
Pennsylvania’s Medical Marijuana Act includes a qualifying condition written in technical medical-legal language that leaves many patients confused about whether they actually qualify. The full statutory name is:
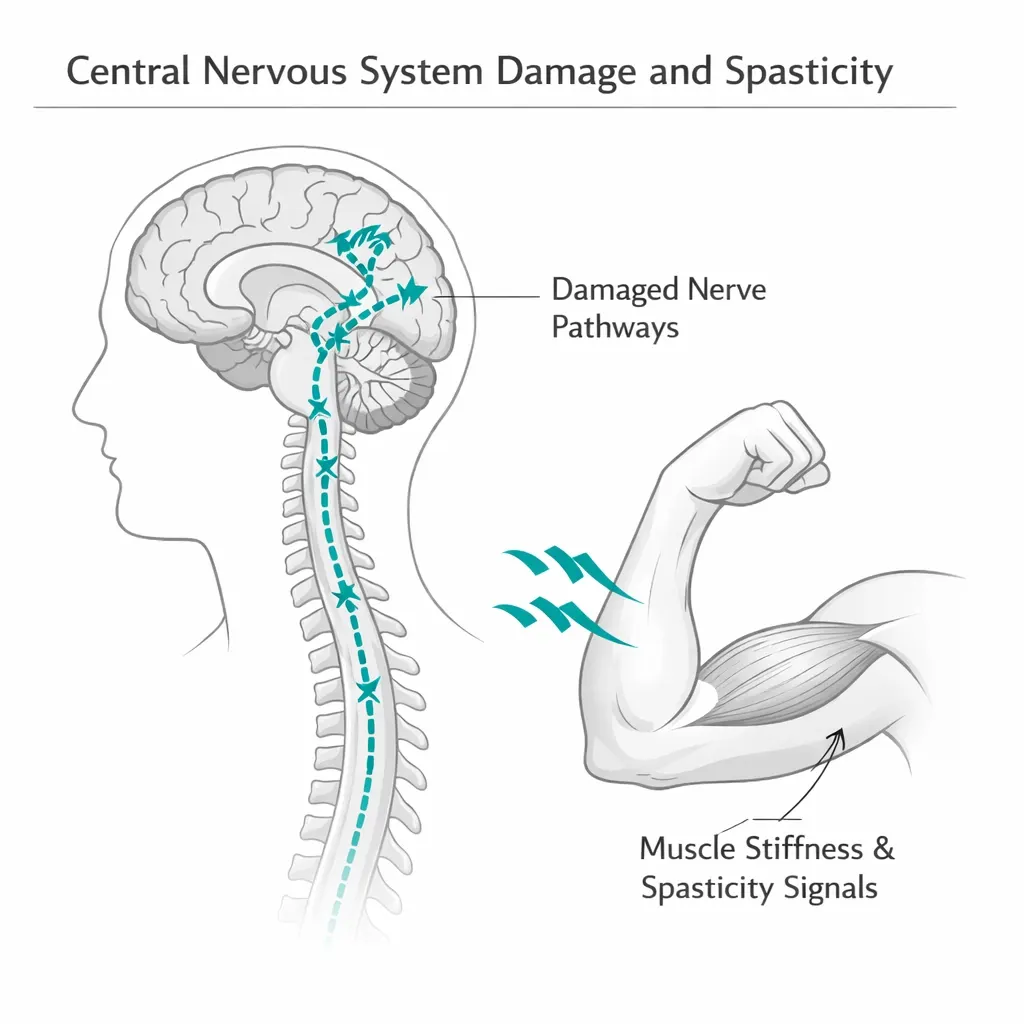
“Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies.”
This is one of the broadest and most clinically important qualifying conditions in Pennsylvania’s program — yet most patients never find it because they’re searching for their specific diagnosis, not this legal phrasing. This page decodes the language, identifies every condition that qualifies under it, explains what “objective neurological indication of intractable spasticity” means in practice, reviews the clinical evidence, and shows you how to get certified.
What This Qualifying Condition Actually Means — Decoded
The statutory language has three distinct components, each carrying specific clinical meaning.
“Damage to the nervous tissue of the central nervous system (brain-spinal cord)” — This is the underlying cause requirement. The patient must have documented damage to the brain, spinal cord, or both. Damage here means any established structural or neurological injury: traumatic injury, acquired neurological disease, congenital neurological conditions causing CNS tissue damage, or progressive disease processes that destroy CNS tissue. It does not require that the damage be recent or acute — chronic, established CNS conditions fully qualify.
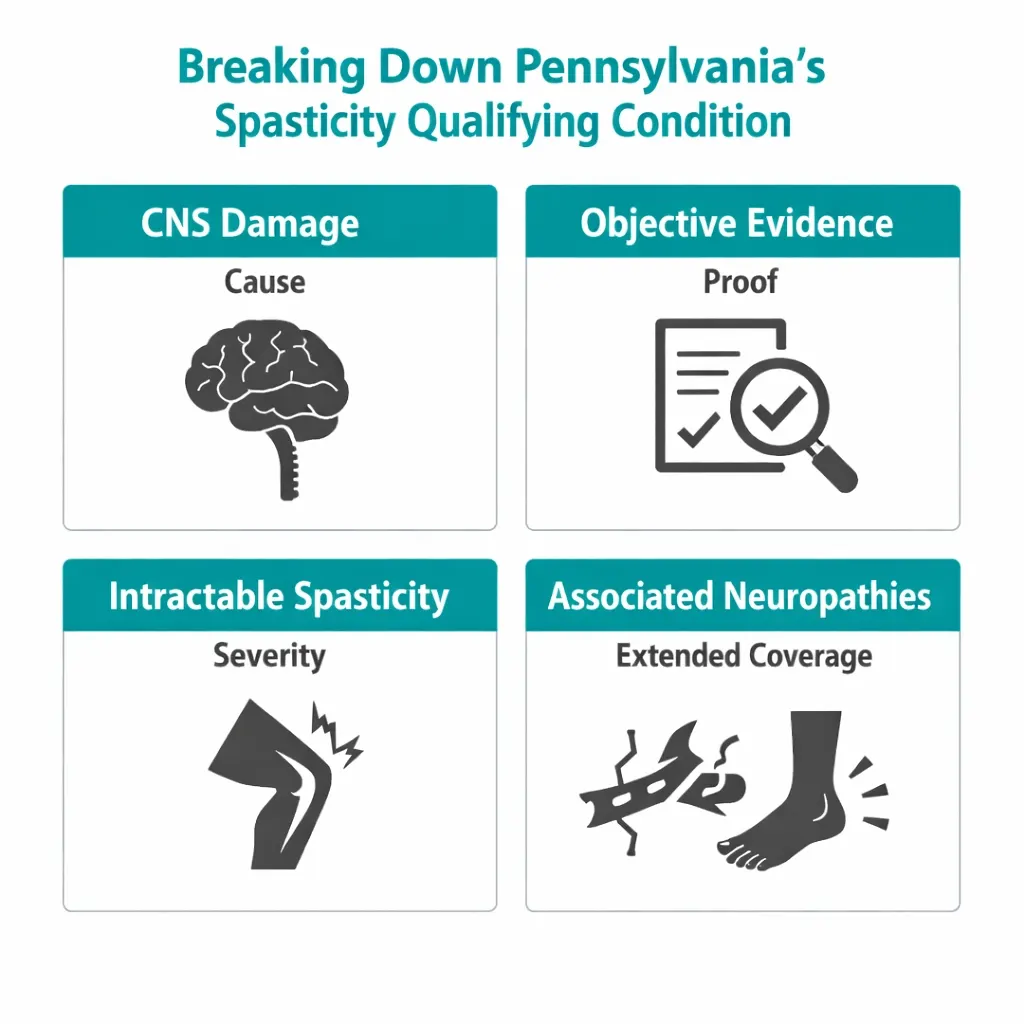
“With objective neurological indication” — This is the clinical documentation requirement. The qualifying spasticity cannot be based on patient report alone. There must be objective clinical findings — documented on physical or neurological examination, imaging, or neurophysiological testing — that confirm the presence of the upper motor neuron signs that cause spasticity. A physician’s documented clinical findings on neurological examination, MRI, EMG/nerve conduction studies, or other objective testing fulfills this requirement.
“Of intractable spasticity” — This is the severity and treatment response requirement. The spasticity must be intractable — meaning it has not been adequately controlled by standard anti-spasticity treatments. Spasticity that is fully managed by baclofen or tizanidine at well-tolerated doses is not intractable. Spasticity that persists despite adequate trials of standard medications, that cannot be controlled without unacceptable side effects, or that requires doses that cause intolerable sedation or weakness — that is intractable spasticity.
“And other associated neuropathies” — This extends the qualifying coverage beyond spasticity itself to include the neuropathic pain, sensory disruptions, and other nerve-related symptoms that accompany CNS damage. Patients with central neuropathic pain, allodynia, hyperalgesia, or other neuropathic symptoms arising from their CNS injury or disease qualify under this language even if their spasticity component alone is not the most debilitating feature.
- Source: Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Source: 28 Pa. Code Appendix A – Serious Medical Conditions
Who Qualifies — Every Condition This Language Covers
This is the section that competing pages fail to provide. The statutory language covers a wide range of specific diagnosed conditions. If you have been diagnosed with any of the following, you may qualify under this condition:
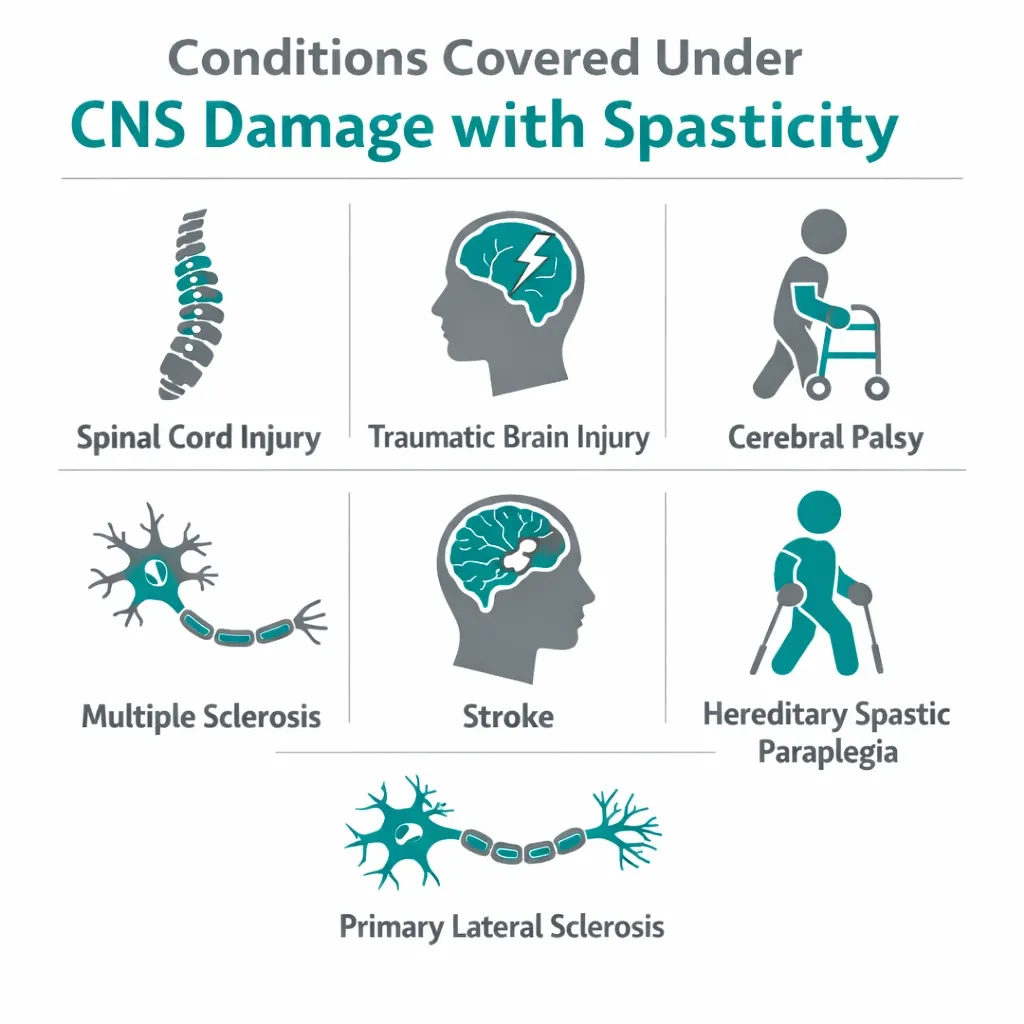
Spinal Cord Injury (SCI)
Traumatic or non-traumatic spinal cord injury producing upper motor neuron syndrome is the prototypical qualifying condition under this language. Spasticity is reported by 65–78% of individuals with SCI, with approximately 35% rating it severe enough to significantly interfere with function. Central neuropathic pain affects roughly 60% of SCI patients. Both are direct consequences of spinal cord tissue damage with objective neurological findings — exactly what this condition describes.
Traumatic Brain Injury (TBI)
TBI produces CNS tissue damage that frequently leads to upper motor neuron spasticity, spastic hemiplegia or diplegia, and central pain syndromes. Even moderate TBI can produce chronic spasticity years after injury. Documentation of TBI and subsequent spasticity on neurological examination satisfies the objective neurological indication requirement.
Cerebral Palsy (Spastic and Mixed Types)
Cerebral palsy arises from brain damage before, during, or shortly after birth. Spastic CP — which accounts for approximately 80% of all CP diagnoses — is characterized by increased muscle tone, hyperreflexia, and movement restriction caused by upper motor neuron damage. This is textbook CNS tissue damage with objective neurological indication of spasticity. Pennsylvania does not separately list cerebral palsy as a qualifying condition, but patients with spastic or mixed CP qualify under this language.
Multiple Sclerosis (MS) with Spasticity
MS is also separately listed as its own qualifying condition in Pennsylvania. However, MS patients whose most debilitating symptom is specifically spasticity may be certified under both MS and this CNS damage/spasticity condition. MS demyelination constitutes damage to CNS nervous tissue, and spasticity is its most common motor symptom, affecting 60–84% of patients. The physician can certify under whichever condition best represents the clinical picture.
Stroke with Spastic Sequelae
Post-stroke spasticity affects approximately 25–43% of stroke survivors within the first year and can persist for decades. Stroke causes focal CNS tissue damage (infarction or hemorrhage) with objective neurological signs of upper motor neuron involvement. Post-stroke spasticity with objective clinical findings qualifies under this condition.
Hereditary Spastic Paraplegia (HSP)
HSP is a group of inherited neurodegenerative conditions causing progressive lower limb spasticity due to degeneration of the corticospinal tracts. The neurological mechanism — progressive damage to upper motor neuron pathways — is directly covered by the statutory language.
Primary Lateral Sclerosis (PLS)
PLS is a rare upper motor neuron disease causing progressive spasticity without significant lower motor neuron involvement (distinguishing it from ALS). As a pure upper motor neuron disease causing CNS tissue damage and intractable spasticity, PLS falls squarely within this qualifying condition. PLS patients may also qualify under ALS if a physician documents appropriate clinical uncertainty.
Acquired Brain Injury from Other Causes
Brain injury from hypoxic-ischemic events (cardiac arrest, near-drowning), infectious encephalitis, CNS tumors and their treatment, radiation injury to the brain or spinal cord, and other causes of acquired CNS damage with resulting spasticity all qualify under this language when objective neurological findings are present.
Central Neuropathic Pain from Any of the Above
Even when spasticity itself has been partially managed, central neuropathic pain arising from SCI, TBI, MS, stroke, or other CNS damage qualifies under the “other associated neuropathies” language. Central pain syndromes — burning pain, allodynia, hyperalgesia following CNS injury — are explicitly included.
What “Objective Neurological Indication” Means in Practice
This phrase concerns many patients. It does not mean you need a recent specialized test specifically for your MMJ certification. It means there must be existing clinical documentation confirming the neurological basis of your spasticity — and for virtually every patient with diagnosed spasticity from the conditions above, this documentation already exists in their medical records.
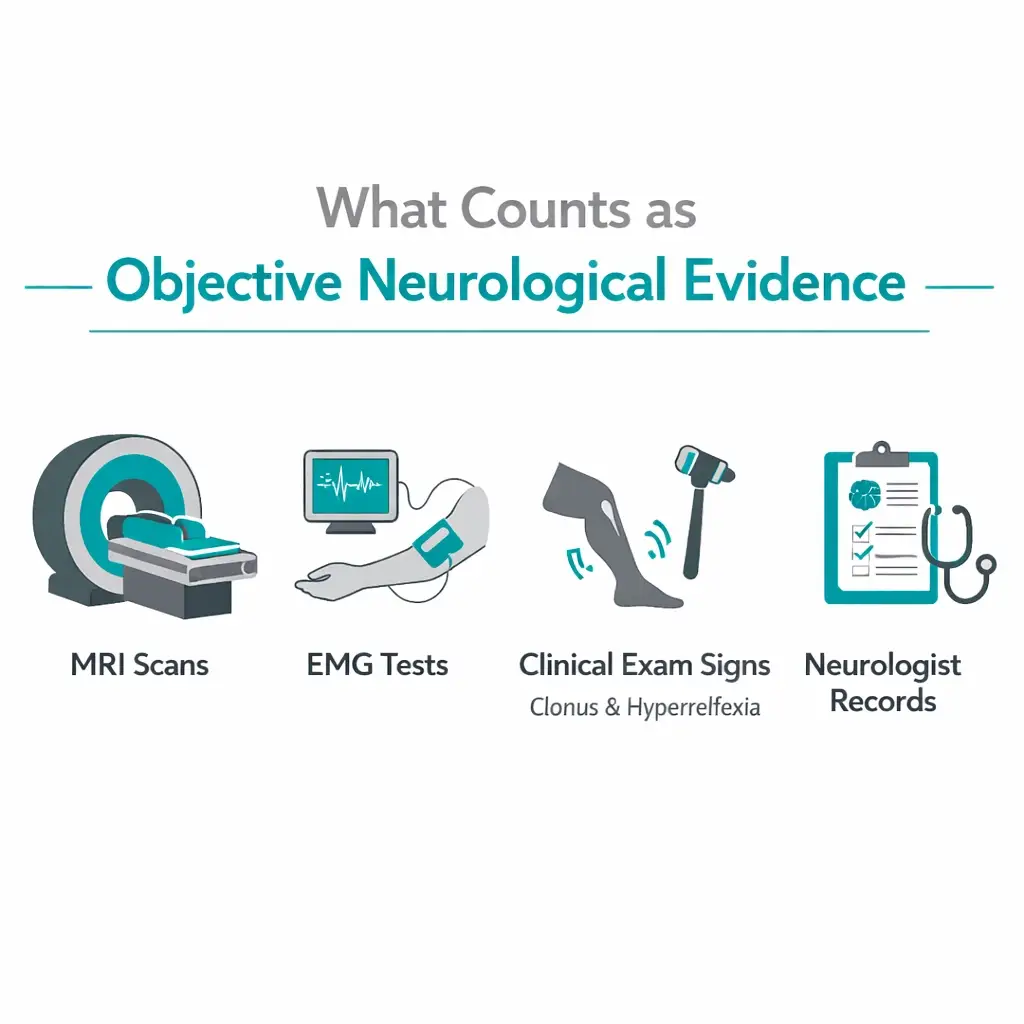
Objective evidence that satisfies this requirement includes:
- Clinical examination findings documented by any physician: hyperreflexia, clonus, Babinski sign, increased muscle tone on examination, velocity-dependent resistance to passive stretch
- MRI of the brain or spinal cord showing the structural damage underlying the spasticity (spinal cord lesions, brain injury, demyelination, etc.)
- EMG/nerve conduction studies documenting the neurological pattern consistent with upper motor neuron damage
- Prior neurological records — notes from a neurologist, physiatrist, or rehabilitation physician documenting spasticity and its neurological basis
For the vast majority of patients with established diagnoses from the conditions listed above, this documentation already exists in records from prior medical care. The certifying physician for your PA MMJ card does not generate this documentation — they review your existing documentation to confirm the objective neurological basis of your spasticity.
The Strongest Evidence Base for Cannabis and Spasticity: What the Research Shows

Spasticity from CNS damage has one of the most substantial clinical evidence bases for cannabis of any condition in Pennsylvania’s qualifying list. The evidence is anchored by nabiximols (Sativex) — a standardized 1:1 THC:CBD oromucosal spray that is approved in over 30 countries specifically for spasticity in multiple sclerosis patients who have not responded adequately to first-line antispastic medications.
While nabiximols is not FDA-approved in the United States, it represents the most rigorously studied cannabis-based medicine for spasticity worldwide and its evidence base is directly relevant to PA patients using cannabis products with comparable THC:CBD ratios.
The 2023 Meta-Analysis of Nabiximols for MS Spasticity
A 2023 systematic review and meta-analysis published in Current Neuropharmacology (Kleiner et al.) assessed all high-quality randomized, placebo-controlled trials of nabiximols for MS-associated refractory spasticity — specifically patients who had failed standard antispastic medications.
The conclusion: Nabiximols is efficient as add-on therapy for MS-associated refractory spasticity, producing statistically significant improvements in spasticity NRS scores at both short-term and long-term treatment intervals. Longer-duration treatment (6–16 weeks) showed greater effect than short-term treatment. The analysis found nabiximols significantly improved spasticity response rates compared to placebo.
The evidence quality is rated moderate — not as high as one would want, but substantially better than most cannabinoid indications. This is the strongest body of controlled evidence for any cannabinoid-based medicine in spasticity.
The 2024 Real-World German Study — Patient-Reported Benefits
A 2024 prospective, multicenter, noninterventional study published in Neurodegenerative Disease Management (Haupts et al.) followed 51 adult MS patients with spasticity unresponsive to conventional medications through 12 weeks of nabiximols treatment.
Mean Goal Attainment Scale scores increased by 46% from baseline to week 12 (p < 0.001). After 12 weeks, 65% of patients considered their spasticity “much improved.” Common treatment goals — less pain, better walking, improved sleep — were achieved “as expected or better” in 62% of cases. Few side effects were reported.
Evidence for SCI-Related Spasticity and Neuropathic Pain
Evidence for cannabis in spinal cord injury-specific spasticity and pain is smaller in volume than the MS literature, but consistently directional. A 2023 survey study published in Frontiers in Pain Research (Kinnunen et al.) assessed self-reported cannabis effects on neuropathic pain and medication use in SCI patients. Of SCI patients using cannabis, the majority reported positive effects on pain and spasticity. Notably, 96.1% of SCI patients reported using cannabis after their injury — a much higher proportion than before — indicating the scale of unmet need driving self-medication in this population.
A 2023 multicenter Danish randomized trial published in Pharmaceuticals (Hansen et al.) studied THC, CBD, THC+CBD, and placebo in MS and SCI patients with neuropathic pain and spasticity. The trial found numerically better effects with active treatment arms compared to placebo, but did not reach statistical significance, likely due to insufficient sample size from COVID-related enrollment challenges. The authors could not exclude a clinically meaningful effect.
- Source: Frontiers in Pain Research – Self-Reported Cannabis Effects on SCI Neuropathic Pain (Kinnunen et al., 2023)
- Source: PMC – Cannabis-Based Medicine for NP and Spasticity in MS and SCI: RCT (Hansen et al., 2023)
Stroke-Related Spasticity
A 2022 double-blind, randomized, placebo-controlled study (Frontiers in Neurology, Marinelli et al.) studied cannabinoid effects specifically in spasticity following stroke. Compared to baseline, nabiximols produced significantly greater mean reductions in spasticity scores (Modified Ashworth Scale) than placebo, and significantly favored nabiximols on pain as a secondary outcome. This is the most direct evidence for cannabis in post-stroke spasticity specifically.
Cerebral Palsy — Honest Assessment of a Mixed Evidence Picture
For cerebral palsy specifically, the evidence is more cautious. A 2020 randomized controlled trial (Fairhurst et al., Developmental Medicine & Child Neurology) tested nabiximols versus placebo for spasticity in 72 children with cerebral palsy or traumatic CNS injury. The trial found no significant difference between nabiximols and placebo on the primary or secondary spasticity outcomes. Three cases of hallucinations were observed in the nabiximols group, one involving a suicide attempt.
This null result matters and should be stated clearly: nabiximols did not show benefit over placebo for pediatric spasticity in cerebral palsy in the most rigorous RCT conducted. For adult patients with CP-related spasticity, the adult MS evidence is reasonably analogous mechanistically — the neurological basis of spasticity is similar — but a direct adult CP RCT of nabiximols has not been conducted. For pediatric patients with CP considering cannabis for spasticity, the current evidence does not support it, and the hallucination risk in the Fairhurst trial is a safety signal that warrants serious caution.
A 2024 double-blind, placebo-controlled Slovenian trial of CBD:THC oil (10:1 ratio) for spasticity in children with severe CP enrolled 53 patients. This is an important emerging trial — results are being processed and further publication is expected.
- Source: PubMed – Nabiximols for Paediatric Spasticity in Cerebral Palsy or TBI: RCT (Fairhurst et al., 2020)
- Source: ScienceDirect – Full-Spectrum Cannabis Oil for Spasticity in Children with CP: Double-Blind RCT (2024)
The American Academy of Neurology Position
The AAN’s 2014 guideline on complementary and alternative medicine in MS (updated since) found that oral cannabis extract was “probably effective” for spasticity and pain in MS — the second-highest certainty level in their rating system. For patients with spasticity from other CNS causes where direct evidence is more limited, the AAN recommends individual clinical judgment informed by the MS evidence base.
Symptom by Symptom: Where Cannabis Helps Most in CNS Spasticity
Spasticity Itself — Patient-Reported vs. Objective Measures
A consistent and clinically important distinction runs through the spasticity literature: cannabis reliably reduces patient-reported spasticity severity but produces smaller effects on objective spasticity measures (Modified Ashworth Scale, pendulum test). This gap between subjective and objective measurement appears in almost every spasticity RCT.
For patients, this distinction matters less than it sounds. Patient-reported spasticity — how much it hurts, how much it limits movement, how much it disrupts sleep — is a legitimate and clinically important outcome in its own right. If a patient with SCI reports meaningful reduction in spasticity-related discomfort and improved function, that is a real benefit even if a clinician’s measurement tool shows modest change. The goal of symptom management is patient wellbeing, not a specific number on the Ashworth scale.
Central Neuropathic Pain
Neuropathic pain from CNS damage is among the most treatment-resistant pain types in medicine. Gabapentin and pregabalin are first-line treatments — and fail or are poorly tolerated by a substantial proportion of patients. Cannabis has shown meaningful benefit for central neuropathic pain specifically. The AAN guideline found cannabinoids “probably effective” for central pain in MS. Multiple RCTs of nabiximols in MS have shown pain as a significant secondary outcome. For SCI-related central pain, direct evidence is limited but patient-reported benefit is consistently high in survey data.
The “associated neuropathies” language in Pennsylvania’s qualifying condition is specifically designed to capture this: patients whose CNS damage produces neuropathic pain as a primary burden qualify even when spasticity itself is not the dominant complaint.
Spasm Frequency and Sleep Disruption
Painful muscle spasms — particularly nocturnal spasms that repeatedly interrupt sleep — are among the most quality-of-life-disrupting features of CNS spasticity syndromes. Multiple nabiximols trials have shown reductions in spasm frequency as a meaningful secondary outcome. Sleep disturbance improvement is consistently reported across the nabiximols real-world literature. A 2024 nabiximols case series published in Drugs in Context found meaningful improvements in spasticity-related sleep disturbance, bladder dysfunction, and pain as interconnected symptom clusters.
Bladder Dysfunction
Neurogenic bladder — overactive bladder, urinary urgency, and incontinence from CNS damage — affects a large proportion of patients with SCI, MS, and TBI. Nabiximols has shown modest but statistically significant reductions in bladder urgency episodes in some MS trials. This is a particularly meaningful outcome for patients whose daily function is most limited by bladder symptoms.
Anxiety and Mood
Living with the chronic physical consequences of CNS damage — limited mobility, pain, spasms, dependence on others — produces significant psychological burden. Anxiety and depression are prevalent in SCI, TBI, MS, and stroke populations. CBD-dominant formulations in particular show benefit for anxiety that compounds the benefit for spasticity management by addressing the psychological dimension of the symptom burden.
Drug Interactions for Patients with CNS Damage
Patients with spinal cord injury, TBI, stroke, and CP typically carry complex medication regimens. The most important interaction considerations:
Baclofen and tizanidine (antispastic drugs): Additive muscle relaxation and CNS depression with cannabis. Monitor for increased sedation and weakness. Tizanidine is metabolized by CYP1A2; CBD may inhibit this enzyme, potentially increasing tizanidine plasma levels and risk of hypotension.
Gabapentin and pregabalin (neuropathic pain): Additive CNS depression. Increased sedation is the primary concern. Driving and operating machinery should be discussed when combining these medications with cannabis.
Opioids (spasticity-related pain): CBD inhibits CYP3A4 and CYP2D6, which metabolize most opioids. Increased opioid plasma levels are possible. Monitor for increased sedation and respiratory depression. The opioid-sparing effect — meaning cannabis may allow lower opioid doses with equivalent or improved pain control — is a clinically meaningful potential benefit.
Benzodiazepines (spasm management, anxiety): Additive CNS depression. Particularly significant for patients with respiratory compromise (as in high-level SCI). Use with caution.
Antiepileptic drugs: Epilepsy is common after TBI and stroke. CBD inhibits CYP2C9, CYP3A4, and other enzymes metabolizing several AEDs. Clobazam and valproate interactions are particularly well-documented. Disclose all AEDs to the certifying physician.
Anticoagulants (warfarin, newer anticoagulants): Common in stroke survivors for secondary prevention. CBD inhibits CYP2C9 — warfarin is a CYP2C9 substrate. INR monitoring is important if adding cannabis.
Always bring a complete, current medication list to the certifying physician evaluation. These are conversation-starters, not hard contraindications.
Practical Guidance: What Products Work Best for This Condition
Pennsylvania’s approved forms include oils and tinctures, capsules and pills, vaporizable dry leaf (vaporizer only), liquid solutions/metered-dose inhalers, patches, and topicals. Smoking is not permitted.
For spasticity and spasm: Balanced THC:CBD formulations (1:1 or close) most closely replicate the nabiximols evidence base. Oral tinctures provide longer duration suitable for sustained spasticity management. Vaporized forms provide faster onset useful for acute spasm episodes in patients with adequate respiratory function.
For central neuropathic pain: THC-containing formulations are generally more effective for central pain than CBD alone. Balanced products or mild THC-dominant formulations, taken on a scheduled basis rather than as needed, provide more consistent pain coverage.
For sleep disruption from spasms: Low-to-moderate THC products in the evening have the most evidence for sleep-onset improvement. Avoid high THC doses which can fragment sleep architecture.
For patients with cognitive concerns after TBI: Start with CBD-dominant products at the lowest effective dose. THC at higher doses can worsen cognitive function and increase confusion — a meaningful safety concern for patients with prior TBI-related cognitive impairment. Begin with THC doses as low as 1–2.5 mg and titrate slowly.
For pediatric patients (CP, congenital CNS injury): Pediatric use requires a caregiver registration, and the certifying physician must be comfortable with pediatric patients. Based on current evidence, the risk-benefit is less clear in children than adults — particularly the hallucination risk observed in the Fairhurst trial. If pursuing cannabis for a child with CP, start with CBD-dominant products and involve the child’s neurologist.
Dermal patches and topicals offer an option for patients with limited dexterity or motor control, as caregivers can apply them without requiring patient action.
How to Get Your Pennsylvania MMJ Card for This Condition

Step 1 — Physician Certification (Telehealth)
Schedule a telehealth appointment with a PA DOH-registered medical marijuana physician. Evaluations take approximately 10–15 minutes. The certifying physician does not need to be your neurologist or physiatrist — any PA-registered MMJ physician who has a continuing care relationship with you and can review your existing neurological documentation can certify you.
What to bring to the appointment:
- Any prior neurological records: MRI reports, EMG results, neurologist notes
- Documentation of your underlying diagnosis (SCI, TBI, CP, stroke, MS, etc.)
- Documentation of prior spasticity treatment and its results — what medications you have tried, at what doses, and why they were inadequate (failed to control spasticity, unacceptable side effects, etc.)
- Your full current medication list
The physician needs to confirm the objective neurological basis of your spasticity and that it has been intractable to prior treatment. For established diagnoses with existing neurological records, this is typically straightforward.
Step 2 — State Registration
After certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com) with your certification, a valid PA driver’s license or state-issued ID, and the $50 annual fee. Fee waivers apply for Medicaid, PACE/PACENET, CHIP, SNAP, and WIC enrollees.
Step 3 — Caregiver Registration (Particularly Relevant Here)
For patients with significant motor impairment — SCI with limited hand function, severe CP, TBI with cognitive impairment — the PA caregiver pathway is particularly important. Up to two designated caregivers can register to make dispensary purchases and assist with product administration on the patient’s behalf. Caregivers must be 21+, pass a background check, and pay the $25 fee.
Step 4 — Visit a Licensed PA Dispensary
Tell the dispensary pharmacist specifically about your underlying diagnosis, your symptom priorities (spasticity, pain, sleep, spasm), and your current antispastic medications. This allows them to recommend formulations that balance effectiveness with the interaction considerations for your specific medication regimen.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Anxiety Disorder
- Terminal illness
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: I have cerebral palsy but my spasticity is managed by Botox injections — do I still qualify?
Q: I had a stroke two years ago and have spastic hemiplegia. I’m on baclofen but it doesn’t fully control my spasms. Do I qualify?
Q: My spinal cord injury is complete at T10. My spasticity is severe below the level of injury. Does “objective neurological indication” require I have feeling in those areas?
Q: I have MS and I’m already certified for MS as my qualifying condition. Can I also use this condition?
Q: I have TBI-related cognitive impairment in addition to spasticity. Are there extra risks of cannabis I should know about?
Support Resources
Christopher & Dana Reeve Foundation (christopherreeve.org) provides resources for spinal cord injury patients and families, including information on emerging therapies and quality-of-life resources. Their helpline is 800-539-7309.
United Cerebral Palsy (UCP) (ucp.org) provides state-by-state resource locators and advocacy for individuals with cerebral palsy and other CNS conditions.
National Multiple Sclerosis Society (nationalmssociety.org) provides comprehensive resources on MS management including cannabis at their dedicated cannabis page.
Brain Injury Association of America (biausa.org) provides resources for TBI survivors and families, including guidance on complementary approaches to symptom management.
American Stroke Association (stroke.org) provides stroke survivor resources including guidance on long-term symptom management.
NOTE: Pennsylvania’s “CNS damage with intractable spasticity” condition is written in technical language, but its coverage is broad: spinal cord injury, traumatic brain injury, stroke, cerebral palsy, primary lateral sclerosis, hereditary spastic paraplegia, and the spasticity and neuropathic pain of MS — all fall within its scope. The evidence base for cannabis in spasticity from central nervous system damage, while stronger for MS than for other conditions, is the most robust of any area of neurological cannabis research, anchored by nabiximols regulatory approvals in more than 30 countries.
If your spasticity has not been adequately controlled by baclofen, tizanidine, or other standard treatments, the evidence supports a trial of cannabis as adjunctive therapy — and Pennsylvania’s program gives you legal access to pursue it.