
MS does not announce itself politely. It arrives sometimes gradually, sometimes all at once and starts changing the rules of your own body. The muscle that locks up at 2am. The burning pain that runs down your leg for no apparent reason. The bladder urgency that makes you mentally map every bathroom before you leave the house. The fatigue that is so much deeper than tired that people who have not felt it truly cannot understand it.
You have probably already tried the medications. Some have helped with the disease itself. Others have helped some symptoms some of the time. And yet you are still here, still managing, still looking for anything that might take some of the daily burden away.
Pennsylvania listed multiple sclerosis as a qualifying condition in its Medical Marijuana Act from the very beginning. If you have MS, you have a legal path to a PA MMJ card and this page explains everything you need to know to use it well.
Does Multiple Sclerosis Qualify for a PA MMJ Card?
Yes – and it has since the program launched. Multiple sclerosis is one of the original qualifying conditions listed in the Pennsylvania Medical Marijuana Act (Act 16 of 2016), recognised by the Pennsylvania Department of Health.
Pennsylvania also separately lists damage to the nervous tissue of the central nervous system with objective neurological indication of intractable spasticity, which covers many MS patients who experience severe, treatment-resistant spasticity even if they want to certify under a more specific description. In practice, MS alone is more than sufficient for certification.
There is no severity requirement. Any confirmed MS diagnosis, relapsing-remitting (RRMS), secondary progressive (SPMS), or primary progressive (PPMS), qualifies. You do not need to have failed any specific medications, though your treatment history will naturally come up in your telehealth appointment.
Sources:
- Pennsylvania Department of Health – Medical Marijuana Qualifying Conditions
- 28 Pa. Code Appendix A – Serious Medical Conditions
What MS Actually Does to Your Body — And Why Cannabis Makes Sense
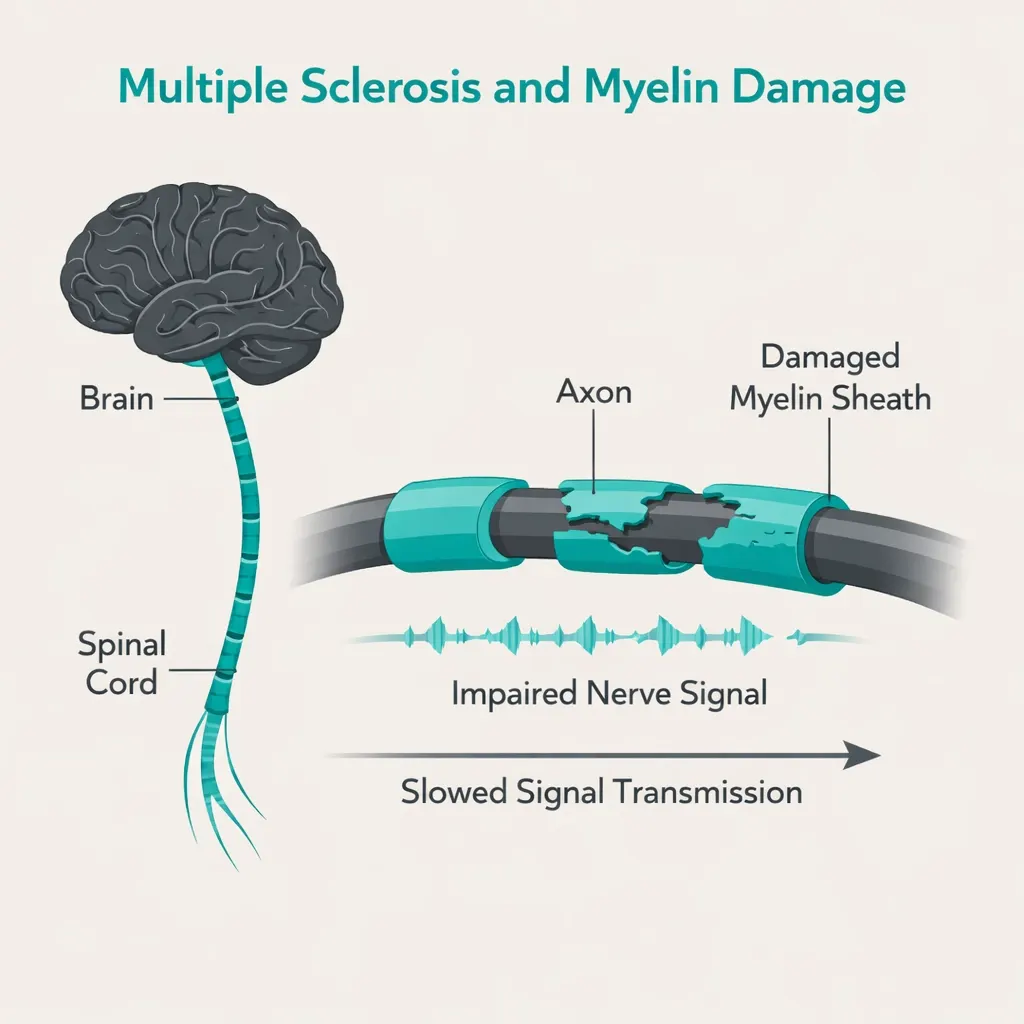
Multiple sclerosis is an autoimmune disease where the immune system attacks myelin, the protective sheath around nerve fibres in the brain and spinal cord. When myelin is damaged, nerve signals slow down, get disrupted, or stop entirely. The result is a wide range of symptoms depending on which nerves are affected.
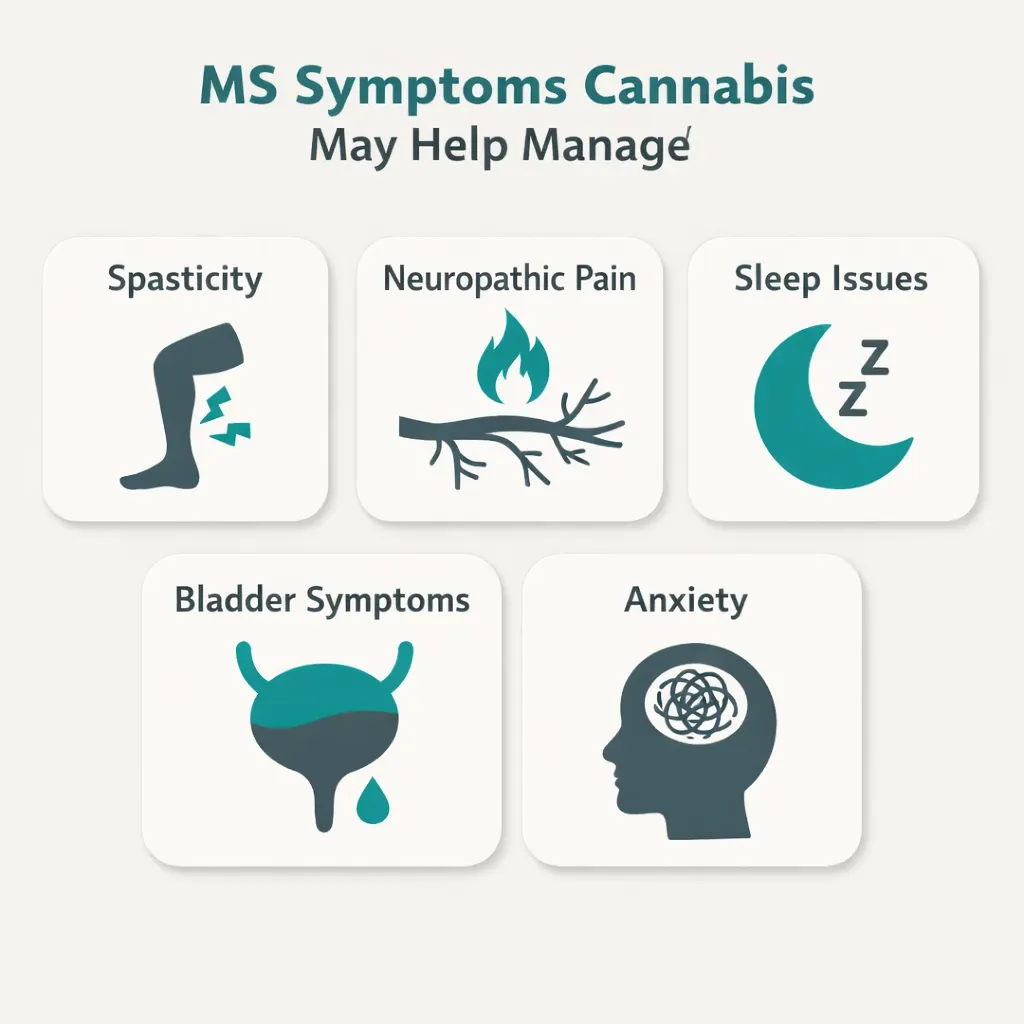
For most people, MS is not a single overwhelming disability. It is a collection of unpredictable daily burdens: the spasticity that tightens your legs at night, the neuropathic pain that feels like burning or electric shocks, the bladder urgency that dominates every outing, the fatigue that is not fixed by sleep, the anxiety that comes from not knowing what tomorrow will look like.
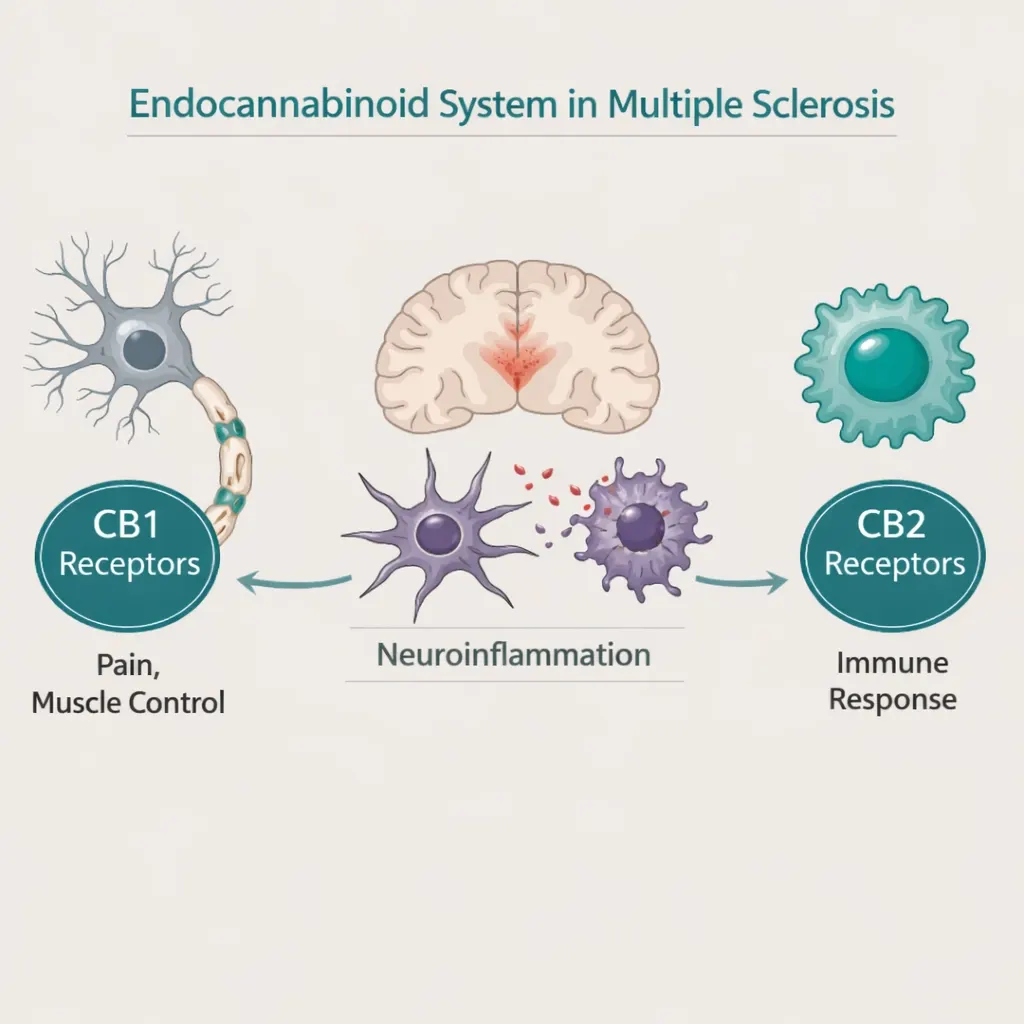
The endocannabinoid system is densely present throughout the central nervous system, exactly where MS does its damage. CB1 receptors regulate pain signalling, muscle tone, and bladder function. CB2 receptors modulate the immune response and inflammation. This is not coincidence. It is why MS is one of the conditions with the longest and strongest evidence base for cannabis in the entire medical marijuana field.
In fact, pharmaceutical cannabidiol for spasticity in MS is the only complementary medicine intervention with high-level evidence for efficacy in MS according to recent clinical reviews. Cannabis did not squeeze its way into MS treatment, the evidence pulled it there.
What the Research Shows
Spasticity — The Strongest Evidence
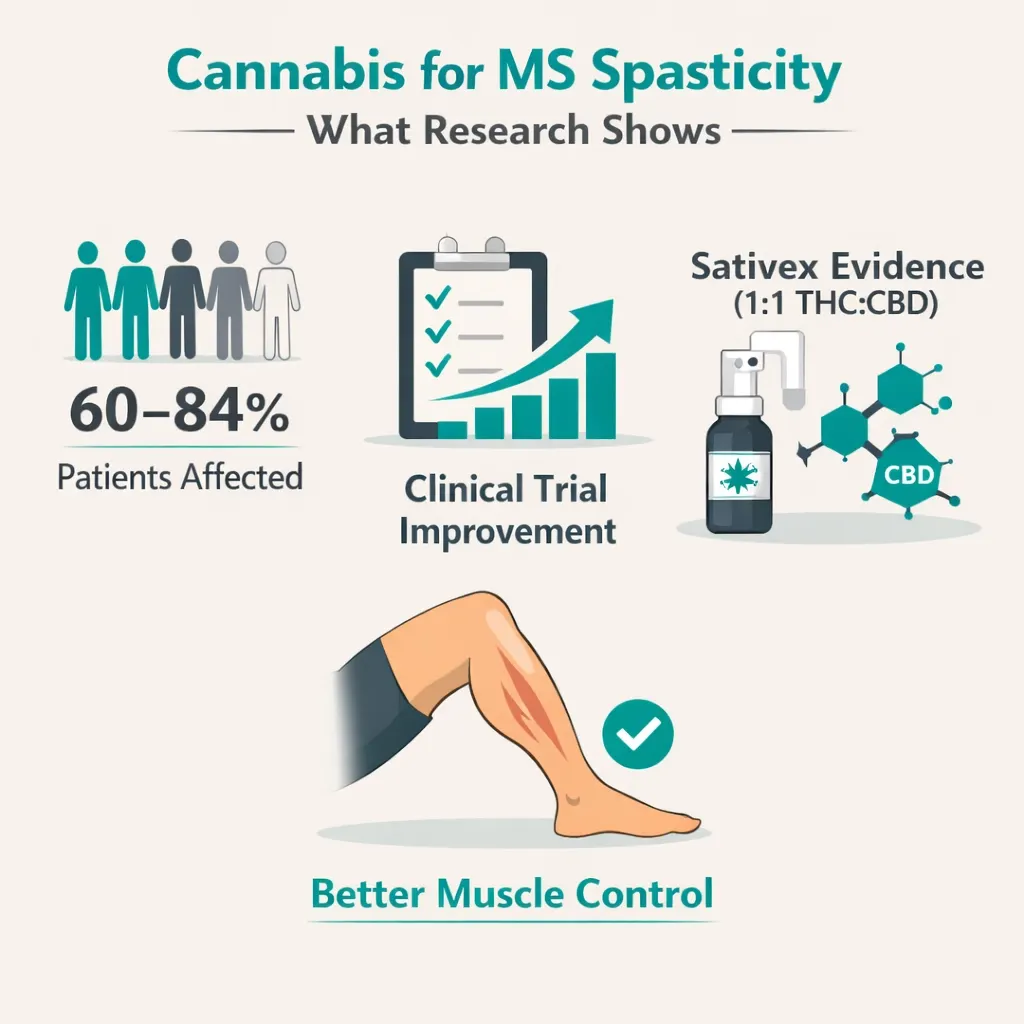
Spasticity is the MS symptom with the most consistent and robust cannabis evidence. Between 60–84% of MS patients experience spasticity at some point, the muscle stiffness, involuntary spasms, and painful contractions that can disrupt sleep, limit movement, and make every physical task harder.
A 2025 systematic review and meta-analysis published in Clinical Therapeutics analysed nine clinical trials involving 2,544 MS patients. The overall result showed clinically meaningful improvement in spasticity scores across the combined data. The conclusion: cannabis-based therapies are associated with clinically meaningful improvements in MS-related spasticity, particularly over longer treatment durations.
The MS Extract of Cannabis (MUSEC) trial found a twofold increased rate of relief from muscle stiffness with oral cannabis extract containing THC after 12 weeks, along with improved spasticity relief, physical and psychological impact, and walking ability compared to placebo.
Nabiximols (Sativex) — a 1:1 THC:CBD oromucosal spray approved for MS spasticity in Canada and most of Europe is the most studied cannabinoid product for MS. A Cochrane review concluded it has moderate certainty evidence for spasticity improvement, most effective in patients with moderate to severe spasticity that has not responded well to other treatments. Sativex is not currently FDA-approved in the United States, which is exactly why a PA MMJ card matters, it gives Pennsylvania patients access to the closest dispensary equivalent.
Sources:
- Clinical Therapeutics – Assessing the Role of Cannabis in Managing Spasticity in MS: Systematic Review and Meta-Analysis (2025)
- ASRA Pain Medicine – Cannabis in the Management of MS-Related Pain and Spasticity (2024)
Pain — Meaningful Relief for Most Patients
Over 60% of people with MS will experience MS-related pain during the course of their disease. This includes central neuropathic pain (the burning, pins-and-needles, electric shock sensations that come from nerve damage), musculoskeletal pain, and pain from spasms.
A retrospective review of 141 MS patients using medical cannabis, published in the International Journal of MS Care in 2023, found that 72% of patients experienced pain alleviation after starting medical cannabis. This is real-world data from a neurology clinic, not a controlled trial, but the numbers are striking.
Both the American Academy of Neurology (AAN) and the National Academies of Sciences, Engineering, and Medicine (NASEM) reviews found that cannabis-based products helped with MS pain, across different pain types including central neuropathic pain and pain from spasms, when assessed both by patient report and objective clinical measures.
Sleep — Consistently Improved
MS disrupts sleep in multiple ways, pain keeping you awake, spasms waking you at night, bladder urgency pulling you up repeatedly, anxiety making it hard to settle. The 2023 retrospective review found sleep improvement in 40% of MS patients after starting medical cannabis. Multiple UK clinical trials (CAMS and MUSEC) showed that people with MS taking oral cannabis reported better sleep than those taking placebo. The NASEM review concluded cannabis-based products could improve sleep in MS.
For patients whose nights have been dominated by pain and spasms, this is one of the most practically meaningful benefits.
Bladder Symptoms — Promising Signal
MS lesions can disrupt the signalling between the brain and the bladder, causing urgency, frequency, and incontinence that severely limits daily life. The evidence for cannabis and bladder symptoms in MS shows that overactive bladder symptoms were significantly reduced with THC/CBD oromucosal treatment (p=0.001) in a pilot trial of MS patients with treatment-resistant overactive bladder. The AAN review suggested oral cannabis products can reduce urinary frequency, though the evidence is less consistent for incontinence specifically.
Opioid Reduction — An Underappreciated Benefit
The 2023 retrospective review found a significant reduction in concomitant opioid use after MS patients started medical cannabis, measured as a significant decrease in daily morphine milligram equivalents among patients who had been prescribed opioid analgesics. For MS patients managing severe neuropathic pain with opioids and their own side effects, this opioid-sparing potential is a genuine quality-of-life benefit.
What Cannabis Does Not Help with in MS
Honesty matters here. The evidence for cannabis reducing MS tremors is weak, studies have not found any clear benefit for tremor control, and you should not expect a PA dispensary product to address that symptom meaningfully. The evidence for cannabis affecting MS fatigue directly is also not robust. Cannabis is not a disease-modifying therapy, it does not slow the progression of MS or repair myelin. It is a symptom management tool, and for the symptoms where evidence is strongest, spasticity, pain, sleep, bladder, it is a genuinely useful one.
PA Dispensary Product Guidance for MS
For Spasticity and Muscle Spasms
A balanced THC:CBD tincture or oil (1:1 ratio) is the closest dispensary equivalent to Sativex, the pharmaceutical product with the most MS-specific clinical evidence. This combination appears to work better for spasticity than either compound alone. Sublingual tinctures have faster onset, 15–45 minutes, making them useful for acute spasm episodes.
For nighttime spasticity that disrupts sleep, a moderate THC dose (5–10 mg THC equivalent) taken an hour before bed via a balanced oil is commonly effective.
For Neuropathic Pain
Balanced or mild THC-dominant products are more effective for neuropathic pain than CBD alone. CBD alone does not have strong evidence for neuropathic pain relief in MS. Start low with THC 2.5–5 mg and increase slowly. Taking oil products with a small amount of fat significantly improves absorption.
For Sleep
Moderate THC doses taken 60–90 minutes before bed via oral capsule or tincture consistently help with sleep in MS patients. The slower release from capsules can be beneficial for staying asleep through the night rather than just falling asleep.
For Anxiety and Mood
CBD-dominant products at meaningful doses (20–40 mg CBD) are appropriate for anxiety management without significant psychoactive effect. CBD also has preliminary evidence for anti-inflammatory activity relevant to MS, though the clinical significance of this in humans is still being studied.
For Bladder Symptoms
THC/CBD balanced products may help with overactive bladder urgency. This is best managed with consistent daily low-dose oral use rather than acute dosing. Results vary more than with spasticity and pain.
Important Caution: Cognitive Effects
MS can already affect cognition and memory. THC, particularly at higher doses, can further affect short-term memory, concentration, and processing speed. Start with the lowest effective dose. If you notice worsening cognitive fog after starting cannabis, reduce the dose or switch to a higher CBD:THC ratio. Monitor this honestly and mention it to your neurologist.
Drug Interactions: MS Medications and Cannabis
Most MS patients are on disease-modifying therapies (DMTs), the medications that slow MS progression. The good news for most PA patients is that the interaction profile is relatively reassuring.
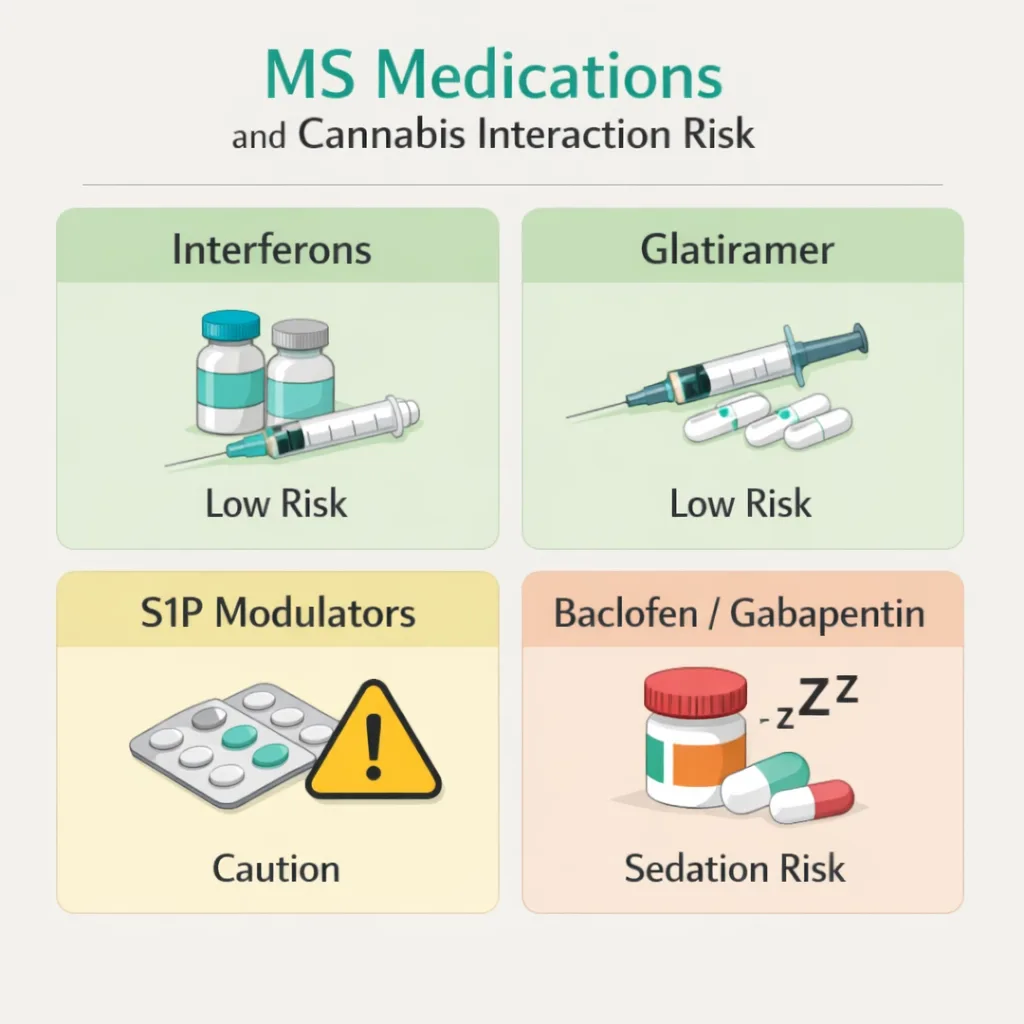
Interferons (Avonex, Betaseron, Rebif), glatiramer acetate (Copaxone), and natalizumab (Tysabri) are not significantly metabolised through CYP450 enzymes in ways that cannabis affects. The direct pharmacokinetic interaction risk with these agents is low. Continue your DMT exactly as prescribed, cannabis does not replace disease-modifying therapy under any circumstances.
Fingolimod (Gilenya), siponimod (Mayzent), and ozanimod (Zeposia) are oral sphingosine-1-phosphate modulators. These are metabolised through CYP pathways that cannabinoids can affect. The interactions are not well-characterised, but it is worth mentioning cannabis use to your neurologist if you are on one of these agents.
Baclofen and tizanidine are muscle relaxants commonly prescribed for MS spasticity. Both cause sedation. Cannabis, particularly at higher THC doses, also causes sedation. Combined, the sedative effects can be additive, meaning you may feel more drowsy than either alone would cause. Start cannabis at a low dose if you are already on a muscle relaxant, and do not take high THC doses until you know how the combination affects you.
Gabapentin and pregabalin are used for neuropathic pain in MS. These also have sedative potential. The same additive sedation caution applies.
The overall message: tell your neurologist you are using cannabis. Cannabis does not threaten your DMT but managing additive sedation from muscle relaxants and pain medications is a genuine practical consideration.
How to Get Your PA MMJ Card for Multiple Sclerosis
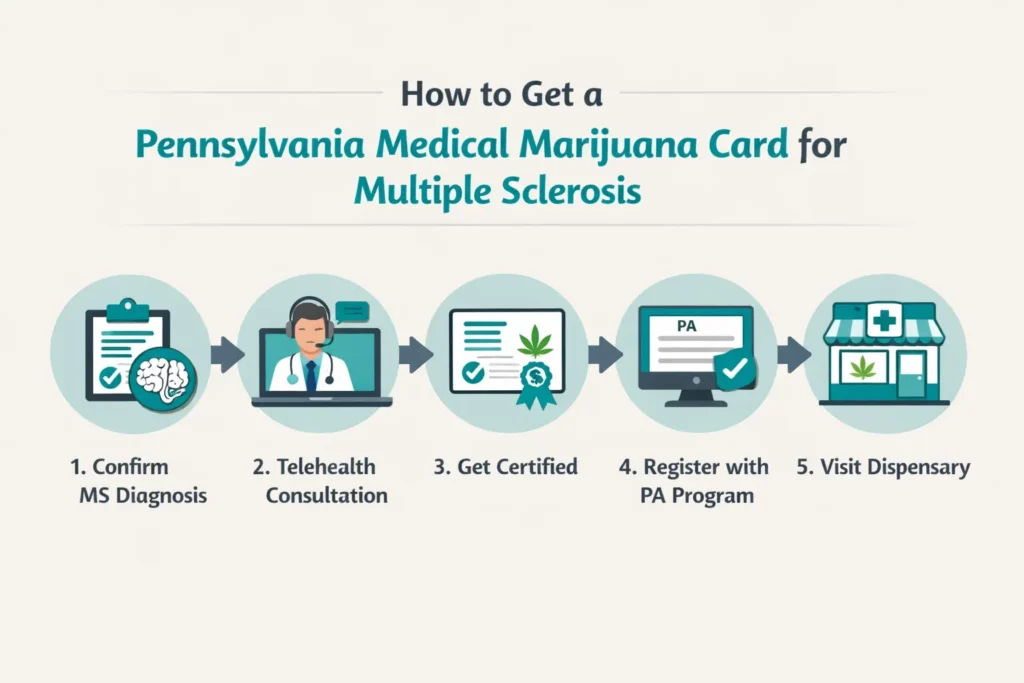
Step 1 — Gather your MS diagnosis records
Your diagnosis documentation from a neurologist is all you need. Bring any recent clinical notes and your current medication list, especially your DMT and any symptomatic medications like baclofen or gabapentin.
Step 2 — Tell your neurologist
Your neurologist needs to know you are using cannabis, particularly because of the additive sedation risk with baclofen or gabapentin, and because cannabis can affect cognition in ways your neurologist should be monitoring. Most MS neurologists are familiar with the evidence and will not be surprised by the conversation.
Step 3 — Book a telehealth certification appointment
Find a PA DOH-registered medical marijuana certifying physician and book a telehealth appointment from home. The appointment takes 10–15 minutes. The certifying physician submits your certification directly to the Pennsylvania Department of Health.
Step 4 — Register with the PA MMJ Program
Go to the PA Medical Marijuana Program Patient Registry at patientportal.mmapinc.com. You need your PA driver’s licence or state-issued ID and the $50 annual fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 5 — Visit a Pennsylvania dispensary
Tell the dispensary pharmacist you have MS and describe your primary symptoms, spasticity, pain, sleep, bladder, or anxiety. Ask for balanced THC:CBD products as a starting point. Start at the lowest available dose and increase slowly over weeks.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Anxiety Disorder
- Chronic Hepatitis C
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: I have RRMS and my disease is well-controlled on my DMT. Can I still get a PA MMJ card for symptom management?
Q: Will cannabis replace my disease-modifying therapy?
Q: I take baclofen for spasticity. Should I stop it when I start cannabis?
Q: My MS fatigue is severe. Will cannabis help?
Q: Is there a risk cannabis will worsen my MS cognition?
Pennsylvania MS Support Resources
National MS Society – Pennsylvania Chapters
- Greater Delaware Valley Chapter (Philadelphia area): nationalmssociety.org
- Keystone Chapter (Pittsburgh and western PA): nationalmssociety.org
Both chapters offer support groups, local programmes, and resources on MS treatment options including medical cannabis. If you have questions about your specific MS situation, these are the organisations most equipped to connect you with Pennsylvania-specific support.
MS Society UK – Cannabis and MS Research Summary mssociety.org.uk/cannabis-and-ms An honest, evidence-based summary of what the research does and does not support, useful reading before your first dispensary visit.
Multiple Sclerosis News Today – Cannabis and MS multiplesclerosisnewstoday.com/cannabis-and-ms Regularly updated patient-facing coverage of new MS and cannabis research.
Note: MS is a long road. The disease-modifying therapies are doing important work in the background, protecting your nervous system, slowing what they can slow. But they do not reach the daily symptom burden that makes ordinary life hard. That is where a PA MMJ card, used thoughtfully and alongside your existing treatment, can genuinely help.
The evidence for cannabis in MS is among the strongest for any qualifying condition on Pennsylvania’s list. Spasticity, pain, sleep, bladder, real symptoms, real evidence, real relief for many patients. You deserve access to every tool that might make tomorrow slightly more liveable than today.