
Living with HIV today looks radically different from what it looked like in 1985. For most people with access to modern antiretroviral therapy, HIV is a managed chronic condition rather than a death sentence. CD4 counts stay high, viral loads stay undetectable, and life expectancy approaches that of HIV-negative peers. But “managed” doesn’t mean symptom-free.
HIV-related peripheral neuropathy, treatment-related nausea, appetite disruption, psychological distress, and sleep problems remain real and common and they are exactly the symptom targets where cannabis has its clearest evidence base in this population.
Pennsylvania recognized HIV and AIDS as qualifying conditions from the start of its Medical Marijuana Act, and the statutory language contains an important nuance that most cannabis websites gloss over.
This page explains what actually qualifies, what the research shows symptom by symptom, and most critically, how cannabis interacts with the antiretroviral medications that most PA MMJ cardholders with HIV will already be taking.
Does HIV/AIDS Qualify for Medical Marijuana in Pennsylvania?
Yes – and the statutory language matters here. Pennsylvania’s Medical Marijuana Act qualifies “positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome.”
This means:
- HIV-positive status alone qualifies. You do not need to have progressed to AIDS.
- There is no CD4 count threshold. A newly diagnosed, virally suppressed patient with a CD4 count of 800 qualifies just as much as a patient with advanced immunosuppression.
- There is no requirement that AIDS-defining conditions be present.
- There is no requirement that standard treatments have failed for any specific symptom.
A confirmed HIV diagnosis documented by a licensed physician is sufficient. The qualifying condition is the serostatus itself, not a disease stage, not a specific complication.
- Source: Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Source: 28 Pa. Code Appendix A – Serious Medical Conditions
What Is HIV, and What Does “Living with HIV” Mean in 2026?
HIV (Human Immunodeficiency Virus) attacks CD4+ T lymphocytes, the immune cells that coordinate the body’s defense against infections. Without treatment, HIV progressively depletes CD4+ cells, eventually crossing the threshold into AIDS (Acquired Immune Deficiency Syndrome), defined by a CD4 count below 200 cells/mm³ or the presence of AIDS-defining opportunistic infections.
The landscape changed fundamentally in 1996 with the introduction of combination antiretroviral therapy (ART). Modern ART, particularly integrase strand transfer inhibitor (INSTI)-based regimens such as dolutegravir/emtricitabine/tenofovir (Triumeq, Biktarvy), suppresses HIV viral load to undetectable levels in most patients, preserves CD4+ counts, and has dramatically reduced AIDS-related mortality.
Pennsylvania is one of 24 states with among the highest HIV burden. An estimated 40,000+ Pennsylvanians are living with HIV, with Philadelphia among the highest-prevalence cities in the country.
What this means for PA MMJ patients: The majority of people living with HIV (PLWH) who seek a PA MMJ card today are on ART and virally suppressed. They are not primarily seeking cannabis for wasting syndrome or acute AIDS complications, they are seeking it for the chronic symptom burden that persists even on effective ART: neuropathic pain, treatment-related GI side effects, appetite disruption, insomnia, anxiety, and depression. The evidence base for cannabis maps well onto this symptom profile.
- Source: NIH/NIAID – HIV Overview
- Source: NIH clinicalinfo.hiv.gov – Guidelines for the Use of Antiretroviral Agents
The Endocannabinoid System and HIV: Why the Biology Makes Sense
Cannabinoid receptors — CB1 and CB2 are expressed throughout the immune system as well as the central and peripheral nervous system. CB2 receptors in particular are concentrated on immune cells, including CD4+ T lymphocytes, macrophages, and microglia. This distribution is directly relevant to HIV biology.
HIV and ART both independently damage peripheral sensory nerves, the primary driver of HIV-related neuropathic pain (HRNP). The mechanism involves direct viral neurotoxicity, immune-mediated nerve damage, and antiretroviral neurotoxicity (particularly from older nucleoside reverse transcriptase inhibitors such as stavudine and didanosine, now largely discontinued, but still implicated in persistent neuropathy in patients exposed to them). Cannabinoid receptor activation modulates pain signaling at multiple points in this cascade.
CB1 receptor activation produces analgesia centrally and peripherally, reduces nausea via brainstem CB1 receptors, and stimulates appetite via hypothalamic CB1 signaling. CB2 receptor activation modulates inflammatory and immune responses, relevant to the chronic systemic inflammation that persists in virally suppressed PLWH.
One important research observation: in a primate SIV model (the closest animal analog to HIV), chronic THC administration prior to and during SIV infection was associated with attenuated viral load, reduced tissue inflammation, and significantly reduced morbidity and mortality compared to untreated controls. Human short-term studies, including the landmark Abrams 2003 trial, found no significant increase in viral load or decrease in CD4+ counts in PLWH receiving stable ART who smoked cannabis or took oral THC for up to 21 days.
- Source: PMC – Cannabinoid Neuroimmune Modulation of SIV Disease
- Source: NCBI – Cannabinoid Receptor 2-Mediated Attenuation of CXCR4-Tropic HIV Infection in Primary CD4+ T Cells
The Clinical Evidence: What Research Shows Symptom by Symptom
HIV-Related Neuropathic Pain (HRNP) — The Strongest Evidence
HIV-related sensory neuropathy affects an estimated 30–50% of people living with HIV, including many on suppressive ART. It typically presents as symmetric, sleeve-like burning, aching, or shooting pain in the feet and lower legs, often with allodynia (pain from non-painful stimuli like light touch or bedsheets). It is frequently undertreated and poorly responsive to standard neuropathic pain agents.
This is the symptom where cannabis has its clearest, most rigorous clinical evidence in PLWH.
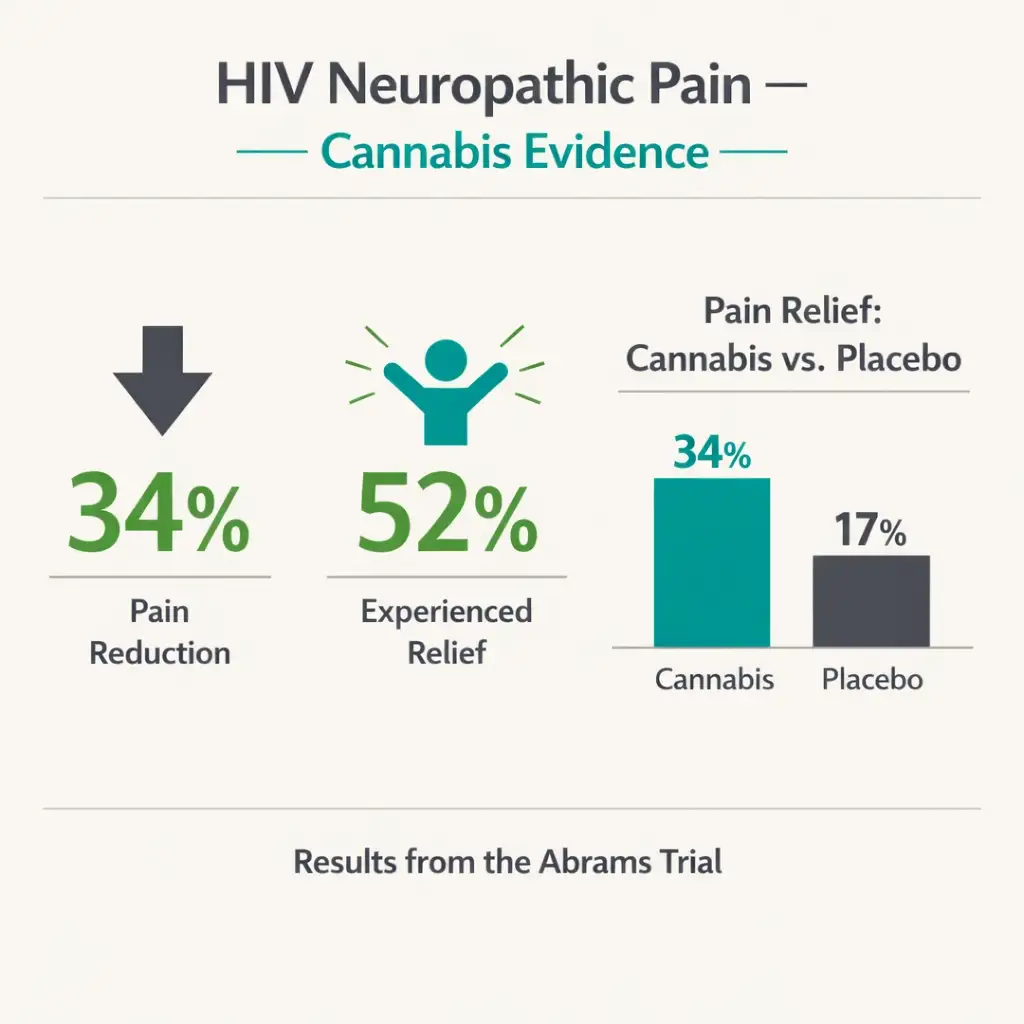
Abrams et al. (2007, Neurology): The landmark randomized, double-blind, placebo-controlled crossover trial. 50 patients with HIV-associated sensory neuropathy were randomized to smoked cannabis (3.56% THC) or placebo cigarettes, 3–4 times daily for 5 days each in a residential clinical setting. Cannabis reduced chronic neuropathic pain by a median of 34% compared to 17% for placebo, a statistically significant difference. 52% of cannabis recipients achieved greater than 30% pain reduction (a clinically meaningful threshold) versus 24% with placebo.
Ellis et al. (2009, JNCI): A second independent residential randomized, placebo-controlled crossover trial in 28 PLWH with neuropathic pain confirmed the finding. Smoked cannabis again significantly reduced pain versus placebo, with a similar effect size.
How these results rank in context: A 2010 systematic review and meta-analysis of all pharmacological treatments for HIV-associated sensory neuropathy in JAMA found that, among all tested interventions, including amitriptyline, gabapentin, pregabalin, mexiletine, lamotrigine, and multiple others, only three demonstrated superiority over placebo: smoked cannabis (NNT 3.38), topical capsaicin 8%, and recombinant human nerve growth factor (rhNGF). The conventional neuropathic pain agents failed to beat placebo. Smoked cannabis and topical capsaicin 8% are the only two clinically available treatments with RCT evidence for HRNP.
A 2023–2024 Canadian cannabis expert panel clinical guidance document, informed by a systematic literature review, specifically recommended cannabis for HIV patients with chronic neuropathic pain based on the Abrams and Ellis RCTs.
The limitation: these trials used smoked cannabis in inpatient settings. PA dispensary products cannot be smoked, vaporization of dry leaf is permitted, and oral oils/tinctures are available. Oral/vaporized formulations were not tested in the HRNP trials. The effect size of oral THC for neuropathic pain is generally lower than inhaled. This does not eliminate the case for cannabis, it is a known limitation patients should discuss with their prescribing physician.
- Source: PubMed – Cannabis in Painful HIV-Associated Sensory Neuropathy: A Randomized Placebo-Controlled Trial (Abrams et al., Neurology 2007)
- Source: PMC – Smoked Medicinal Cannabis for Neuropathic Pain in HIV (Ellis et al., JNCI 2009)
- Source: PubMed – Pharmacological Treatment of Painful HIV-Associated Sensory Neuropathy: Systematic Review and Meta-Analysis (Phillips et al., 2010)
Appetite, Weight, and Wasting
Dronabinol (Marinol/Syndros) — synthetic oral THC was FDA-approved in 1985 specifically for anorexia associated with weight loss in AIDS patients. This is a critically important fact for PA patients: a prescription for dronabinol for HIV-related appetite loss is available from any licensed physician, requires no MMJ card, and may be covered by insurance. Dronabinol (Marinol capsules, Syndros liquid) should be discussed with the treating HIV provider before pursuing dispensary cannabis for appetite concerns.
What dronabinol’s RCT evidence shows: in the pivotal trials, dronabinol improved patient-reported appetite, reduced nausea, and produced modest weight gain versus placebo over 6 weeks. However, a head-to-head comparison trial found that megestrol acetate produced significantly more weight gain than dronabinol as a primary endpoint, though dronabinol had less metabolic toxicity.
For patients already on ART who do not qualify for or tolerate dronabinol, dispensary cannabis products may provide similar appetite stimulation via THC-dominant tinctures or capsules. A 2022 residential laboratory study found both smoked cannabis and dronabinol at 10–20 mg doses significantly increased caloric intake in HIV-positive marijuana smokers.
Viral load and CD4 safety reassurance: A 2024 University of Utah evidence review (Utah Cannabis Research Review Board) summarized the available controlled trials. Oral THC/CBD combination capsules administered for 12 weeks in PLWH on stable ART were not associated with significant changes in HIV viral load or CD4+/CD8+ lymphocyte counts from baseline.
This is an important safety data point: for patients and prescribers concerned that cannabis might compromise immune status, short-to-medium term use appears immunologically safe in virally suppressed individuals on modern ART.
- Source: NCBI StatPearls – Dronabinol (Updated September 2023)
- Source: Syndros – FDA-Approved Liquid THC for AIDS-Related Anorexia
- Source: University of Utah CRRB – Evidence Review: Cannabis in HIV/AIDS (July 2024)
Nausea and GI Side Effects
Modern ART regimens are generally well-tolerated compared to earlier generations of antiretroviral drugs, but nausea, diarrhea, and GI discomfort remain common, particularly early in treatment, or when regimens are switched. Cannabis has well-documented antiemetic activity via CB1 receptors in the brainstem dorsal vagal complex. THC-dominant products taken before ART doses may help with treatment-associated nausea. The evidence for cannabis-related nausea control is strongest in chemotherapy-induced nausea, but the mechanism is shared.
Sleep, Anxiety, and Psychological Distress
PLWH experience significantly higher rates of anxiety disorders, depression, PTSD, and insomnia compared to the general population, driven by a combination of chronic disease burden, stigma, comorbidities, and the psychological weight of long-term management.
Cannabis addresses sleep and anxiety via mechanisms independent of the HIV-specific evidence, and these are among the most common reported reasons for cannabis use among PLWH. Survey data from the Multicenter AIDS Cohort Study / Women’s Interagency HIV Study found that cannabis users with HIV more frequently cited relief from psychological distress and sleep assistance as primary motivations.
PA patients with HIV who also qualify under the anxiety disorders pathway may consider pursuing certification under both qualifying conditions, which is permitted allowing the certifying physician to discuss the full symptom picture.
The ART Drug Interaction Section: What Every PA Patient on HIV Treatment Must Know
This section is the most clinically important content on this page and the section most completely absent from every competing Pennsylvania MMJ website. Cannabis (particularly CBD, and to a lesser extent THC) is metabolized through the cytochrome P450 enzyme system.
Many antiretroviral medications are either inhibitors or inducers of CYP3A4, CYP2C19, and related enzymes. The class of ART a patient is taking determines their interaction risk profile entirely.
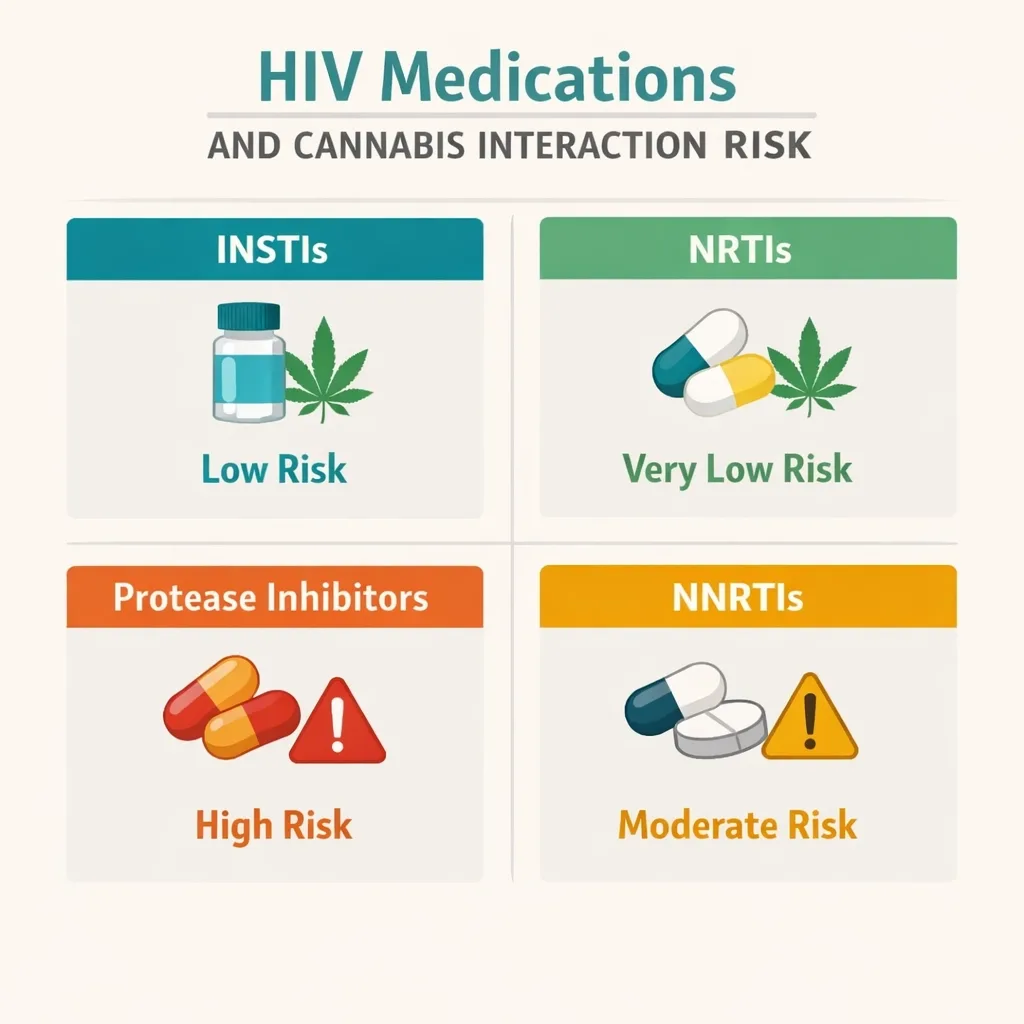
ART Class Risk Stratification for Cannabis Co-Administration
Integrase Strand Transfer Inhibitors (INSTIs) – LOWEST INTERACTION RISK
This is the most important class to understand because INSTIs are now the preferred first-line backbone of virtually all modern ART regimens.
- Dolutegravir (Tivicay; also in Triumeq, Dovato, Juluca): Metabolized primarily by UGT1A1 with only 10–15% via CYP3A4. Dolutegravir does not inhibit or induce CYP450 enzymes at clinically relevant concentrations. Cannabis interactions are not expected to be clinically significant. The University of Liverpool HIV Drug Interactions database rates the dolutegravir-cannabis interaction as unlikely to be clinically significant.
- Bictegravir (Biktarvy): Metabolized equally by UGT1A1 and CYP3A4. No significant inhibition or induction of CYP enzymes. Low interaction risk.
- Raltegravir (Isentress): Metabolized primarily by UGT1A1. Minimal CYP involvement. Low interaction risk.
- Cabotegravir (Vocabria, Apretude): No clinically significant CYP interactions expected.
Practical implication: The majority of PA patients living with HIV on first-line modern ART, Biktarvy, Triumeq, Dovato, or injectable cabotegravir/rilpivirine, have the lowest ART-cannabis interaction risk of any regimen class. For these patients, the pharmacokinetic interaction concern is substantially reduced, though not entirely absent.
Nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NRTIs) — VERY LOW INTERACTION RISK
NRTIs (tenofovir disoproxil fumarate, tenofovir alafenamide, emtricitabine, lamivudine, abacavir, zidovudine) are not significantly metabolized by CYP450 pathways. They do not inhibit or induce CYP enzymes. Cannabis is not expected to alter NRTI plasma levels meaningfully, and NRTIs are not expected to alter cannabis cannabinoid levels. This is one of the safest classes for co-administration from a pharmacokinetic standpoint.
Protease Inhibitors (PIs) with Boosting Agents — SIGNIFICANT INTERACTION RISK — REQUIRES MONITORING
This is the highest-risk ART class for cannabis co-administration, and the most important one to discuss with an HIV provider.
Ritonavir (Norvir) and cobicistat (Tybost) are pharmacokinetic boosting agents used in combination with protease inhibitors. Both are potent CYP3A4 inhibitors, their entire clinical purpose is to slow the metabolism of the co-administered PI, raising its plasma level. This same CYP3A4 inhibition also slows the metabolism of cannabinoids.
- Ritonavir-boosted PIs (darunavir/ritonavir — Prezista/Norvir; lopinavir/ritonavir — Kaletra): Co-administration with cannabis can significantly increase CBD and THC plasma levels, extending their duration of action and potentially intensifying their effects and side effects. Patients may experience greater psychoactive effects, more sedation, or cardiovascular effects (tachycardia, hypotension) at cannabis doses that previously produced minimal effects.
- Cobicistat-boosted regimens (darunavir/cobicistat — Prezcobix; elvitegravir/cobicistat — Stribild, Genvoya): Same CYP3A4 inhibition mechanism. Same elevated cannabinoid plasma level concern.
- Monitoring required: If a patient on a boosted PI regimen wants to use cannabis, they should start with the lowest available dose, titrate slowly, and be alert for amplified effects. Their HIV provider should be informed.
Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs) — MODERATE INTERACTION RISK — OPPOSITE DIRECTION
NNRTIs present a different pharmacokinetic challenge. Rather than inhibiting CYP3A4 (like boosted PIs), most NNRTIs induce CYP3A4, increasing enzyme activity and accelerating the metabolism of co-administered drugs.
- Efavirenz (Sustiva; also in Atripla): A potent CYP3A4 inducer. Co-administration with cannabis may significantly reduce cannabinoid plasma levels — meaning patients may get less effect from the same cannabis dose. Additionally, efavirenz itself has well-known CNS side effects (vivid dreams, dizziness, mood changes) that may overlap with or be compounded by THC-related CNS effects.
- Nevirapine (Viramune): CYP3A4 inducer. Similar cannabinoid-level reduction concern.
- Rilpivirine (Edurant; also in Complera, Odefsey, Juluca): CYP3A4 substrate but weaker interaction profile than efavirenz/nevirapine. Lower risk.
- Doravirine (Pifeltro, Delstrigo): Weaker CYP3A4 interaction profile; lower risk.
The practical consequence for NNRTI patients: If you are on efavirenz or nevirapine and find that cannabis has a reduced or inconsistent effect, the enzyme induction from your ART may be responsible. Do not escalate cannabis doses rapidly without consulting your HIV provider.
The University of Liverpool HIV Drug Interactions Checker
The most comprehensive, continuously updated resource for specific ART-cannabis interactions is the University of Liverpool HIV Drug Interactions database at www.hiv-druginteractions.org. This free, searchable tool allows patients and providers to enter specific ART medications and see the current interaction rating for cannabis alongside a clinical summary. Before starting or changing cannabis use, running your complete ART regimen through this tool, or asking your HIV pharmacist or provider to do so, is best practice.
- Source: NIH clinicalinfo.hiv.gov – Drug-Drug Interactions: Overview
- Source: PMC – A Review of the Toxicity of HIV Medications II: Interactions with Drugs and CAM Products
- Source: Aidsmap – Interactions Between HIV Medication and Recreational Drugs
Telling Your HIV Provider: Why This Conversation Matters
People living with HIV sometimes avoid disclosing cannabis use to their HIV providers out of concern about judgment or stigma. This is understandable but it matters clinically in ways that go beyond interaction risk.
ART adherence: Cannabis use in PLWH is associated in some studies with improved ART adherence (through reduction of side effects and psychological distress) and in others with missed doses. Your HIV provider can help you structure cannabis use around your ART schedule in a way that supports rather than disrupts consistent dosing.
Drug screen interpretations: Some clinical monitoring protocols for PLWH include urine toxicology. Your provider needs to know you’re a registered PA MMJ patient so a positive cannabis screen is properly contextualized.
Comprehensive symptom management: If neuropathic pain, nausea, or appetite loss drove your MMJ card application, your HIV provider may also have medical management options for those symptoms that work alongside rather than instead of cannabis, including referral to pain management, adjustment of your ART regimen if neurotoxic agents are implicated, or prescription dronabinol.
Full medication review: Your PA MMJ certifying physician and your HIV provider should both have your complete and current medication list, every ART drug by its actual name (not just “my HIV meds”), every dose, every other prescription, OTC medication, and supplement.
PA Dispensary Product Guidance for HIV Patients
For neuropathic pain (HRNP): The strongest evidence comes from inhaled THC. PA dispensary options include vaporizable dry leaf (the closest delivery route to the smoked cannabis studied in the RCTs) and vaporizer cartridges. Oral tinctures and capsules will have slower onset and different bioavailability but are appropriate for patients who prefer non-inhaled routes. THC-dominant or balanced THC:CBD products at low-to-moderate doses are the evidence-based starting point. Start low, 2.5–5 mg THC equivalent and titrate slowly.
For appetite stimulation: THC-dominant oral products (tinctures, capsules) taken 30–60 minutes before meals are the most common approach. This mirrors the dronabinol mechanism. CBD-dominant products are not appetite-stimulating via the same pathway.
For nausea and GI side effects: THC-dominant products, often sublingual tinctures for faster onset, taken before anticipated nausea onset (i.e., shortly before taking ART with food). Start with very low doses.
For anxiety, sleep, and psychological distress: CBD-dominant products or low-THC balanced formulations are generally preferred. High-THC products can exacerbate anxiety in some users. For sleep, moderate THC doses taken 1–2 hours before sleep (with slower-onset oral formats) are commonly reported effective.
For patients on boosted PI regimens (ritonavir or cobicistat): Start substantially lower than standard dispensary starting doses. The boosting effect on CYP3A4 may meaningfully increase cannabinoid plasma exposure. Titrate with extra caution.
How to Get Your Pennsylvania Medical Marijuana Card if You Are HIV-Positive
Step 1 — Prepare Your Documentation
Have documentation of your HIV-positive status available, either from your HIV provider, an infectious disease specialist, or primary care physician managing your HIV. This can include a recent lab report showing HIV RNA (viral load) or CD4 count, a letter from your provider, or other standard documentation of your diagnosis. Have your complete and current ART medication list ready, including each drug by name and dose.
Step 2 — Physician Certification (Telehealth)
Schedule a telehealth appointment with a PA DOH-registered medical marijuana physician. The evaluation typically takes 10–15 minutes. The certifying physician confirms your qualifying diagnosis and discusses the symptoms you intend to address. Bring your full medication list. The physician will flag any high-risk interactions (especially boosted PI regimens) and advise on starting doses and monitoring.
Step 3 — State Registration
After certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com) with your certification, a valid PA driver’s license or state-issued ID, and the $50 annual registration fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC, programs that many low-income PLWH may qualify for.
Step 4 — Dispensary Visit
At the dispensary, tell the pharmacist you have HIV and describe your primary symptom target. Share your ART medication list, or at minimum identify your ART class (INSTI, NNRTI, PI/boosted PI, NRTI). A dispensary pharmacist can help select a product and dose range appropriate for your interaction risk class. For patients on boosted PIs, ask specifically for the lowest-dose products available.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Anxiety Disorder
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: I’m HIV-positive but undetectable on ART with no symptoms. Do I still qualify?
Q: Will using cannabis affect my viral load or CD4 count?
Q: My HIV provider doesn’t support cannabis. Can I still get certified?
Q: I take Biktarvy. Do I have any major drug interaction concerns with cannabis?
Q: I take Genvoya (elvitegravir/cobicistat/emtricitabine/tenofovir). What should I know?
HIV/AIDS Support Resources in Pennsylvania
AIDS Law Project of Pennsylvania (aidslawpa.org) provides free legal help on healthcare access, employment rights, housing, and public benefits for people living with HIV in Pennsylvania. They can assist with issues including medical insurance coverage, workplace protections under the ADA as it applies to HIV status, and benefits access that may affect the $50 MMJ registration fee.
Philadelphia FIGHT Community Health Centers (fight.org) is one of the primary HIV care and advocacy organizations in Pennsylvania, providing primary care, infectious disease services, pharmacy services, and behavioral health services for PLWH in Philadelphia and surrounding counties.
AIDSNET / Positive Health Center at UPMC provides HIV primary care services in western Pennsylvania and can serve as a medical home for PLWH seeking integrated symptom management including cannabis.
PA DOH HIV Prevention and Care Program: The Pennsylvania Department of Health funds HIV care coordination services statewide. Ryan White Part B and Part D funding supports services for low-income PLWH including medication assistance programs.
NIH clinicalinfo.hiv.gov provides the most comprehensive, up-to-date clinical guidance on HIV treatment, drug interactions, and comorbidity management, including the most current ART drug interaction tables.
University of Liverpool HIV Drug Interactions Checker (hiv-druginteractions.org), the gold-standard free tool for checking specific ART medication interactions with cannabis and other drugs.
NOTE: For people living with HIV in Pennsylvania, the MMJ card opens access to products that have the most rigorous evidence for two symptoms that remain poorly treated by conventional medicine: HIV-related neuropathic pain, where smoked cannabis has a lower NNT than most standard pharmaceutical options, and appetite stimulation, where THC has FDA-approved drug-level evidence going back to 1985. The interaction risks from modern INSTI-based ART are manageable and substantially lower than those from older PI-era regimens. The viral load safety data for moderate-term cannabis use in virally suppressed patients is reassuring.
What matters most is that your HIV provider and your PA MMJ certifying physician both know your complete medication list, and that you use the University of Liverpool interaction checker as a baseline tool before starting any new cannabis product. HIV in 2026 is a managed condition and cannabis, used thoughtfully with awareness of the pharmacology involved, is a legitimate tool for managing the chronic symptom burden that persists even in well-controlled disease.