
Parkinson’s disease is one of the fastest-growing neurological conditions in the world — and one of the most frustratingly undertreated. The gold-standard medication, levodopa, works well in early disease, but as the years pass it loses reliability. Patients experience ‘off’ periods where the drug stops working before the next dose is due.
They develop levodopa-induced dyskinesia: involuntary, writhing movements caused by the very treatment keeping them upright. And alongside the motor symptoms that define the diagnosis, they carry an enormous non-motor burden — sleep disorders, anxiety, depression, psychosis, chronic pain, and cognitive changes — that dopaminergic drugs often make worse, not better.
Medical cannabis has entered this gap. Between 25 and 40 percent of Parkinson’s disease patients in the United States are already using cannabis or cannabinoids — a rate two to three times higher than in the general population. Pennsylvania recognized Parkinson’s disease as a qualifying condition for its medical marijuana program from the very beginning of Act 16 in 2016. But most PA MMJ sites give Parkinson’s patients only a superficial paragraph. This page does not.
Here you will find the complete picture: the qualifying criteria, what Parkinson’s disease actually is and what makes its treatment so challenging, the unique endocannabinoid system involvement specific to PD, the honest evidence for every symptom category including what the research supports and what it does not, the critical drug interaction chapter every PD patient needs before starting cannabis, product guidance based on symptom targets, and a clear, step-by-step path to your PA MMJ card.
Does Parkinson’s Disease Qualify for Medical Marijuana in Pennsylvania?
Yes — Parkinson’s disease is a named qualifying condition under Pennsylvania’s Medical Marijuana Act.
Parkinson’s disease is explicitly listed as a qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016), as recognized by the Pennsylvania Department of Health. A confirmed PD diagnosis at any stage qualifies — there is no requirement to have reached advanced disease or to have exhausted other treatments first.
Additionally, Pennsylvania’s list includes ‘Dyskinetic and spastic movement disorders’ as a separate qualifying category — meaning that Parkinson’s patients whose primary burden is levodopa-induced dyskinesia or movement-related complications may qualify under this category as well, giving them additional qualifying pathways if needed.
The qualification is straightforward:
- Any stage of Parkinson’s disease qualifies — from early diagnosis through advanced disease
- All Parkinson’s subtypes qualify (idiopathic PD, drug-induced parkinsonism, Parkinson’s-plus syndromes)
- No requirement to have failed specific medications
- Caregivers of PD patients who cannot independently manage their medical care can register and obtain cannabis on their behalf
- Early-onset Parkinson’s disease (diagnosed before age 50) qualifies identically to later-onset PD
Sources:
- Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Marijuana Policy Project – Pennsylvania Medical Marijuana Law Guide
Parkinson’s Disease in Pennsylvania and the United States: The Scale
Before examining what cannabis can do for Parkinson’s disease, it is worth understanding who this page is written for. Parkinson’s disease is the second most common neurodegenerative disorder after Alzheimer’s disease, and it is growing faster than almost any other neurological condition.
Nationally, an estimated 1.1 million Americans are currently living with Parkinson’s disease, a number projected to reach 1.2 million by 2030. Nearly 90,000 new diagnoses occur every year in the United States — a figure 1.5 times higher than previously estimated. The combined direct and indirect cost of Parkinson’s in 2024 was calculated at $82.2 billion. The Parkinson’s Foundation has identified Central Pennsylvania as a region of elevated PD incidence, placing Pennsylvania residents at disproportionate risk.
Critically for this guide: a nationwide survey of over 1,000 PD patients published in npj Parkinson’s Disease found that approximately 25% reported cannabis use within the prior six months. Other sources estimate 25–40% of US PD patients use cannabis — a rate two to three times higher than in the general population. PA MMJ patients with Parkinson’s are not an exception to a trend. They are at the center of it.
Sources:
- Parkinson’s Foundation – Statistics
- npj Parkinson’s Disease – Weeding Through the Haze: A Survey on Cannabis Use in US PD Patients
- PubMed – Cannabis Use in Parkinson’s Disease: Patient Access and Physician Perspective (2024)
What Is Parkinson’s Disease? Why Treatment Is So Difficult
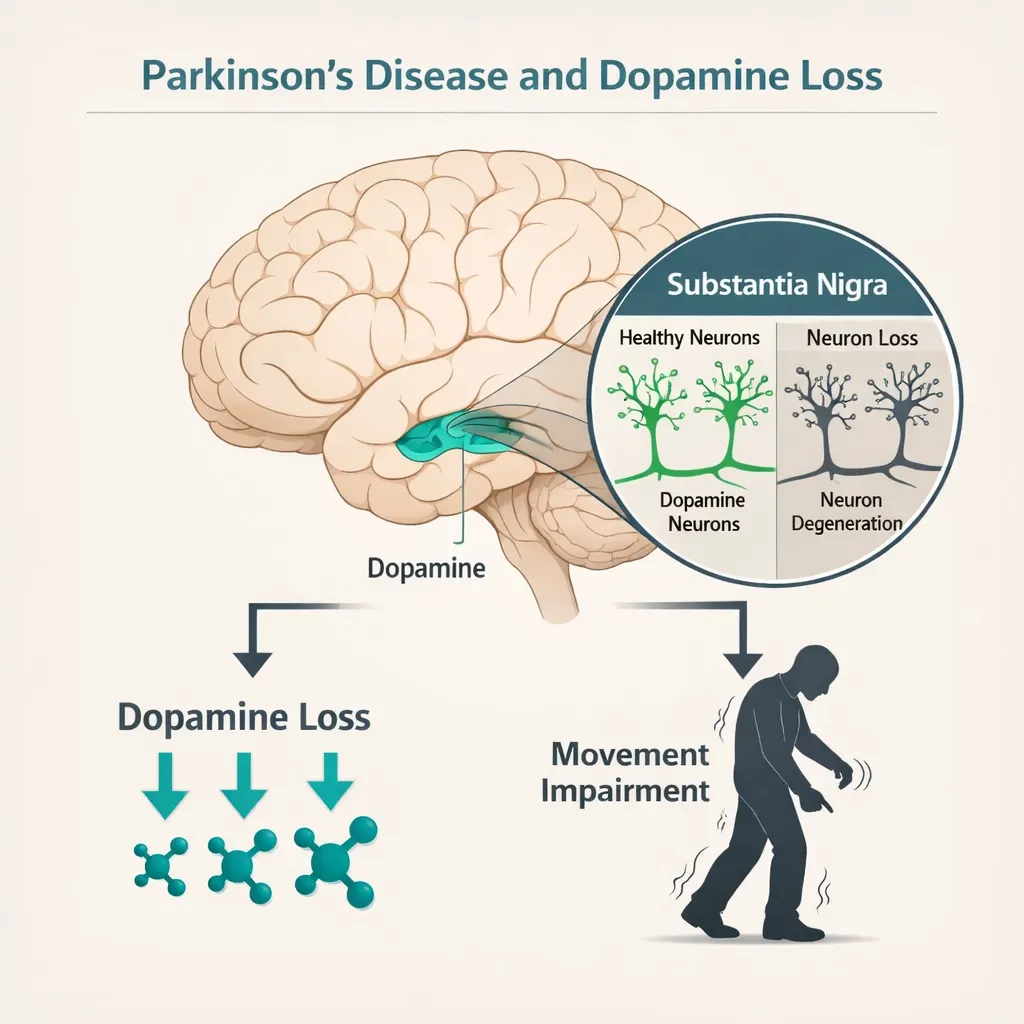
Parkinson’s disease is a progressive neurodegenerative disorder caused by the loss of dopamine-producing neurons in the substantia nigra — a region of the brainstem critical for movement control. As these neurons die, striatal dopamine levels fall, producing the cardinal motor features of PD: resting tremor, rigidity (stiffness), bradykinesia (slowness of movement), and postural instability.
But PD is far more than a movement disorder. Non-motor symptoms are present in nearly all patients and often precede motor diagnosis by years. In many patients, non-motor symptoms are more disabling than the motor deficits.
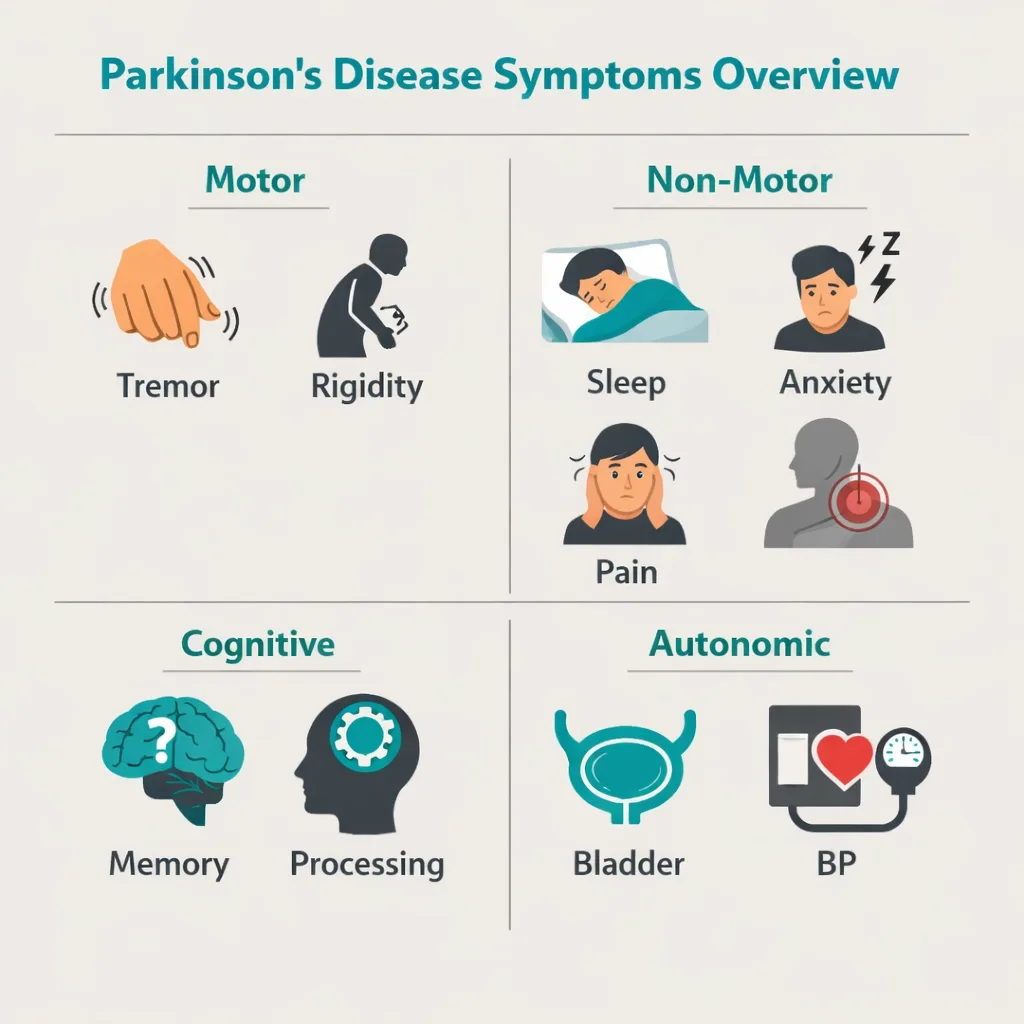
The Full Symptom Burden of Parkinson’s Disease
| Symptom Category | What It Includes |
|---|---|
| Motor symptoms | Resting tremor, rigidity, bradykinesia, postural instability, freezing of gait, dysarthria (speech), dysphagia (swallowing) |
| Levodopa complications | Levodopa-induced dyskinesia (involuntary movements), motor fluctuations with ‘on/off’ periods, wearing-off effect |
| Sleep disorders | REM sleep behavior disorder (RBD), insomnia, excessive daytime sleepiness, restless legs syndrome, sleep fragmentation |
| Psychiatric / behavioral | Depression (affects ~40% of PD patients), anxiety (~40%), apathy, impulse control disorders (from dopamine agonists) |
| Psychosis | Hallucinations and delusions affect up to one-third of PD patients, especially in later stages; worsened by antiparkinsonian drugs |
| Pain | Musculoskeletal pain, dystonic pain, central neuropathic pain — affects 40–85% of PD patients |
| Cognitive | Executive function decline, processing speed, memory impairment; approximately 30% develop dementia over time |
| Autonomic | Constipation, urinary urgency, orthostatic hypotension, sexual dysfunction, drooling (sialorrhea) |
The Levodopa Problem That Cannabis Research Directly Addresses
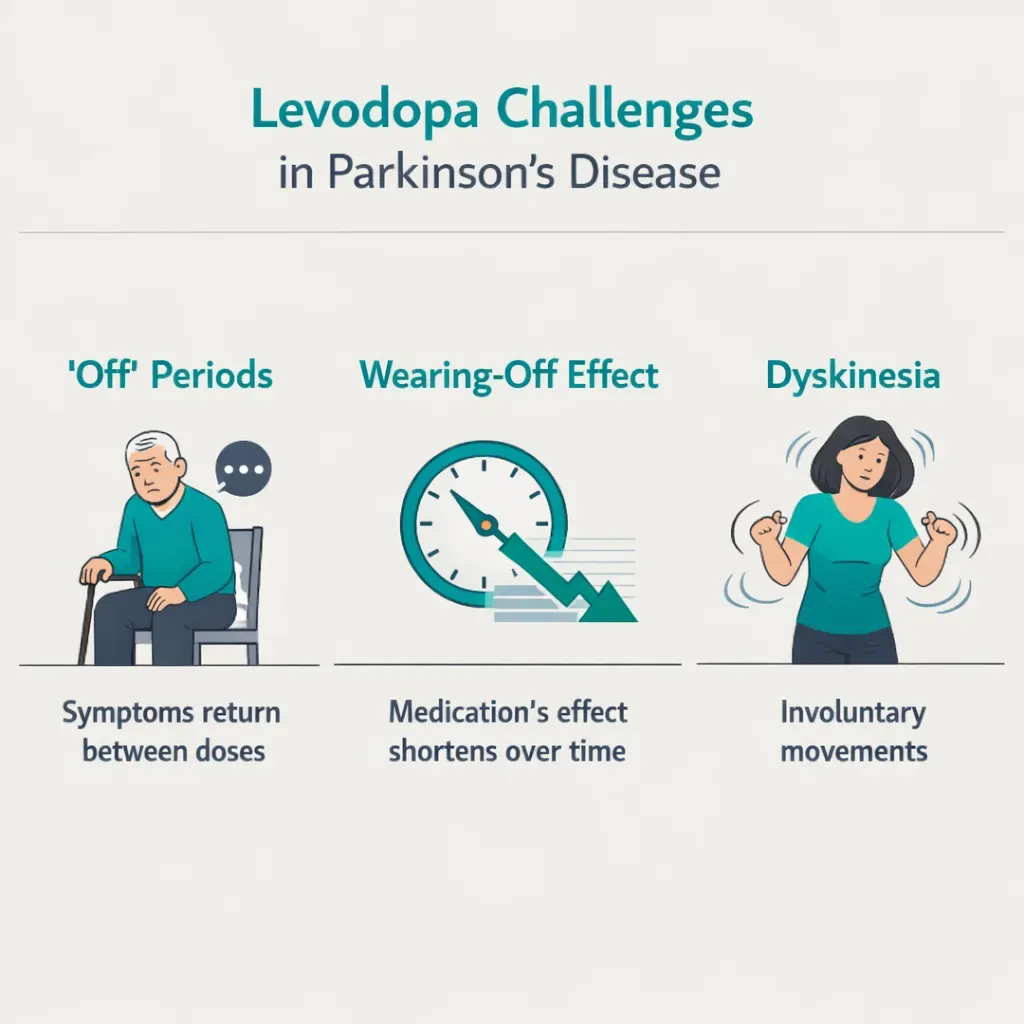
Levodopa remains the gold standard for motor symptom control. But two major complications make long-term levodopa management increasingly difficult for many patients:
Motor fluctuations: As PD progresses, levodopa’s effect becomes less reliable and shorter-lasting. Patients experience ‘off’ periods — windows before the next dose when motor symptoms return, sometimes severely. Managing off-time is one of the most challenging aspects of advanced PD care.
Levodopa-induced dyskinesia (LID): Approximately 25% of patients develop LID within a few years of starting levodopa therapy. After ten years, prevalence rises to as high as 80%. LID consists of involuntary, often dramatic writhing movements that can be as disabling as the underlying PD symptoms. The only FDA-approved treatment specifically for LID is amantadine — which has its own significant side effects. This unmet need is one reason cannabis research in PD has focused heavily on dyskinesia.
It is also important to understand that dopaminergic medications — levodopa and dopamine agonists — do not adequately treat non-motor symptoms and in some cases worsen them. Anxiety, psychosis, and cognitive effects may all be exacerbated by standard PD medications. This is the clinical gap that cannabis research in PD is most actively trying to fill.
Sources:
- Parkinson’s Foundation – Medical Marijuana
- Frontiers in Aging Neuroscience – Levodopa-Induced Dyskinesia: An Updated Review (2025)
The Endocannabinoid System in Parkinson’s Disease: Why the Biology Matters
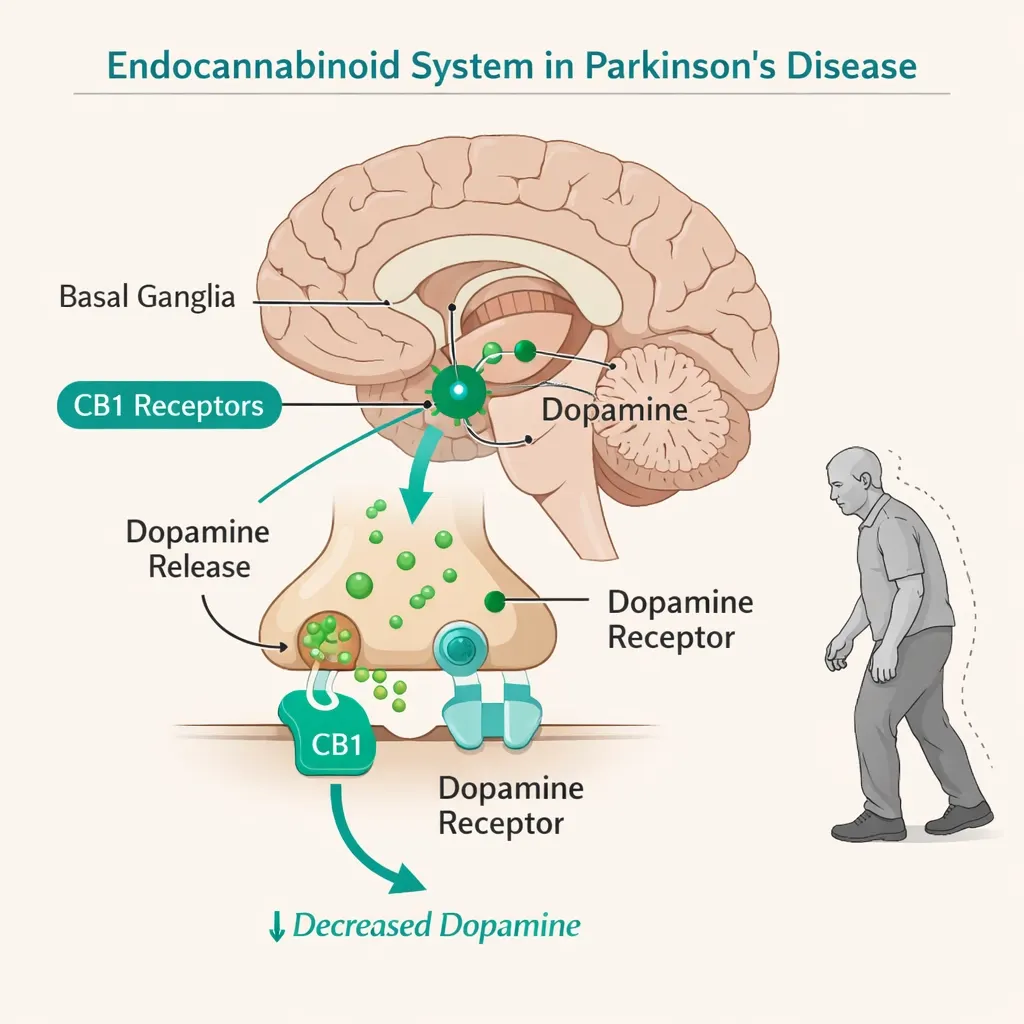
Parkinson’s disease is not just tangentially connected to the endocannabinoid system. The ECS is deeply embedded in the basal ganglia circuits that PD destroys, and the dopaminergic and endocannabinoid systems are tightly coupled through direct receptor interactions in the striatum.
CB1 Receptors in the Basal Ganglia
CB1 receptors are expressed at extremely high density throughout the basal ganglia — the network of brain structures responsible for movement initiation and coordination that is the primary site of PD pathology. This is not coincidental. CB1 receptor activation in the striatum modulates dopamine and glutamate signaling, reduces excitotoxicity, and plays a direct role in regulating movement.
In Parkinson’s disease, the loss of dopaminergic neurons disrupts normal ECS-dopamine crosstalk in the striatum. This disruption contributes to both the motor symptoms of PD and to the abnormal striatal plasticity that underlies levodopa-induced dyskinesia. Research has established that when dopamine depletion occurs, CB1 signaling in the striatum is significantly reorganized — a finding with direct therapeutic implications, as modulating this system with external cannabinoids may help restore balance.
CB2 Receptors and Neuroinflammation
CB2 receptors, primarily expressed on microglial cells (the brain’s immune cells), are upregulated in the substantia nigra of PD patients — a response to the ongoing neuroinflammation that drives dopaminergic neuron death. Activating CB2 receptors reduces microglial activation and the release of pro-inflammatory cytokines. This is the biological basis for studying cannabinoids as potential neuroprotective agents in PD.
CBD’s Multiple Non-Cannabinoid Receptor Mechanisms
Unlike THC, CBD does not primarily act through CB1 or CB2 receptors. CBD’s relevance to PD comes from its effects on multiple other targets:
- TRPV1 receptor activation — providing analgesic and anti-inflammatory effects
- PPARgamma activation — reducing neuroinflammation and potentially promoting hippocampal neurogenesis
- Serotonin receptor (5-HT1A) partial agonism — producing anxiolytic and antidepressant effects
- Alpha-synuclein modulation — preclinical evidence suggests CBD may reduce alpha-synuclein aggregation, one of the core pathological processes in PD
- Antioxidant properties — reducing oxidative stress, a key driver of dopaminergic neuron death in PD
The 2025 systematic review of CBD and Parkinson’s disease (Cannabidiol and Parkinson’s Disease: Investigating Receptor Interactions, ScienceDirect) concluded that these cellular-level effects directly target dysfunctions that contribute to dopaminergic neurodegeneration and disease progression, and strongly support continued investigation of CBD as a candidate for disease-modifying intervention in PD.
Sources:
- PMC – CBD’s Potential Impact on Parkinson’s Disease: An Updated Overview (2024)
- ScienceDirect – Cannabidiol and Parkinson’s Disease: Investigating Receptor Interactions (2025)
- PMC – Marijuana Compounds: A Nonconventional Approach to Parkinson’s Disease Therapy
What the Clinical Research Shows: Honest Evidence for Every Symptom
This is where most PA MMJ sites fail Parkinson’s patients. The evidence for cannabis in PD is genuinely mixed — strong for some symptoms, weak or absent for others — and patients deserve to know which is which before making treatment decisions. Here is the honest picture, symptom by symptom.
The Position of Major PD Organizations
The Parkinson’s Foundation, American Parkinson Disease Association (APDA), and Michael J. Fox Foundation (MJFF) all hold measured positions on cannabis: they recognize potential benefits for quality of life, non-motor symptoms, and specific complications, but emphasize that more rigorous clinical trials are needed and that cannabis should not replace dopaminergic therapy. The consensus: cannabis as adjunctive therapy for specific unmet symptoms, not as a standalone PD treatment.
Motor Symptoms: Tremor, Rigidity, and Bradykinesia — Mixed Evidence
This is where patient experience and controlled trial data diverge most sharply — and where honesty matters most.
In self-report and observational studies, cannabis produces promising motor signal. A survey of 339 PD patients found significant improvement in general PD symptoms in 46% of cannabis users: 31% reported tremor improvement, 38% reported relief from rigidity, and 45% reported reduced bradykinesia. Higher THC metabolite levels in urine were associated with greater symptom relief, suggesting dose-dependence. A separate study of 22 PD patients using smoked cannabis showed statistically significant improvement in tremor, rigidity, and bradykinesia 30 minutes after use — with relief lasting up to 3 hours. A 2023 retrospective chart review of 69 PD patients using cannabis reported improvements in tremor, spasticity, and dystonia.
However, the randomized controlled trial data tells a more cautious story. The 2022 systematic review and meta-analysis published in the Journal of Parkinson’s Disease (Urbi et al.) analyzed 5 RCTs and 18 non-randomized studies. The conclusion: no compelling evidence was found to recommend cannabis for PD motor symptoms in controlled settings. The meta-analysis of RCTs did not demonstrate statistically significant improvement in UPDRS motor scores. The 2021 PMC meta-analysis of 6 RCTs (133 total patients) similarly found no significant motor improvement in controlled studies despite observational data suggesting benefit.
The Honest Summary on Motor Symptoms
Observational data and patient reports consistently suggest motor benefit for a subset of PD patients, particularly for tremor and rigidity. Controlled trials have not confirmed this at a population level. The discrepancy likely reflects individual variability, dose and formulation differences across studies, and the challenge of measuring motor symptoms objectively in heterogeneous populations. Cannabis does not reliably substitute for levodopa on motor symptoms. Some patients experience clear benefit; others do not. Starting low and titrating cautiously is the appropriate approach.
Levodopa-Induced Dyskinesia (LID) — A Genuinely Promising Target
Levodopa-induced dyskinesia may be the most scientifically compelling motor target for cannabis in PD — and it is one of the most underserved areas in PD pharmacology.
Nabilone, a synthetic CB1 agonist similar to THC, produced a 22% reduction in levodopa-induced dyskinesia in a controlled PD trial. In a separate study, oral nabilone significantly reduced dyskinesia without aggravating parkinsonism in seven PD patients with severe LID. The CB1 receptor mechanism for anti-dyskinetic effects is well established in animal models: cannabinoid agonists reduce the abnormal involuntary movements associated with pulsatile levodopa exposure through striatal CB1 modulation.
The contradictory data comes from Carroll et al.’s randomized crossover trial of oral cannabis extract in 19 PD patients, which found no improvement in dyskinesia. This negative result is often cited, but it used an oral cannabis extract formulation and may not reflect results with THC-dominant tinctures or vaporized formulations. The Parkinson’s Foundation acknowledges that cannabinoids reducing LID is a clinically plausible mechanism, though calling for more definitive evidence.
Current status: promising preclinical and small-scale human data, no definitive large RCT. Among PA dispensary-accessible products, THC-dominant formulations timed to levodopa doses represent the most plausible approach for patients seeking anti-dyskinetic benefit.
Sleep Disorders — Among the Strongest Non-Motor Evidence
Sleep disorders are nearly universal in Parkinson’s disease and are among the most impactful on quality of life. REM sleep behavior disorder (RBD), insomnia, restless legs syndrome, and nighttime motor symptoms all contribute to fragmented, unrestorative sleep. Standard sleep medications are problematic in PD — benzodiazepines worsen motor coordination, and most alternatives have inadequate evidence.
Cannabis has produced some of the most consistent and encouraging results in PD for this target:
- A case series by Chagas et al. found that CBD (75–300 mg/day) improved complex sleep-related behaviours associated with REM sleep behavior disorder in four PD patients, with significant reduction in RBD symptoms.
- A 2025 case series using THC:CBD cannabis extracts showed significant improvement in insomnia in PD patients after approximately 60 days of treatment.
- A 2024 case series (Frontiers in Human Neuroscience) of low-dose cannabis extracts in PD patients found improvements in non-motor symptoms including sleep.
- The nationwide PD cannabis survey found sleep disorders among the most commonly reported symptoms improved with cannabis use.
- The 2025 French nationwide survey of PD cannabis users found sleep disorders were among the most commonly reported areas of improvement.
The sleep evidence in PD is among the most consistently positive in the cannabis-PD literature, and it is clinically meaningful given the near-universal sleep burden in this population.
Psychosis — CBD’s Most Distinctive and Well-Supported Role in PD
PD-related psychosis — affecting up to one-third of patients, with some estimates as high as 50% in later stages — is one of the most challenging management problems in neurology. Conventional antipsychotics worsen motor symptoms. The only FDA-approved treatment for PD psychosis (pimavanserin) is expensive and has its own limitations. CBD’s potential here is genuine and represents one of its most unique therapeutic opportunities in PD.
Zuardi et al. conducted an open-label pilot study of CBD (150–400 mg/day) in six PD patients with psychotic symptoms for at least 3 months. Results showed significant decreases in psychotic symptoms on both the Brief Psychiatric Rating Scale and the Parkinson Psychosis Questionnaire, with no influence on cognitive or motor function and no severe side effects. This study, while small, is the first controlled evidence that CBD reduces PD psychosis.
The UK’s CAN-PDP trial is currently evaluating CBD specifically for Parkinson’s disease psychosis. Animal and human data consistently suggest CBD has antipsychotic effects and is well tolerated in PD populations. Multiple reviews have concluded that CBD’s antipsychotic profile without motor side effects makes it uniquely suitable for PD psychosis management compared to conventional antipsychotics.
For PA patients: CBD-dominant products represent a particularly rational choice for PD patients experiencing hallucinations or delusions, and should be discussed with the treating neurologist as a potential adjunct or alternative to conventional antipsychotic agents.
Anxiety and Depression — Strongly Supported Targets
Anxiety affects approximately 40% of PD patients. Depression affects a similar proportion. Both are frequently undertreated, partly because available medications have motor side effects or interaction concerns in PD. Cannabis has well-established evidence for anxiety and mood in the broader clinical literature.
In PD-specific research: a double-blind trial of CBD (75 mg and 300 mg) in 21 PD patients found no significant improvement in UPDRS motor scores but showed improved quality of life scores at 300 mg, measured by the PDQ-39. The 2023 retrospective chart review (Aladeen et al., Clinical Neuropharmacology) of 69 PD patients on medical cannabis found that 87% showed improvement in at least one PD symptom, with cramping/dystonia, pain, lack of appetite, and overall quality of life among the highest-response categories. A 2024 double-blind RCT evaluated CBD for cognitive and inflammatory markers in PD patients and found improvements in naming ability.
The CBD-serotonin (5-HT1A) mechanism that underpins its anxiolytic effects is particularly relevant in PD, where serotonergic dysfunction contributes significantly to both anxiety and depression.
Pain — Well-Supported and Frequently Underrecognized
Pain affects an estimated 40–85% of PD patients and is among the most undertreated PD symptoms. Dystonic pain (from sustained muscle contractions), musculoskeletal pain, and central neuropathic pain all occur in PD. The 2023 chart review found pain among the symptoms with highest rates of improvement with medical cannabis. Smoked cannabis produced statistically significant improvement in pain scores in two separate observational studies of PD patients. Cannabis has broad and well-established analgesic mechanisms relevant to all PD pain subtypes.
Long-Term Safety: What a Major Real-World Study Found
A critical question for any chronic condition is whether long-term cannabis use is safe. The landmark retrospective case-control study from the Sheba Medical Center Movement Disorders Institute (ScienceDirect, 2023) followed 152 PD patients from 2008 to 2022 — 76 using whole-plant medical cannabis for at least one year versus a matched control group not using cannabis. The findings:
- No significant differences in disease progression (Hoehn and Yahr stage) between cannabis users and non-users
- No significant differences in levodopa equivalent daily dose requirements over time
- No evidence of worsening psychotic, depressive, or cognitive symptoms in cannabis users over the study period
- Cannabis was well tolerated, with a low discontinuation rate due to adverse events
This is, to date, the largest and longest real-world safety study of medical cannabis in PD, and its results are reassuring: long-term cannabis use did not appear to accelerate disease progression or worsen cognitive, psychiatric, or motor outcomes in PD patients.
Sources:
- PubMed – Effects of Cannabis in Parkinson’s Disease: Systematic Review and Meta-Analysis (2022)
- PubMed – Medical Cannabis in the Treatment of Parkinson’s Disease (Aladeen et al., 2023)
- ScienceDirect – Long-Term Safety of Medical Cannabis in Parkinson’s Disease (2023)
- PMC – Cannabidiol in Parkinson’s Disease (PMC NIH)
- APDA – Cannabidiol and Parkinson’s Disease
- Parkinson’s Foundation – Medical Marijuana
- PMC – Cannabis and Its Derivatives for Motor Symptoms in Parkinson’s Disease: Systematic Review and Meta-Analysis
- PMC – Patterns of Use and Patient-Reported Effects of Cannabinoids in PD (France 2025)
Product Selection for Parkinson’s Patients: What the Evidence Guides
The evidence points toward clear product guidance for Parkinson’s disease — but it also reveals that different symptom targets require different cannabinoid profiles. This is the most nuanced product decision of any PA MMJ qualifying condition.
The Critical Distinction: THC vs. CBD in PD
| Factor | THC-Dominant Products | CBD-Dominant Products |
|---|---|---|
| Best for | Motor symptom relief, pain, appetite, sleep onset, dyskinesia reduction | Psychosis, anxiety, depression, REM sleep disorder, daytime management |
| Evidence level | Observational – strong; RCTs – mixed | Clinical trials for psychosis, RBD, and quality of life – positive |
| Caution | Risk of worsening confusion, hallucinations, balance problems at high doses in PD | Generally well tolerated; few PD-specific concerns at moderate doses |
| Timing | Evening/bedtime; can align with levodopa dose timing | Daytime use appropriate; can be taken throughout the day |
Specific Product Guidance by Symptom
For sleep (insomnia, nighttime motor symptoms): Low-to-moderate dose THC-dominant tincture or capsule taken 1–1.5 hours before bedtime. The highest-dose administration of the day at bedtime is a validated strategy. A 1:1 THC:CBD ratio product at bedtime may provide combined sedation and RBD benefit.
For REM sleep behavior disorder (RBD): CBD-dominant products at 75–300 mg/day (the dosing range showing benefit in Chagas et al.’s case series) represent the most evidence-aligned approach. Discuss with your neurologist before adjusting any RBD-related medications.
For PD-related psychosis or hallucinations: CBD-dominant products (100–400 mg/day range used in Zuardi et al.’s study) are the evidence-supported choice. THC-dominant products should be used with extreme caution in patients experiencing psychotic symptoms, as THC can worsen hallucinations. CBD-dominant products for psychosis should always be discussed with the treating neurologist.
For anxiety and depression (daytime): CBD-dominant products at moderate doses (50–150 mg/day) provide anxiolytic and mood-stabilizing effects via serotonin receptor mechanisms without psychoactive impairment. Appropriate for daytime use.
For pain (dystonia, musculoskeletal, neuropathic): Low-to-moderate dose THC-dominant tincture or capsule, dosed 2–3 times daily. Topical cannabis preparations may be appropriate for localized dystonic pain without systemic effects.
For dyskinesia (LID): Low-dose THC-containing products timed around levodopa administration represent the most pharmacologically rational approach. The anti-dyskinetic mechanism requires CB1 activation. Start low: 2.5–5 mg THC oral, timed 30–60 minutes before a levodopa dose when dyskinesia typically peaks.
Critical Dosing Cautions Specific to Parkinson’s Disease
Parkinson’s disease introduces specific vulnerabilities that make conservative dosing especially important:
- Balance and fall risk: THC impairs coordination. PD patients already have postural instability and are at high fall risk. Use cannabis initially while seated or in a supervised setting. Avoid high-dose THC if balance is a significant concern.
- Cognitive vulnerability: PD patients are at elevated risk for cognitive decline and dementia. High-dose THC can worsen executive function and memory. Use the minimum effective dose, especially in patients with existing cognitive impairment.
- Psychosis sensitivity: THC can precipitate or worsen hallucinations in PD patients, particularly those already on dopaminergic medications that increase psychosis risk. CBD-dominant products are significantly safer in psychosis-prone PD patients.
- Orthostatic hypotension: Both cannabis (particularly THC) and many PD medications can lower blood pressure. PD patients on levodopa or dopamine agonists who add cannabis may experience enhanced orthostatic hypotension, increasing fall and syncope risk. Monitor blood pressure and stand up slowly.
- Swallowing: Advanced PD patients with dysphagia may find sublingual tinctures more practical than capsules or tablets.
Drug Interactions: What Every PD Patient Must Know Before Starting Cannabis
⚠ Always Tell Your Movement Disorders Specialist or Neurologist Before Starting Cannabis
Cannabis has interactions with several medications commonly used in Parkinson’s disease management. These interactions are not reasons to avoid cannabis, but they require physician awareness and sometimes dose monitoring or adjustment.
Levodopa (Sinemet, Rytary, Duopa): No major pharmacokinetic interaction has been established between levodopa and cannabis. However, cannabis may influence the subjective experience of levodopa ‘on’ and ‘off’ periods, and any changes in motor status after starting cannabis should be communicated to your neurologist. Do not adjust your levodopa dose based on cannabis effects without neurologist guidance.
Dopamine agonists (pramipexole, ropinirole, rotigotine): No major CYP-mediated interaction identified. Additive sedation and orthostatic hypotension risk with THC-containing products. Monitor carefully.
MAO-B inhibitors (selegiline, rasagiline, safinamide): Selegiline is metabolized by CYP2B6 and CYP3A4. CBD inhibits CYP3A4, potentially increasing selegiline blood levels. Alert your neurologist if you are on selegiline or rasagiline before starting CBD.
COMT inhibitors (entacapone, tolcapone): No significant CYP interaction established. Use with standard monitoring.
Clozapine (used for PD psychosis): Clozapine is metabolized by CYP1A2 and CYP3A4. CBD inhibits CYP3A4. This could increase clozapine levels, raising the risk of clozapine toxicity — a serious concern given clozapine’s narrow therapeutic window. This interaction requires explicit neurologist and prescriber awareness.
Antidepressants (SSRIs, SNRIs): CBD inhibits CYP2D6 and CYP3A4. Many antidepressants are metabolized by these pathways. Levels of fluoxetine, paroxetine, venlafaxine, and others may rise when CBD is added. Monitor for increased side effects.
Warfarin: CBD significantly inhibits CYP2C9, the primary warfarin metabolizing enzyme. If you take warfarin, adding CBD requires INR monitoring and physician coordination.
The general rule for PD patients: because the PD medication regimen is often complex and precision-dosed, cannabis should be introduced one product at a time, at low initial doses, with explicit physician awareness.
How to Get Your Pennsylvania Medical Marijuana Card for Parkinson’s Disease
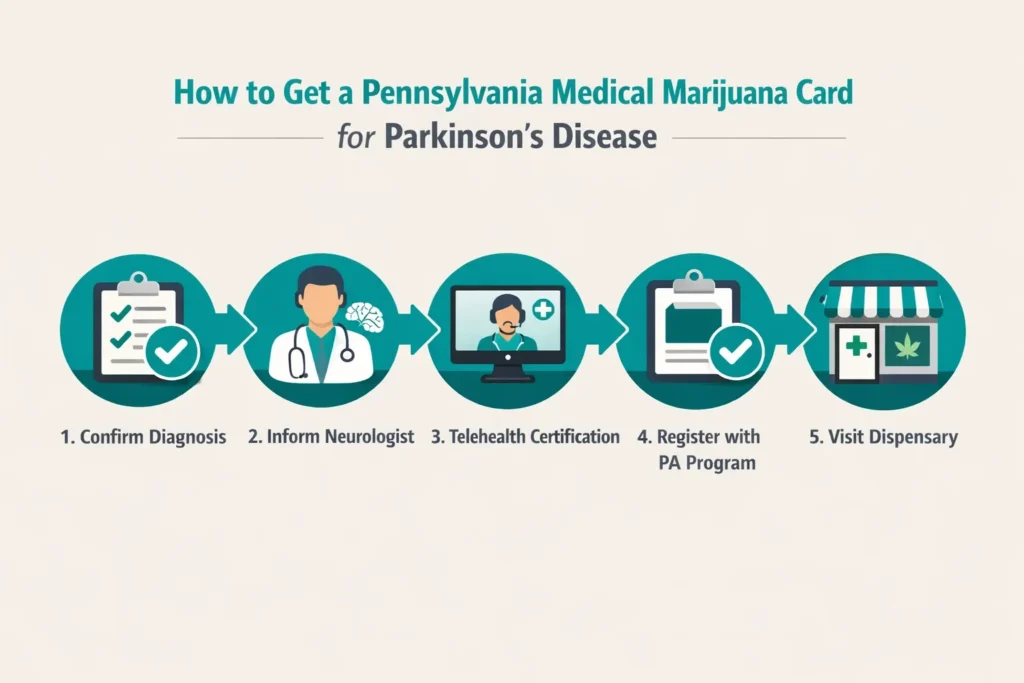
The process is straightforward, completely manageable from home, and can be completed in less than a week. Here is the specific path for Parkinson’s disease patients.
Step 1 — Tell Your Movement Disorders Specialist or Neurologist First
Before your certification appointment, tell your treating neurologist or movement disorders specialist that you are pursuing a PA MMJ card. This is not just courtesy — it is practically important. Your neurologist manages a complex medication regimen. They need to know:
- Which symptoms you are targeting with cannabis
- What products you plan to use (THC vs. CBD, dosing range)
- That they should watch for any changes in motor status, mood, sleep, or medication side effects after you begin
The long-term safety study from Sheba Medical Center found no significant problems in PD patients using cannabis, but individual variability means ongoing neurologist monitoring is important.
Step 2 — Gather Your Medical Records
Your certifying PA MMJ physician will want to confirm your PD diagnosis. Bring or have available:
- A note or visit record from your neurologist confirming the PD diagnosis
- Your current medication list (levodopa, dopamine agonists, MAO-B inhibitors, etc.)
- Any information about symptoms you are specifically hoping to address (sleep, anxiety, dyskinesia, pain, etc.)
Step 3 — PA MMJ Physician Certification (Telehealth)
Schedule a telehealth appointment with a PA DOH-registered medical marijuana physician. These 10–15 minute video appointments are conducted from your home. The certifying physician will review your diagnosis, discuss your symptoms and treatment goals, and submit your certification directly to the PA DOH registry.
✨ Ready to get your PA MMJ card for Parkinson’s disease?
Our PA DOH-registered physicians understand Parkinson’s disease and can help you identify which cannabis products are most evidence-supported for your specific symptoms — motor, non-motor, sleep, psychosis, pain, or dyskinesia.➡ [BOOK YOUR PA MMJ CERTIFICATION HERE — Insert booking link]
Step 4 — State Registration
After your physician certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com). You will need your certification, a valid PA driver’s license or state-issued ID, and the $50 annual registration fee. Fee waivers are available for Medicaid, PACE/PACENET, CHIP, SNAP, or WIC recipients. Your digital MMJ card is typically accessible within a few business days.
Step 5 — First Dispensary Visit
Tell the dispensary pharmacist you have Parkinson’s disease. Be specific about your symptom targets and which medications you currently take. A knowledgeable PD-aware dispensary pharmacist can make a substantial difference in helping you select the right product, ratio, and dosing approach. Starting with a single product at low dose is strongly recommended.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Multiple Sclerosis
- Neuropathies
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
Frequently Asked Questions
Q: Will cannabis replace my levodopa?
Q: I have PD-related hallucinations. Should I use THC or CBD?
Q: I have REM sleep behavior disorder (RBD). Can cannabis help?
Q: My PD is early stage. Is it too soon to consider cannabis?
Q: Can my caregiver manage my PA MMJ card if I can no longer do so myself?
Q: Can cannabis help with levodopa-induced dyskinesia (LID)?
A: Preclinical data and small human studies suggest cannabinoids — particularly CB1 agonists like THC — may reduce LID through striatal mechanisms. Nabilone produced a 22% LID reduction in a controlled study. The oral cannabis extract RCT (Carroll et al.) found no benefit, creating conflicting evidence. Low-dose THC-dominant products timed around levodopa doses represent a rational trial for PD patients with significant LID, undertaken with neurologist awareness and monitored carefully.
Q: Will cannabis affect my ability to drive?
A: Yes — potentially significantly. THC impairs driving-relevant functions including reaction time, tracking, and divided attention. PD itself already impairs driving ability. The combination requires serious attention. In Pennsylvania, driving under the influence of cannabis is illegal regardless of MMJ card status. Patients should not drive after using THC-containing products until they have fully assessed their individual response at their stable dose. CBD-dominant products at moderate doses have a much lower driving-impact profile.
Parkinson’s Disease Support Resources
Parkinson’s Foundation: The leading national PD organization, maintaining the Parkinson’s Foundation Helpline (1-800-4PD-INFO, 1-800-473-4636), Centers of Excellence, and extensive patient education on cannabis and Parkinson’s at parkinson.org.
American Parkinson Disease Association (APDA): Provides evidence-based patient resources on CBD and PD, a national network of information and referral centers, and a comprehensive CBD/PD overview at apdaparkinson.org.
Michael J. Fox Foundation for Parkinson’s Research (MJFF): Actively funds cannabis and PD research and maintains current trial listings. mjff.org.
HDSA Centers of Excellence / APDA Centers: Multidisciplinary PD care teams are the appropriate setting for complex cannabis-medication discussions. Find your nearest center via Parkinson’s Foundation or APDA websites.
ClinicalTrials.gov – Parkinson’s Disease and Cannabis: Search for open studies including CAN-PDP (CBD for PD psychosis) and NCT05106504 (cannabis for non-motor PD symptoms) at clinicaltrials.gov.
Conclusion
Parkinson’s disease is one of the most complex qualifying conditions on Pennsylvania’s medical marijuana list — not because the evidence for cannabis is weak, but because the evidence is nuanced. It is strong and consistent for non-motor symptoms: sleep disorders, anxiety, depression, pain, and — in a unique and specifically supported way — PD-related psychosis through CBD.
It is promising but inconsistent for motor symptoms in controlled trials, even as patient experience data is far more positive. It points toward genuine potential for levodopa-induced dyskinesia that deserves further investigation. And it is supported by long-term real-world safety data showing no disease acceleration in PD cannabis users over 14 years of follow-up.
For Pennsylvania Parkinson’s disease patients, the PA MMJ card opens access to a complementary tool that can meaningfully address the non-motor symptom burden that standard PD medications frequently leave unmet. The key is approaching cannabis as medicine: selecting products based on your specific symptom targets, dosing conservatively, keeping your neurologist informed, and monitoring your response systematically.