disease education, treatment information, and patient support resources at foundationforpn.org.
American Chronic Pain Association: Provides comprehensive resources for neuropathic pain management, including a directory of healthcare providers experienced in chronic pain. theacpa.org.
Neuropathy Action Foundation: Patient advocacy organization focused on research funding and education for neuropathy patients. neuropathyaction.org.
NIH – National Institute of Neurological Disorders and Stroke: Authoritative information on all neuropathy types, current research, and treatment options. ninds.nih.gov.
Cleveland Clinic Neurological Institute: Maintains one of the most accessible evidence-based patient resources on cannabis and peripheral neuropathy online. clevelandclinic.org.
Conclusion
Of all the qualifying conditions on Pennsylvania’s medical marijuana list, neuropathies may have the most directly applicable clinical trial evidence for cannabis as a therapeutic option. Twenty-two randomized controlled trials spanning 20 years and multiple neuropathy subtypes. Pain reductions in 15 of 22 studies. An established biological mechanism that connects the endocannabinoid system directly to how neuropathic pain is generated and sustained. FDA approval of a synthetic cannabinoid specifically for neuropathic pain indications.
This does not mean cannabis will eliminate your neuropathic pain. It means cannabis is a scientifically legitimate, evidence-supported option for managing it — one that works through a completely different mechanism than standard medications, which is precisely why it can succeed where those medications have not fully worked.
NOTE: A PA MMJ card gives you legal access to a range of products specifically applicable to your condition. The key is choosing products based on evidence — THC-dominant for pain and sleep, CBD-complement for daytime anxiety, topical for localized symptoms — in coordination with the physicians who manage your neuropathy care.