
If you are reading this page, there is a good chance you are exhausted.
Maybe you are the parent who has sat on the floor next to your child during a seizure, counting the seconds, wondering if this is the one that doesn’t stop. Maybe you are the adult who has quietly stopped driving, stopped swimming, stopped doing the things that everyone else takes for granted because you never know when the next one is coming. Maybe you have tried drug after drug after drug, sat through appointment after appointment, watched doses go up and side effects pile on, and still the seizures keep coming.
“Intractable” is a clinical word. But for the people living with it, it means something far more personal than a medical definition. It means that the standard answers haven’t been enough. It means you are still looking.
Pennsylvania heard you. Intractable seizures is an explicitly named qualifying condition under Pennsylvania’s Medical Marijuana Act. If your seizures have not responded to standard medications, you may be eligible for a PA MMJ card and this page is going to walk you through everything you need to know, honestly and completely.
Does Intractable Seizures Qualify for a PA MMJ Card in Pennsylvania?
Yes — absolutely and unambiguously yes.
Intractable seizures is one of the 24 serious medical conditions explicitly listed under the Pennsylvania Medical Marijuana Act (Act 16 of 2016), as recognised by the Pennsylvania Department of Health. It appears as its own standalone qualifying condition, separate from epilepsy, which is also listed on its own.
This means that Pennsylvania patients whose seizures have not been controlled by standard antiseizure medications have two separate qualifying pathways: intractable seizures and epilepsy. Your certifying physician can note one or both during your appointment either way, you get the same PA MMJ card and the same access to Pennsylvania dispensaries.
There is no requirement that your seizures be of a specific type or frequency. There is no minimum number of medications you must have tried (though in practice, drug-resistance is typically defined as failing two or more appropriate antiseizure drugs). There is no severity threshold. If your seizures are not adequately controlled by conventional treatment and a licensed physician confirms that, you qualify.
Pennsylvania is one of the very few states that has explicitly separated intractable seizures from general epilepsy as a distinct qualifying condition. That was not an accident. The Pennsylvania legislature recognised that drug-resistant seizures represent a uniquely urgent medical need, one that deserves its own pathway rather than being buried inside a broader category.
Sources:
- Pennsylvania Department of Health – Medical Marijuana Qualifying Conditions
- 28 Pa. Code Appendix A – Serious Medical Conditions
What “Intractable” Actually Means — And Why It Matters for Your Card
The word intractable comes from the Latin for “cannot be handled.” In seizure medicine, it means seizures that keep happening despite genuine, adequate attempts at treatment. The clinical term you may also hear is drug-resistant epilepsy, defined by the International League Against Epilepsy as the failure of two or more appropriate, adequately dosed antiseizure medications to achieve sustained seizure freedom.
About one in three people with epilepsy will develop drug-resistant seizures. That is not a small number. It means that roughly three million Americans, including hundreds of thousands of Pennsylvanians, are living with seizures that their current medications cannot fully control.
For many of those people, “trying another medication” has already happened more times than they can count. The seizures may be less frequent than they once were, or they may have shifted in character, or they may be exactly as relentless as they always were. The medications may have brought side effects, cognitive slowing, weight changes, mood disruption, bone density loss, that feel like their own kind of burden on top of the seizures themselves.
Intractable seizures do not look the same for everyone. They may be:
Dravet syndrome — a severe genetic epilepsy that typically begins in the first year of life, usually triggered initially by fever, and progresses to multiple seizure types, developmental delay, and in many families, a constant background of fear. Dravet is one of the conditions with the most powerful evidence for cannabidiol-based treatment. Parents of children with Dravet syndrome were among the earliest advocates who pushed the conversation about cannabis and seizures into the mainstream, their stories changed the national conversation and ultimately led to the first FDA approval of a cannabis-derived medicine in US history.
Lennox-Gastaut syndrome (LGS) — a severe childhood-onset epilepsy involving multiple seizure types, including the frightening “drop seizures” that happen without warning and cause falls and injuries. LGS comes with cognitive challenges, a lifetime of complex medication management, and for families, an exhaustion that runs very deep. The evidence for CBD in LGS is among the strongest in the entire cannabis medicine space.
Tuberous Sclerosis Complex (TSC) — a genetic condition that causes tumours to grow in the brain and other organs, and brings epilepsy in up to 90% of those affected. For many TSC families, seizure control is a daily, ongoing struggle that has shaped everything from schooling to sleep to employment.
Drug-resistant focal epilepsy — many adults and children have drug-resistant seizures that do not fit into one of the named syndromes above. Post-traumatic epilepsy, cortical dysplasia, and idiopathic drug-resistant focal epilepsies are equally valid, equally exhausting, and equally qualifying under Pennsylvania’s medical marijuana program.
Whatever form intractable seizures takes in your life or your child’s life, the PA MMJ program was designed to include you.
Why Cannabis Has Always Been Part of the Seizure Conversation
Long before the clinical trials, long before the FDA approvals, long before any of the science we will cover in this page, families were already using cannabis for their children’s seizures. And many of them were doing it quietly, carefully, and often in legal grey areas, because they had tried everything else and they were desperate.
The story that changed everything was Charlotte Figi, a Colorado girl with Dravet syndrome who was having up to 300 grand mal seizures a week as a toddler. Her family began giving her a CBD-rich cannabis extract in 2012. Her seizures dropped to roughly three to four per month. Her story went viral. CNN covered it. Parents across the country, including parents in Pennsylvania, started asking neurologists questions they had never asked before.
The medical establishment was initially sceptical. That scepticism was not unreasonable, the evidence at the time was almost entirely anecdotal. But it prompted researchers to design the rigorous clinical trials that have since produced some of the most impressive results in epilepsy medicine in a generation. The families who spoke up, who moved to cannabis-legal states, who fought for their children, they created the evidence base that now exists.
Pennsylvania parents were part of that story. When Pennsylvania was debating Act 16, parents across the country and in Pennsylvania treating children with seizure disorders reported that use of medical marijuana had significantly reduced or completely eliminated seizures. Their testimony helped shape the law that now gives you a legal path forward.
The Science: What Research Actually Shows
The Most Important Thing to Understand First
Before getting into the studies, there is something you absolutely need to know, something that almost no cannabis website explains clearly, and that matters enormously for how you use your PA MMJ card wisely.
There are two different things being discussed when people talk about “cannabis for seizures”:
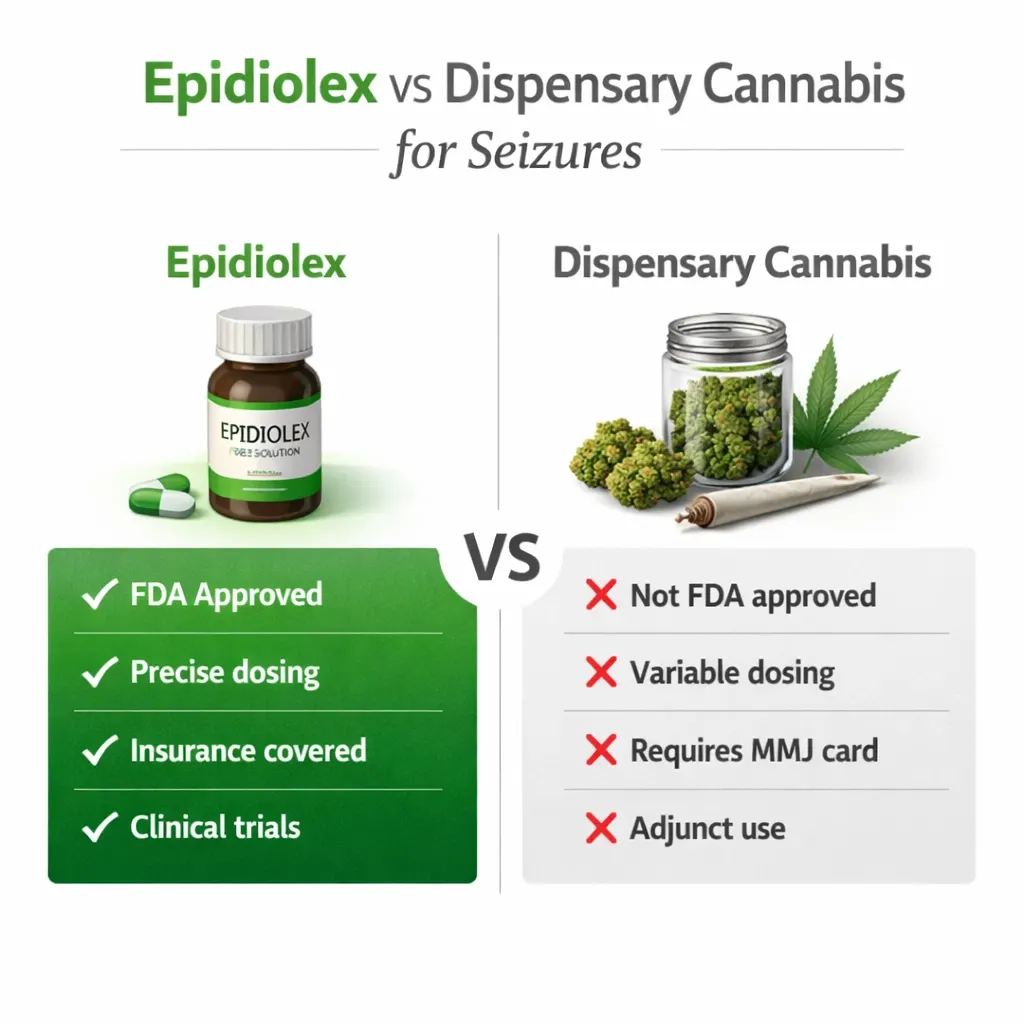
Epidiolex is a pharmaceutical-grade, FDA-approved prescription oral solution containing nearly 100% purified cannabidiol (CBD). It was approved by the FDA in June 2018, making it the first cannabis-derived medicine ever approved in the United States. It is prescribed by neurologists, dosed in precise mg/kg amounts, covered by many insurance plans, and backed by multiple Phase 3 randomised controlled trials. It is a real medicine with a real regulatory approval.
Pennsylvania dispensary cannabis products are CBD oils, tinctures, capsules, and other forms available through your PA MMJ card. They are not the same formulation as Epidiolex, not manufactured to the same pharmaceutical standard, and not FDA-approved seizure treatments. They can be genuinely useful but they are not identical to the drug studied in those landmark clinical trials.
This does not mean your PA MMJ card is not valuable. It absolutely is. But understanding the difference helps you use it in the right way, and makes sure you never accidentally replace a neurologist-managed treatment plan with self-directed dispensary products.
With that context established, here is what the research actually shows.
Dravet Syndrome: The Landmark Evidence
The study that changed everything was published in the New England Journal of Medicine in 2017. Researchers from 23 sites across the US and Europe enrolled 120 children and young adults aged 2–18 with Dravet syndrome who were still having four or more convulsive seizures per month despite standard treatment.
Half received pharmaceutical CBD (20 mg/kg/day) added to their existing medications. Half received placebo.
The results were striking. Seizure frequency in the CBD group dropped by 39%, from a median of 12.4 convulsive seizures per month before treatment to 5.9 with CBD, compared with a reduction from 14.9 to 14.1 in the placebo group. More than four in ten patients receiving CBD achieved at least a 50% reduction in seizure frequency. Five percent became completely seizure-free during the trial period.
For families who have lived with Dravet syndrome, who know what 12 seizures a month looks like, what the ambulance rides and the emergency medication and the sleepless nights look like, a 39% reduction is not a small statistical finding. It is a profound change in daily life.
- Source: NEJM – Trial of Cannabidiol for Drug-Resistant Seizures in Dravet Syndrome (Devinsky et al., 2017)
Lennox-Gastaut Syndrome: Drop Seizures and Real Relief
Two pivotal Phase 3 trials in LGS followed, published in the New England Journal of Medicine in 2018. These trials focused specifically on drop seizures, the atonic and tonic events that happen without warning and send children crashing to the floor, into furniture, into injury.
This trial involving children and adults with Lennox-Gastaut syndrome showed that pharmaceutical CBD at doses of 10 mg/kg/day and 20 mg/kg/day resulted in significantly greater reductions in drop seizure frequency than placebo. Eight patients (5%) who received CBD were completely free from drop seizures during the entire maintenance phase, compared with one patient in the placebo group.
For LGS families managing the physical danger of unpredictable falls, the helmets, the padded rooms, the constant supervision, the injuries, any meaningful reduction in drop seizure frequency is genuinely life-changing.
- Source: NEJM – Effect of Cannabidiol on Drop Seizures in the Lennox-Gastaut Syndrome (Devinsky et al., 2018)
Tuberous Sclerosis Complex: A Third FDA Approval
The JAMA Neurology trial (Thiele et al., 2021) established CBD’s efficacy for TSC-associated seizures, completing the evidence base that led to a third FDA-approved indication. Epidiolex is now the first and only FDA-approved prescription CBD to treat seizures associated with Lennox-Gastaut syndrome, Dravet syndrome, or tuberous sclerosis complex in patients one year of age or older.
Three separate FDA approvals for three distinct, severe epilepsy conditions, driven by randomised controlled trials published in the most respected medical journals in the world. This is not fringe medicine. This is some of the strongest evidence in modern epilepsy treatment.
The Pittsburgh Experience: Pennsylvania-Specific Data
Closer to home, neurologists at the University of Pittsburgh enrolled Pennsylvania patients in the state’s MMJ program beginning in January 2018, in one of the first real-world studies of cannabis for intractable seizures in Pennsylvania specifically. From January 2018, 22 patients were enrolled. Preliminary analysis of the 17 patients with post-transition follow-up longer than three months showed a decrease in seizure frequency by at least 50% in 12 patients. Patients, on average, reported lower levels of fear and anxiety with improved energy post-transition.
Twelve out of seventeen Pennsylvania patients, that is more than 70%, achieving at least a 50% seizure reduction. These are real Pennsylvania people, not clinical trial participants in controlled settings. And the improvement in fear and anxiety alongside the seizure reduction reflects something important: living with intractable seizures is not just about the seizures. It is about everything the seizures take from you.
It Is Not Just About the Seizures
The clinical trials measure seizure frequency because that is what you can count. But the families living with Dravet, LGS, and other drug-resistant epilepsies know that the seizures are only part of the story. There is also the sleep. The anxiety. The alertness. The ability to communicate. The moments of connection.
The 2023 BECOME survey asked 498 caregivers of children and adults on CBD treatment about outcomes beyond seizure counts. The findings were striking across every domain measured:
- 85% reported improvements in alertness, cognition, and executive function
- 82% reported improvements in emotional functioning
- 79% of caregivers of non-verbal patients reported improvements in language and communication
- 51% reported improvements in sleep quality
- 51% reported improvements in activities of daily living
And crucially — improvements in non-seizure outcomes were also reported in patients who either had no change or worsening of seizure frequency. This matters deeply for families where complete seizure control has not been achieved. Even when the seizures themselves do not fully respond, something else may still improve. The child may sleep better. May be more present. May communicate in ways they were not communicating before.
Overall, 93% of caregivers reported planning to continue CBD treatment, primarily because of reduced seizure burden but also because of improvements in non-seizure-related outcomes.
The Epidiolex vs. PA Dispensary Question — Answered Honestly
This is the question families ask most often, and most cannabis websites dance around it. Let us answer it directly.
If your child has Dravet syndrome, Lennox-Gastaut syndrome, or tuberous sclerosis complex: The first conversation should be with your neurologist about Epidiolex, the FDA-approved, precisely dosed, insurance-covered pharmaceutical CBD. That is the product the clinical trials tested. That is the product with the established dosing protocols and the safety monitoring guidelines. Your neurologist can prescribe it.
So why would anyone with one of these conditions also need a PA MMJ card?
There are several genuinely good reasons:
Insurance prior authorisation for Epidiolex can take time, get denied, or lapse during appeals. A PA MMJ card provides access to high-quality CBD-dominant dispensary products in the meantime, not identical to Epidiolex, but a meaningful bridge.
Epidiolex contains only CBD. Many patients and families, particularly adults, find that small amounts of THC alongside CBD help with sleep quality, anxiety, pain, and the overall emotional burden of living with severe epilepsy. A PA MMJ card enables access to complementary products alongside a prescription Epidiolex regimen, with your neurologist’s knowledge.
For patients whose drug-resistant epilepsy does not fall into the three FDA-approved Epidiolex indications, and that includes the majority of drug-resistant epilepsy patients, a PA MMJ card may be the most accessible route to a CBD-dominant product while conventional insurance pathways are navigated.
The bottom line: A PA MMJ card and Epidiolex are not competitors. For many Pennsylvania patients and families, they work together. The MMJ card fills gaps, provides complementary options, and ensures access is never interrupted by insurance bureaucracy.
Drug Interactions: What Every Intractable Seizure Patient in PA Needs to Know
This is the section that separates genuine, useful information from what most cannabis websites publish. Every person with intractable seizures is already taking antiseizure medications. Some of those medications interact with CBD in ways that require real monitoring, not precautionary boilerplate, but actual clinical attention.
Please read this section before starting any cannabis product. And please share it with your neurologist.
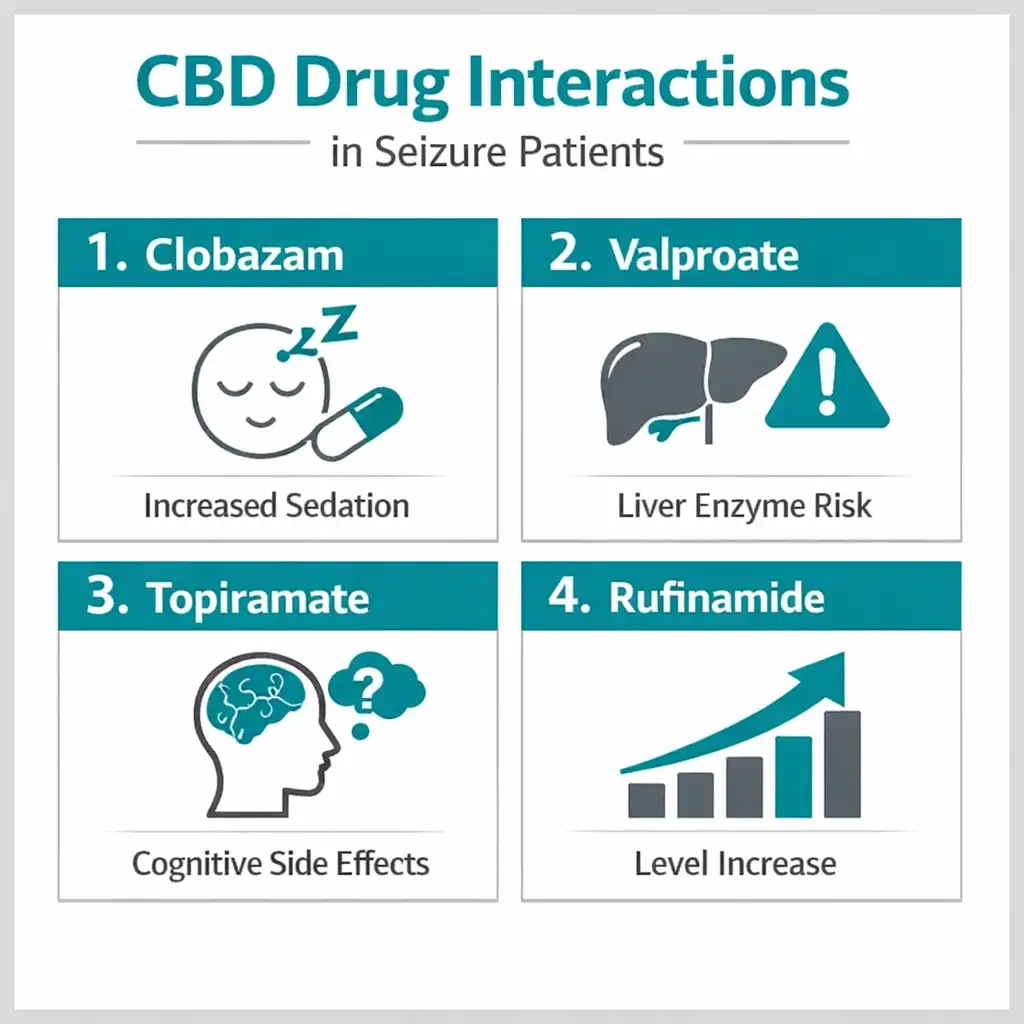
If You Take Clobazam (Onfi) — This Is the Most Important Interaction
Clobazam is one of the most commonly used antiseizure medications in LGS and Dravet syndrome. If you take it, the interaction with CBD is the most significant one you will encounter.
CBD inhibits certain liver enzymes involved in metabolising clobazam. The result is that the active metabolite of clobazam, called N-desmethylclobazam or norclobazam, builds up to much higher levels in your system when CBD is added. Levels of the active metabolite of clobazam showed increased plasma levels up to 8 times when used in conjunction with CBD, associated with somnolence.
Eight times. That is not a small increase. It explains why many patients on clobazam who add CBD become unusually sleepy, and why neurologists often need to reduce the clobazam dose when CBD is introduced.
There is also a nuance worth knowing: some researchers have raised the question of whether CBD’s apparent anticonvulsant benefit in clinical trials partially reflects this pharmacokinetic enhancement of clobazam, essentially, CBD raising clobazam to higher levels, which then does more of the seizure-control work. This question is not fully resolved scientifically. What it means practically is that clobazam-CBD co-administration needs active neurologist supervision, not just awareness.
What to do: Talk to your neurologist before starting any CBD product if you take clobazam. Clobazam dose adjustment is often needed. Do not add CBD and expect your clobazam dose to stay the same.
Sources:
- PubMed – Interactions Between CBD and Commonly Used Antiepileptic Drugs (Gaston et al., 2017)
- PubMed – Drug-Drug Interaction Between Clobazam and CBD in Children with Refractory Epilepsy
If You Take Valproate (Depakote, Depakene) — Liver Monitoring Is Required
Valproate is widely used in epilepsy and is part of the standard treatment protocol in Dravet syndrome. When CBD is combined with valproate, the risk of liver enzyme elevation (transaminase elevation) increases substantially.
The FDA’s Epidiolex prescribing label reports clearly: the majority of ALT elevations in the controlled studies occurred in patients taking concomitant valproate. The incidence of ALT elevations greater than 3 times the upper limit of normal was 30% in patients taking both concomitant valproate and clobazam, and 21% in patients taking concomitant valproate without clobazam, compared with 3% in patients taking neither drug.
This does not mean the combination is forbidden. It means it needs to be actively monitored. Liver function tests (ALT, AST, total bilirubin) should be done before starting CBD, and at intervals afterward. Most elevations resolve when doses are adjusted. But you cannot manage what you are not monitoring.
What to do: If you take valproate, get baseline liver function tests before starting any CBD product and discuss an ongoing monitoring schedule with your neurologist or prescribing physician.
If You Take Topiramate (Topamax) — Watch for Increased Side Effects
Researchers found increases in serum levels of topiramate with increasing CBD dose. Topiramate already causes cognitive side effects, word-finding difficulty, mental slowing, what many patients call “Dopamax fog.” Higher topiramate levels from CBD interaction can intensify these effects. If you are on topiramate and add CBD and notice increased cognitive dulling, mention it to your neurologist.
If You Take Rufinamide (Banzel) — Dose Adjustment May Be Needed
Rufinamide is used specifically in LGS management. CBD raises rufinamide serum levels. In clinical trials this did not produce serious safety events, but rufinamide dose reduction may be appropriate when CBD is introduced in patients on this combination.
If You Take Levetiracetam (Keppra) or Lamotrigine (Lamictal)
These widely used antiseizure medications do not show the same concerning interaction signals as clobazam and valproate. Clinically significant serum level changes were not identified for levetiracetam or lamotrigine in the primary interaction studies. Standard monitoring is still sensible, but these are lower-concern combinations.
If You Take Stiripentol (Diacomit)
Stiripentol is used in Dravet syndrome in combination with clobazam and valproate. If you are on all three, stiripentol, clobazam, and valproate, adding CBD means navigating multiple interactions simultaneously. This combination requires particularly careful neurologist-supervised monitoring. Do not add CBD to this regimen without your neurologist’s active involvement.
The Overall Message
“A perception exists that since CBD is plant-based, it is natural and safe; and while this may be mostly true, CBD, just like other antiepileptic drugs, has interactions with other seizure drugs that patients and providers need to be aware of.”
That is not a reason to be afraid. It is a reason to be informed and to make sure your neurologist knows what you are doing.
Pennsylvania Dispensary Product Guidance for Intractable Seizures
The Most Important Rule: CBD-Dominant Products Only
THC is not the seizure-control compound. CBD is. When you walk into a Pennsylvania dispensary for intractable seizures, you are looking for CBD-dominant products with the highest CBD:THC ratio available, at minimum 20:1, preferably higher.
High-THC products are not appropriate for seizure management and may at higher doses lower the seizure threshold or interfere with how your brain responds to your existing antiseizure medications. This is not a theoretical concern, it is a practical one. Please tell the dispensary pharmacist you have intractable seizures, tell them your medications, and ask specifically for high-CBD-ratio products.
CBD Oils and Tinctures
These are the most appropriate and versatile format for seizure management. Taken sublingually (under the tongue), they have a faster onset, typically 15–45 minutes, than capsules. For patients managing breakthrough seizure clusters or needing more responsive dosing, sublingual tinctures offer the most control.
Start low and go slow. Begin with a small CBD dose (5–10 mg CBD equivalent) and increase gradually over several weeks. CBD bioavailability varies, taking oil products with a small amount of fat (like a little full-fat dairy or nut butter) significantly improves absorption and consistency.
CBD Capsules
Capsules provide more consistent dosing than tinctures for daily maintenance use. They take longer to work, 60–120 minutes but for patients using CBD as a daily adjunct rather than an acute intervention, the slower and more stable release can be an advantage. Capsules are also easier for caregivers managing pediatric or adult patients who cannot take sublingual oils easily.
What to Avoid
Say no to high-THC products for seizure management. THC-dominant vaporisable flower, THC edibles, THC tinctures, these are not appropriate for this condition. Some adults with epilepsy may find small, controlled amounts of THC helpful for sleep or anxiety as a secondary goal, but only with neurologist awareness and at very conservative doses.
For Children
Pennsylvania permits minors to participate in the MMJ program through a parent or legal guardian caregiver registration. For pediatric patients, oil formats in precise small doses are generally the most practical. Avoid any product that cannot be accurately dosed by volume.
At the Dispensary
Tell the pharmacist: “I have intractable seizures. I am on [your medications]. I need the highest CBD:THC ratio you have, in an oil or capsule.” A knowledgeable dispensary pharmacist will guide you to appropriate products. If they steer you toward high-THC products, ask why specifically and push back if the answer is not convincing.
Pediatric Patients: What Pennsylvania Parents Need to Know
A very large part of the intractable seizure community in Pennsylvania is made up of children and their families. The PA Medical Marijuana Act was written with them in mind.
Minors qualify for the PA MMJ program. A parent or legal guardian registers as the minor’s caregiver through the PA Medical Marijuana Patient Registry. The caregiver is responsible for acquiring and administering cannabis on the child’s behalf. The child still requires a physician certification from a PA DOH-registered certifying physician, but that process is the same telehealth appointment described below.
Pennsylvania law also provides that it is not a violation of state law if a parent or guardian of a minor lawfully obtains medical marijuana from another state, territory, or country to administer to the minor, an important legal protection for families who may have sought cannabis access before Pennsylvania’s own program was fully operational.
For families with a Dravet, LGS, or TSC diagnosis in a child: Please pursue Epidiolex through your child’s neurologist as the primary, FDA-approved pathway. A PA MMJ card is a powerful complementary tool, for access during insurance delays, for non-seizure symptom support, for flexibility, but it is not a substitute for neurologist-managed care in severe pediatric epilepsy. The drug interaction concerns with clobazam and valproate are especially important in children because of weight-based dosing precision.
How to Get Your Pennsylvania MMJ Card for Intractable Seizures: Step by Step
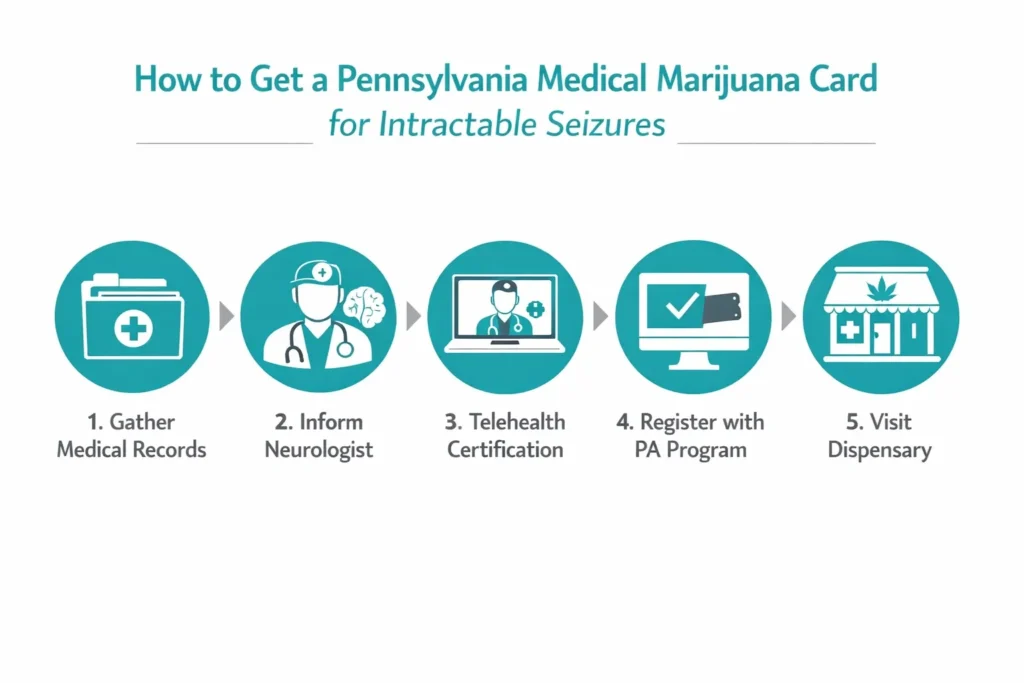
Step 1 — Pull Together Your Medical Records
Before your telehealth appointment, gather documentation that shows your seizure history and treatment resistance. This means your diagnosis from a neurologist, a list of the antiseizure medications you have tried and why they were not adequate, and your current medication list with exact names and doses. The certifying physician needs to see that your seizures are intractable, treatment-resistant, not just that you have had seizures.
You do not need to bring MRI reports or EEG results to a certifying appointment, but having them available does not hurt. The key documentation is your treatment history.
Step 2 — Tell Your Neurologist
This step is not optional for this condition. Please tell your neurologist before you start using cannabis products. The clobazam and valproate interactions are real, they require monitoring, and your neurologist needs to know what is in your system. Even if you expect pushback, have the conversation. If your neurologist is uncomfortable with cannabis, that is okay — you can still get your PA MMJ card through a separate certifying physician. What you should not do is add CBD to a regimen that includes clobazam or valproate without anyone monitoring your labs and medication levels.
Step 3 — Book a Telehealth Certification Appointment
Find a PA DOH-registered medical marijuana certifying physician and book a telehealth appointment. These are available from home – no travel, no waiting room. The appointment typically takes 10–15 minutes. Tell the certifying physician you have intractable seizures, share your diagnosis and medication history, and ask to be certified under both intractable seizures and epilepsy if both apply. The physician submits your certification electronically to the Pennsylvania Department of Health.
Step 4 — Register with the PA MMJ Program
After your certification is submitted, go to the PA Medical Marijuana Program Patient Registry at patientportal.mmapinc.com and complete your registration with:
- Your physician certification (submitted electronically by your certifying doctor)
- A valid Pennsylvania driver’s licence or state-issued ID
- The $50 annual registration fee
If cost is a barrier, fee waivers are available for Pennsylvania patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC. You should not let the fee stand between you and access to this program.
Step 5 — Your First Dispensary Visit
When you arrive at a Pennsylvania dispensary, introduce yourself as a patient with intractable seizures who is on antiseizure medications. Name your specific medications, especially clobazam and valproate if you take them. Ask for CBD-dominant oils or capsules with the highest available CBD:THC ratio. A good dispensary pharmacist will take the time to explain your options and suggest a starting dose.
Do not leave without knowing the CBD and THC content per dose of whatever you purchase. Precise dosing matters for this condition more than almost any other.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Tourettes
- Chronic Hepatitis C
- Anxiety Disorder
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: My child has Dravet syndrome. Should I pursue Epidiolex through their neurologist or a PA MMJ card — or both?
Q: My seizures are not Dravet or LGS — just drug-resistant focal epilepsy. Do I still qualify?
Q: Will cannabis stop my seizures completely?
Q: I take clobazam. Is it safe to use CBD products from a PA dispensary?
Q: I take valproate. What do I need to do before starting CBD?
Q: My neurologist says cannabis is not a treatment for epilepsy. Are they right?
Q: Do I need to fail a specific number of medications to qualify?
Q: Can cannabis make seizures worse?
Pennsylvania Support Resources for Intractable Seizure Patients and Families
Epilepsy Foundation of Western/Central Pennsylvania — efwp.org Serving Pittsburgh, western, and central PA with support groups, education, emergency preparedness resources, and school advocacy for children with epilepsy. One of the most valuable local resources for Pennsylvania families managing any form of intractable seizures.
Epilepsy Foundation of Eastern Pennsylvania — epilepsyeasternpa.org Serving the Philadelphia region and eastern Pennsylvania with support groups, caregiver resources, and referral services.
Dravet Syndrome Foundation — dravetfoundation.org The leading US advocacy and research organisation for Dravet syndrome. Provides family support, clinical trial information, and resources on cannabidiol treatment specifically for Dravet families. If your child has Dravet syndrome, this should be your first support community call.
Lennox-Gastaut Syndrome Foundation — lgsfoundation.org The primary US patient advocacy organisation for LGS families, with caregiver education, clinical trial listings, and specific resources on CBD treatment for drop seizures and LGS-related quality of life.
Tuberous Sclerosis Alliance — tscalliance.org Research updates, patient advocacy, and support resources for the TSC community, including guidance on epilepsy management and cannabidiol access.
Epilepsy Foundation — epilepsy.com Comprehensive patient-facing information on drug-resistant epilepsy, treatment options, and how to access clinical trials.
Children’s Hospital of Philadelphia (CHOP) — Epilepsy Program One of the top pediatric epilepsy centres in the United States, treating many of Pennsylvania’s most complex pediatric epilepsy cases including Dravet, LGS, and TSC.
UPMC Children’s Hospital of Pittsburgh — Epilepsy Program Serving western Pennsylvania families with specialist paediatric epilepsy care and access to clinical research.
A Final Word for Pennsylvania Patients and Families
If you have been living with intractable seizures or loving someone who has — you already know that the system does not always move fast enough. You have waited for appointments, waited for insurance approvals, waited to see if the next medication would finally be the one that worked.
Pennsylvania’s medical marijuana program is not a miracle. It is a tool. And for many people with intractable seizures, it is a meaningful one, backed by some of the most compelling clinical trial evidence in the history of epilepsy medicine, supported by real Pennsylvania patient data, and accessible through a straightforward telehealth process that does not require you to leave your home.
The evidence is clearest for Dravet syndrome and Lennox-Gastaut syndrome. The evidence for other drug-resistant epilepsies is growing. The non-seizure benefits, sleep, anxiety, alertness, quality of life, are real and clinically documented.
Use your PA MMJ card well. Choose CBD-dominant products. Keep your neurologist informed. Monitor the interactions that need monitoring. And do not let anyone, insurance company, bureaucratic process, or the gap between what exists today and what should exist tomorrow, stand between you and the access the Pennsylvania law says you deserve.