
Pennsylvania’s medical marijuana program covers 24 conditions, a list that has expanded meaningfully since the Medical Marijuana Act was signed in 2016. Whether you were recently diagnosed, have been managing a condition for years, or are looking at medical cannabis as an alternative to medications that aren’t working, understanding the full scope of what qualifies is the first step toward obtaining a Pennsylvania medical marijuana card.
Before applying, it’s helpful to understand the full Pennsylvania medical marijuana laws governing patient eligibility, possession limits, and dispensary purchases.
This page covers every qualifying condition, what Pennsylvania law actually says about each, what the research shows, and how to start the certification process if you decide to move forward.
🎬 Watch This First – Thousands of Pennsylvania Patients Are Getting Legal Relief and Most Don’t Even Know They Qualify

How Pennsylvania’s Qualifying Conditions Work?
Pennsylvania’s Medical Marijuana Act (MMA), signed into law on April 17, 2016 as Act 16, created the framework for the state’s medical cannabis program. The Pennsylvania Department of Health (DOH) administers the program and maintains the official list of approved conditions. Under the MMA, the DOH’s Medical Marijuana Advisory Board can add conditions through a formal review process, which is how the list has grown from the original conditions to 24 today.
To qualify for a Pennsylvania medical marijuana card, a physician registered with the DOH, such as Dr. Johnathon Chance Miller, MD must certify that you have been diagnosed with one of the 24 approved conditions and that medical marijuana is appropriate for your situation. The physician does not prescribe cannabis the way they prescribe other medications, they issue a certification that authorizes you to register with the state program.
The DOH’s complete, current list of qualifying conditions is maintained at pa.gov/guides/pennsylvania-medical-marijuana-program.
The 24 Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
- Chronic Hepatitis C
1. Amyotrophic Lateral Sclerosis (ALS)
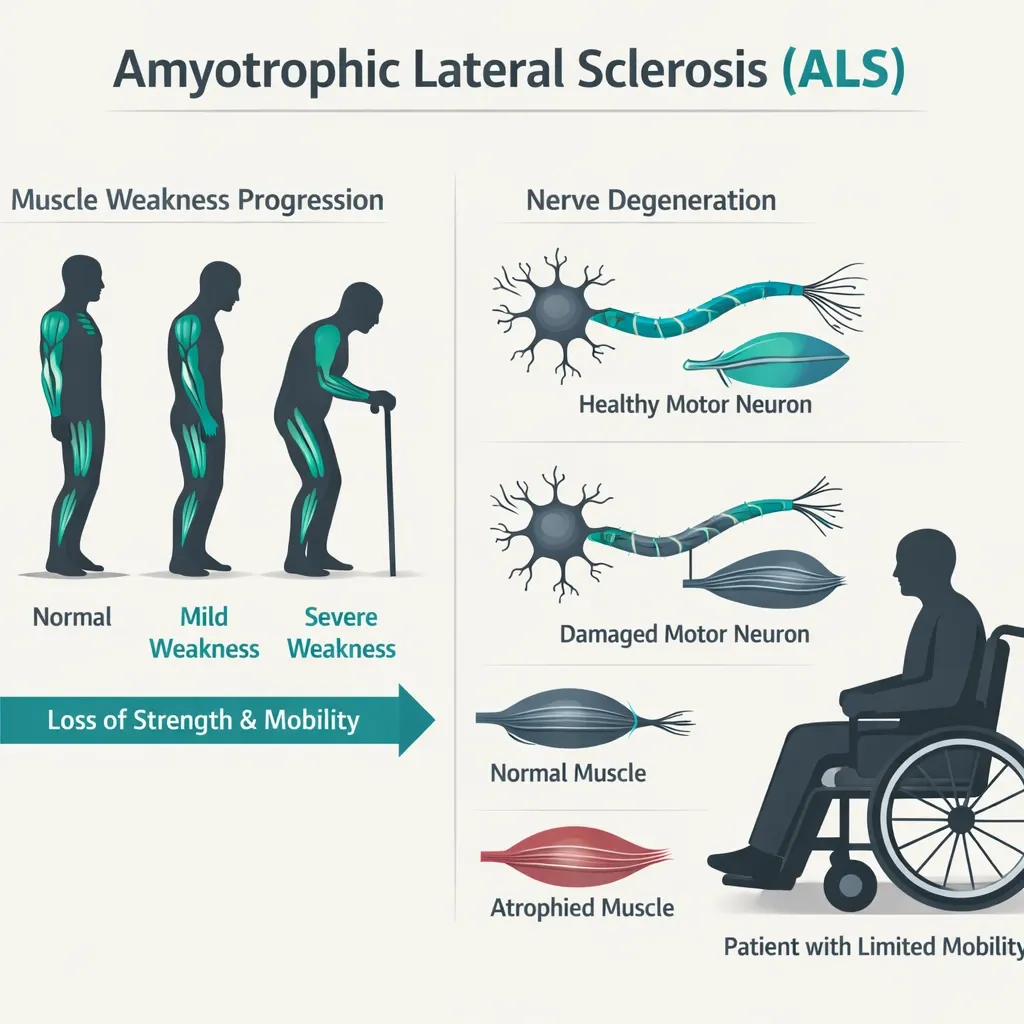
ALS is a progressive neurodegenerative disease that destroys the nerve cells controlling voluntary muscle movement. It is among the most serious conditions on Pennsylvania’s qualifying list and also one where palliative symptom management becomes the central goal of care relatively early in the disease course.
Research context: A 2019 survey published in Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration found that a significant percentage of ALS patients reported using cannabis to address symptoms including spasticity, pain, drooling, appetite loss, and depression. The ALS Association has recognized the need for formal research into cannabinoids for ALS symptom management. Evidence supporting the direct use of cannabis for ALS is still largely observational, controlled trial data remains limited but the symptom profile of ALS (spasticity, pain, appetite disruption, sleep problems) overlaps substantially with areas where cannabis has shown benefit in other populations.
Pennsylvania notes: ALS is also separately covered under the “dyskinetic and spastic movement disorders” category and the “damage to nervous tissue with intractable spasticity” category, meaning patients may qualify under multiple conditions.
2. Autism

Pennsylvania added autism spectrum disorder (ASD) as a qualifying condition recognizing that many patients, particularly those with severe behavioral symptoms, self-injurious behavior, and treatment-refractory anxiety have not found adequate relief from conventional interventions.
Research context: A 2019 study published in Scientific Reports (Barchel et al.) evaluated medical cannabis in 53 children with ASD. Parents reported improvements in behavioral outbursts, anxiety, communication problems, and sleep disruption. A 2020 study in Nature Medicine (Aran et al.) assessed cannabidiol (CBD)-rich cannabis treatment in 150 pediatric ASD patients and found improvements in disruptive behavior and anxiety. These are early-stage studies, but they represent meaningful real-world data from pediatric ASD populations.
For adult patients with ASD, the qualifying pathways often involve associated symptoms: anxiety, sleep disruption, chronic pain from self-injury, where cannabis has a better-established evidence base.
3. Cancer, Including Remission Therapy
Cancer is broadly qualifying in Pennsylvania and notably, the condition language includes remission therapy, which means patients who have completed active treatment but are managing ongoing symptoms related to their cancer history or treatment also qualify.
Research context: This is one of the most studied areas for medical cannabis. Cannabinoids have demonstrated antiemetic properties (reducing chemotherapy-induced nausea and vomiting), a finding supported by decades of research and reflected in the FDA approval of dronabinol (synthetic THC) for chemotherapy nausea since 1985. A 2022 systematic review in the Journal of Pain and Symptom Management covering 52 studies and 4,786 participants found positive signals for pain, nausea, appetite, and sleep in cancer patients. The evidence quality is rated “low to very low” by formal standards due to study design limitations but the consistent directional signal across studies is meaningful.
The inclusion of remission therapy is particularly important: peripheral neuropathy from chemotherapy agents, ongoing fatigue, sleep disruption, anxiety about recurrence, and appetite problems are all conditions that may persist long after active treatment ends and that cannabis may address.
4. Crohn’s Disease
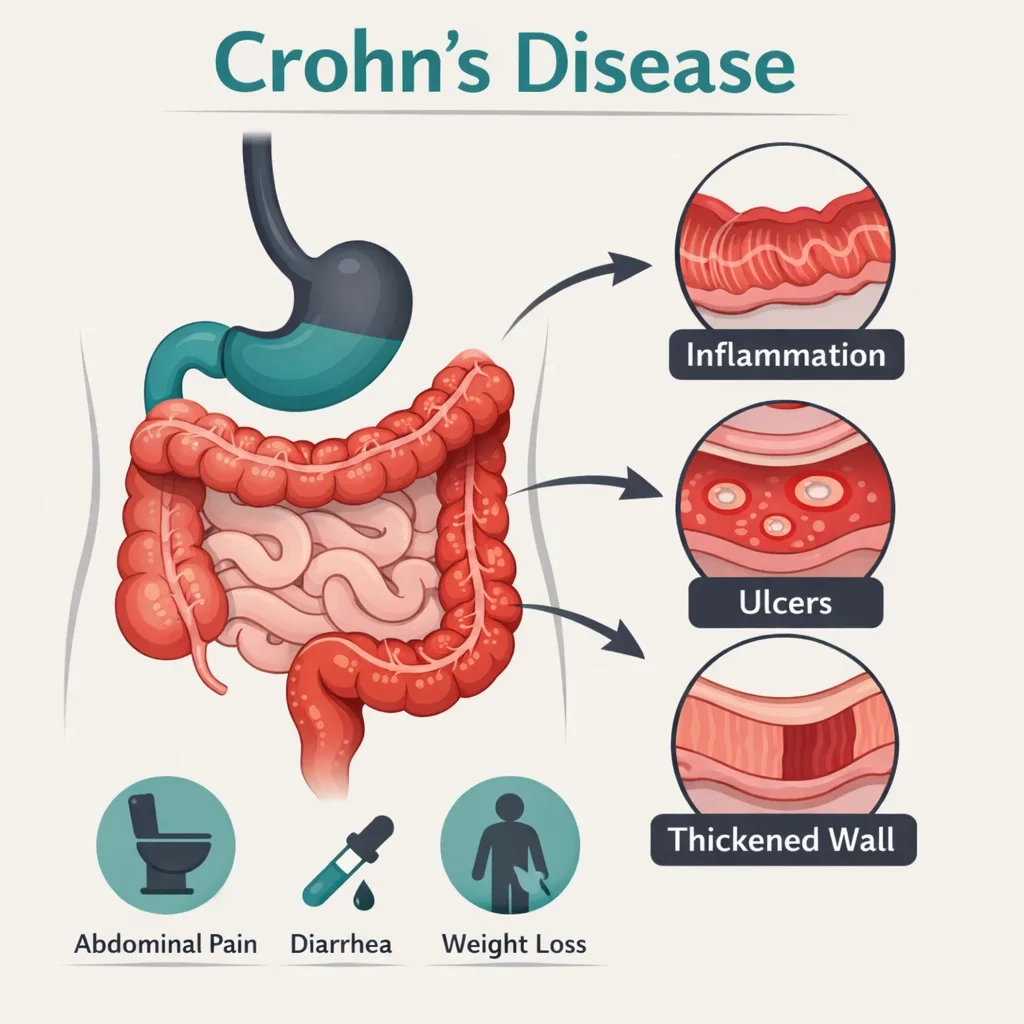
Crohn’s disease is a chronic inflammatory bowel condition affecting any part of the gastrointestinal tract. Symptoms including abdominal pain, diarrhea, weight loss, fatigue, and nausea, can be debilitating and are frequently inadequately controlled by standard therapies.
Research context: The endocannabinoid system plays a recognized role in gut motility, intestinal inflammation, and visceral pain. A 2013 randomized controlled trial published in Clinical Gastroenterology and Hepatology (Naftali et al.) found that cannabis induced complete remission in 5 of 11 active Crohn’s patients versus 1 of 10 in the placebo group. A 2017 pilot study by the same group found cannabis reduced Crohn’s Disease Activity Index scores and improved quality of life. While the evidence base remains small and formal guidelines do not yet recommend cannabis as a first-line treatment, the mechanistic rationale and early clinical data are genuinely supportive.
5. Damage to the Nervous Tissue of the Central or Peripheral Nervous System (Brain or Spinal Cord) with Objective Neurological Indication of Intractable Spasticity, and Other Associated Neuropathies
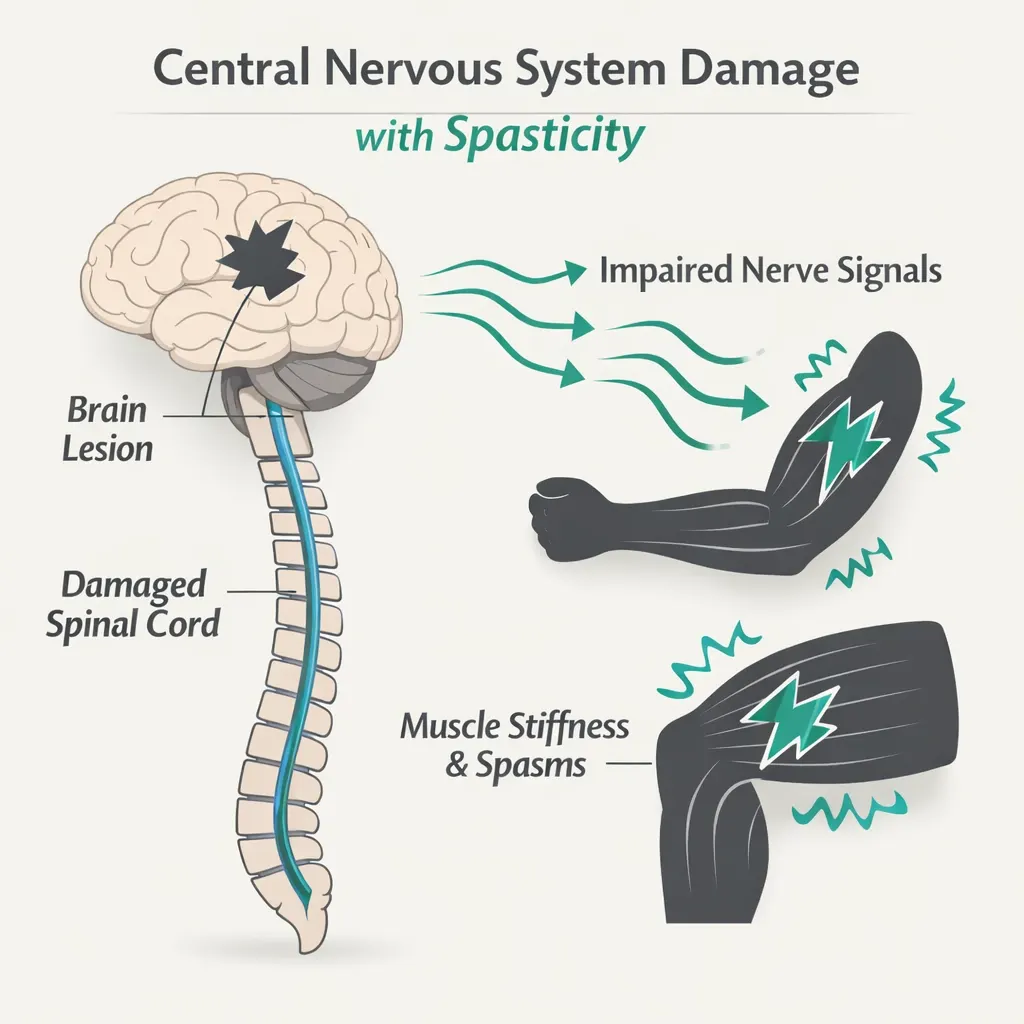
This condition is one of the more precisely worded entries on Pennsylvania’s list. It requires objective neurological indication, meaning clinical findings, not just symptoms and the spasticity must be intractable (not adequately controlled by standard treatments).
Conditions that commonly qualify under this category include spinal cord injury, traumatic brain injury with neurological sequelae, spastic cerebral palsy, and other documented CNS injury states. The “associated neuropathies” language opens the pathway to qualifying neuropathic pain arising from the central nervous system damage, not just the spasticity itself.
Research context: Cannabis for spasticity has the strongest clinical evidence base among all neurological symptoms, arguably because of early work in multiple sclerosis. Sativex (nabiximols), a cannabis-based oromucosal spray, is approved in many countries (though not the US) specifically for MS-related spasticity and has been studied extensively. Multiple systematic reviews have found evidence supporting cannabis for spasticity of neurological origin.
6. Epilepsy
Epilepsy was among the original qualifying conditions in the MMA and remains one of the strongest evidence categories for medical cannabis, particularly for treatment-refractory epilepsy syndromes.
Research context: The FDA approval of Epidiolex (pharmaceutical-grade CBD) in 2018 for Dravet syndrome and Lennox-Gastaut syndrome, two severe childhood epilepsy syndromes, represents the strongest regulatory endorsement of cannabinoid medicine to date. The pivotal trials showed significant reductions in seizure frequency versus placebo. For broader epilepsy populations, evidence is more mixed, but CBD-dominant formulations have shown consistent benefit in treatment-resistant cases.
Pennsylvania patients: Epidiolex can be prescribed by any physician as an FDA-approved drug. However, patients who want to use other cannabis formulations, including those with THC, must go through the PA MMJ program. For adult epilepsy patients, the treating neurologist is often the appropriate certifying physician, though any PA-registered physician who knows your history can certify.
7. Glaucoma
Glaucoma is characterized by elevated intraocular pressure (IOP) leading to optic nerve damage and vision loss. It is one of the original and most long-standing research areas for cannabis in medicine studies dating back to the 1970s demonstrated that THC reduces IOP.
Research context: The IOP-lowering effect of smoked and intravenous cannabis is well-documented. A 1971 study in JAMA by Hepler and Frank was among the first to establish this. The clinical challenge has always been duration: cannabis reduces IOP for only 3–4 hours, requiring very frequent dosing to maintain therapeutic effect, a practical barrier that conventional glaucoma medications don’t share. The American Glaucoma Society’s position is that while cannabis does lower IOP, the duration limitation makes it impractical as a primary glaucoma treatment. Many Pennsylvania glaucoma patients use medical cannabis as a supplemental option, particularly for symptom management or sleep, alongside standard glaucoma treatment.
8. HIV/AIDS (Positive Status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome)
Pennsylvania qualifies both HIV-positive status and AIDS, meaning you do not need to have progressed to an AIDS diagnosis to qualify. A confirmed HIV-positive diagnosis is sufficient.
Research context: Cannabis use in HIV/AIDS populations has one of the more robust observational evidence bases of any qualifying condition group. Common benefits reported include appetite stimulation and weight maintenance (cachexia is a significant complication), nausea reduction (both from the disease and from antiretroviral medications), pain management (HIV-related peripheral neuropathy is particularly difficult to treat conventionally), and anxiety reduction.
A 2007 placebo-controlled trial published in Neuropsychopharmacology found smoked cannabis significantly reduced HIV-related neuropathic pain. Dronabinol (synthetic THC) is FDA-approved for AIDS-related anorexia, giving this indication an additional regulatory anchor.
Drug interaction note: CBD can inhibit CYP3A4 and CYP2D6 enzymes that metabolize several antiretroviral medications (including protease inhibitors and NNRTIs). Disclose all antiretroviral medications to your certifying physician and dispensary pharmacist before starting cannabis.
9. Huntington’s Disease
Huntington’s disease is a fatal genetic neurodegenerative condition causing progressive deterioration of motor function, cognition, and psychiatric stability. Chorea (involuntary movements), behavioral disturbance, sleep problems, and pain are among the most difficult-to-treat symptom clusters.
Research context: The endocannabinoid system is significantly disrupted in Huntington’s disease, cannabinoid receptor density in the basal ganglia is markedly reduced in HD patients. This neurobiological rationale has driven research interest in cannabinoids for HD. A 2017 systematic review in the Journal of Huntington’s Disease found insufficient high-quality evidence to draw firm conclusions but noted the theoretical and observational basis for exploration. Survey data from HD patients consistently shows cannabis use for chorea, sleep disruption, and anxiety.
- Source: HDSA – Medical Marijuana FAQ
10. Inflammatory Bowel Disease (IBD)
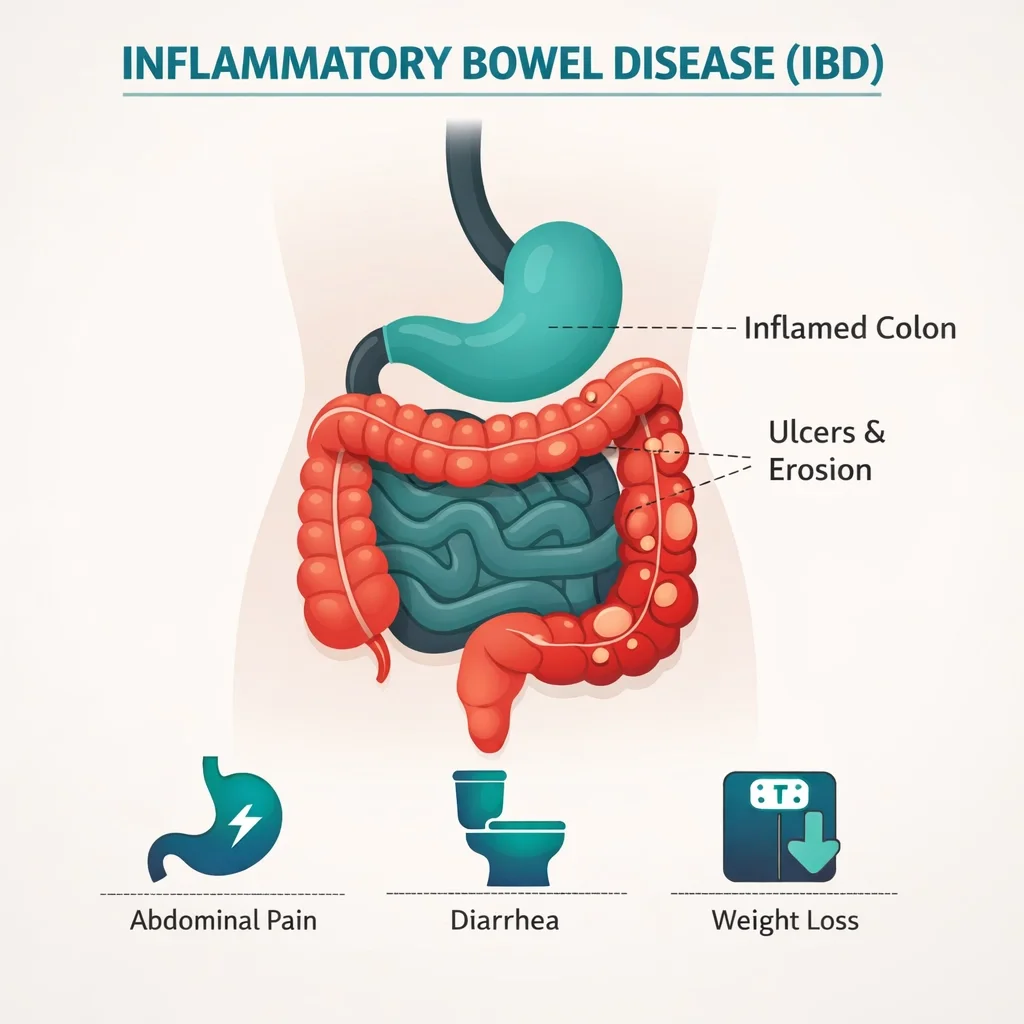
Inflammatory bowel disease encompasses Crohn’s disease and ulcerative colitis. Pennsylvania lists IBD as a separate qualifying condition from Crohn’s specifically, which means patients with ulcerative colitis, who technically qualify under IBD rather than Crohn’s, have their own explicit pathway.
Research context: The endocannabinoid system modulates intestinal motility, permeability, immune response, and visceral pain, making it a scientifically rational target for IBD. Survey studies consistently show high rates of cannabis use in IBD patient populations and high rates of self-reported benefit. A 2021 Cochrane review assessed cannabis and cannabinoids for IBD and found insufficient evidence from controlled trials to draw firm conclusions about induction or maintenance of remission, though it noted the positive direction of observational findings.
For ulcerative colitis patients who do not qualify under Crohn’s specifically, IBD is the appropriate qualifying category to discuss with your certifying physician.
11. Intractable Seizures
Pennsylvania lists intractable seizures as a qualifying condition separately from epilepsy. This is specifically intended to cover seizure disorders that do not fall under an epilepsy diagnosis, as well as to clarify access for patients whose seizures have been refractory to standard antiseizure treatments.
“Intractable” typically means the seizures have not been adequately controlled despite trials of two or more appropriately selected antiseizure medications. This is clinically meaningful, it places cannabis consideration in the context of patients for whom other options have already failed.
Research context: As with epilepsy, the FDA approval of Epidiolex for treatment-resistant seizure syndromes anchors the evidence base here. Real-world studies from patient registries and the observational literature consistently show seizure frequency reduction in intractable cases with CBD-dominant formulations.
12. Tourette Syndrome
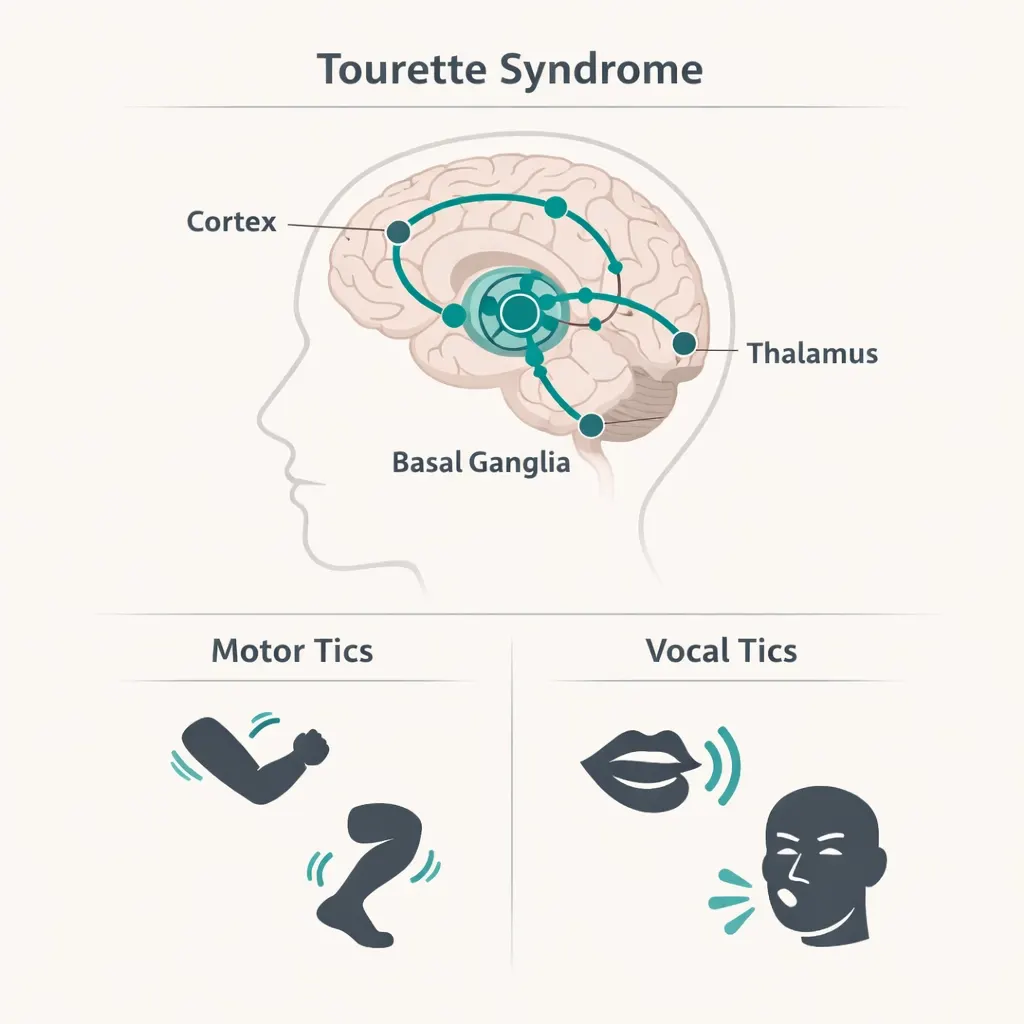
Tourette syndrome is a neurological disorder characterized by repetitive involuntary movements and vocalizations (tics). Motor and vocal tics can be severe, painful, and disruptive to daily functioning, and are frequently inadequately managed by conventional medications, many of which carry significant side effects.
Research context: A 2017 systematic review published in Behavioural Neurology assessed cannabis-based treatments for Tourette syndrome and found evidence that THC may reduce tic severity and obsessive-compulsive symptoms in TS patients. A small but positive randomized controlled trial (Müller-Vahl et al., 2002) found THC superior to placebo in reducing tic severity. The evidence base is limited by sample sizes but consistently positive in direction.
Cannabis may also address common TS comorbidities anxiety, obsessive-compulsive symptoms, sleep disruption, and ADHD-associated features, that are not well managed by tic-targeted medications.
13. Multiple Sclerosis
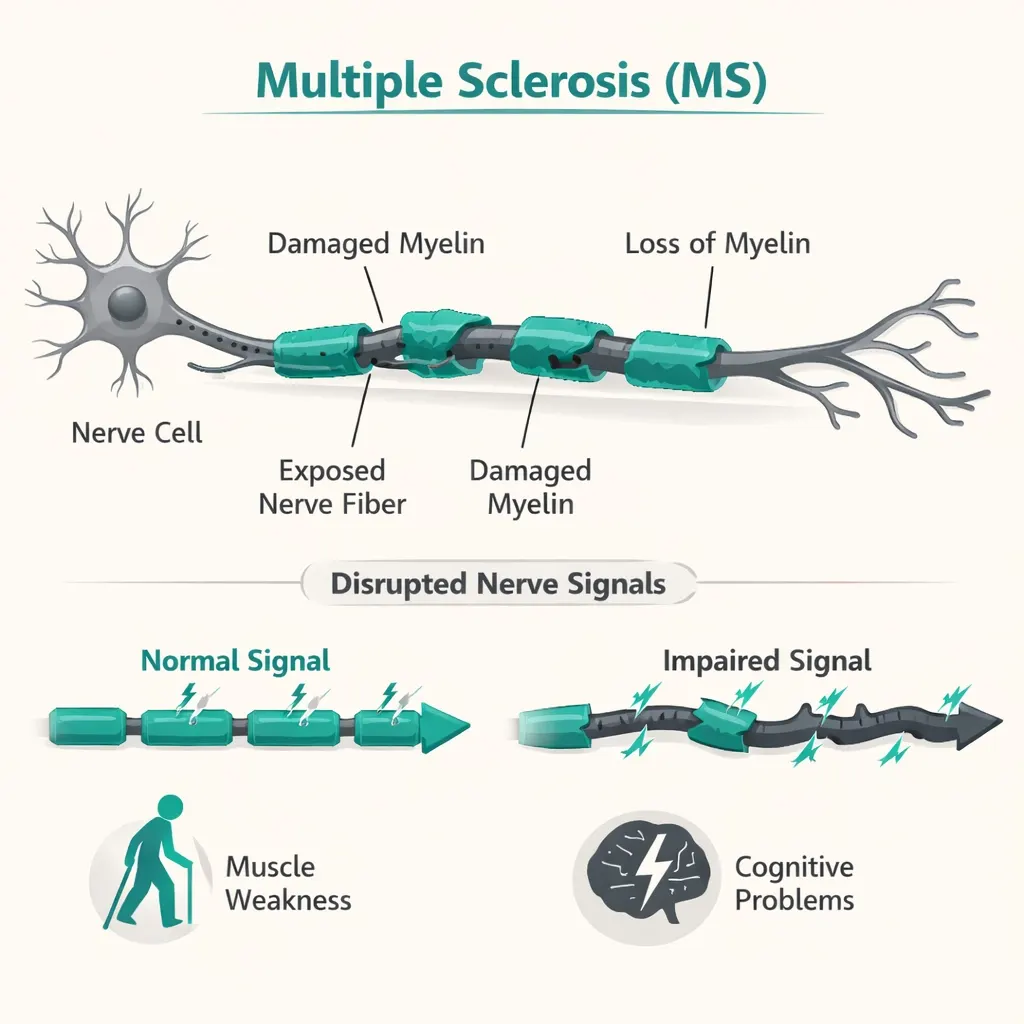
Multiple sclerosis involves demyelination of the central nervous system, producing a wide range of neurological symptoms including spasticity, pain, fatigue, bladder dysfunction, tremor, and cognitive disruption. It is one of the conditions with the most substantial clinical evidence base for cannabis.
Research context: Sativex (nabiximols, a 1:1 THC:CBD oromucosal spray) has been studied extensively in MS and is approved in Canada, the UK, and multiple European countries specifically for MS-related spasticity, the largest regulatory acknowledgment of cannabis-based medicine outside of Epidiolex for epilepsy. Patient-reported outcome measures in MS cannabis studies consistently show benefits for spasticity, pain, and sleep. The American Academy of Neurology’s 2014 guideline on complementary and alternative therapies in MS found that oral cannabis extract was probably effective for spasticity and pain, and possibly effective for bladder symptoms.
14. Neuropathies
Neuropathy — nerve damage producing pain, numbness, burning, and weakness, covers a broad category of conditions with diverse causes: diabetic neuropathy, chemotherapy-induced peripheral neuropathy (CIPN), post-herpetic neuralgia, idiopathic neuropathy, and others. Neuropathic pain is among the most treatment-resistant pain types in medicine.
Research context: Cannabis for neuropathic pain has one of the stronger evidence bases among chronic pain conditions. A 2018 Cochrane review found moderate-quality evidence supporting cannabis-based medicines for chronic neuropathic pain. A well-cited series of randomized trials from the University of California Center for Medicinal Cannabis Research (CMCR) found inhaled cannabis statistically significantly reduced neuropathic pain in HIV-related and post-traumatic/postsurgical neuropathy. Gabapentin, pregabalin, and tricyclic antidepressants, the standard neuropathic pain treatments, fail a substantial portion of patients, making this an area where cannabis has genuine clinical relevance.
15. Parkinson’s Disease
Parkinson’s disease is a neurodegenerative condition producing motor symptoms (tremor, rigidity, bradykinesia) and a wide range of non-motor symptoms (sleep disruption, pain, anxiety, psychosis, autonomic dysfunction). Both motor and non-motor symptoms can be poorly managed by dopaminergic medications alone.
Research context: A 2014 open-label pilot study published in the Journal of Psychopharmacology (Lotan et al.) found cannabis significantly improved motor and non-motor Parkinson’s symptoms. A 2020 survey study found the most commonly reported cannabis benefits in PD patients were sleep improvement, pain reduction, and tremor reduction. The interaction between the endocannabinoid system and basal ganglia circuits makes cannabinoids mechanistically plausible for PD. Formal randomized controlled trial data in PD is still limited but growing.
One important caution: cannabis, particularly high-THC products, can worsen psychotic symptoms and confusion in some PD patients, a consideration that should be discussed explicitly with the certifying physician, especially for patients already experiencing PD-related psychosis or who are on antipsychotic medications.
16. Post-Traumatic Stress Disorder (PTSD)
PTSD has become one of the most commonly certified conditions in state medical marijuana programs. Pennsylvania’s inclusion reflects a meaningful body of evidence and a substantial population of veterans, first responders, assault survivors, and others who have found conventional treatments inadequate.
Research context: The endocannabinoid system plays a central role in fear extinction, the neural mechanism by which traumatic memories lose their emotional charge over time. Cannabis may facilitate this process and reduce the hyperarousal, nightmares, and intrusive symptoms that define PTSD. A 2014 study in the Journal of Psychoactive Drugs found self-reported improvements in PTSD symptom severity among medical cannabis users in New Mexico. A 2020 observational study in Journal of Affective Disorders found significant reductions in PTSD checklist scores with cannabis use. The VA maintains a nuanced position, acknowledging the need for research while noting that VA providers can discuss cannabis with veterans in states where it is legal.
Common targets for PTSD patients using cannabis: nightmares and sleep disruption, hyperarousal, anxiety, and emotional reactivity. Many PTSD patients report specific benefit from cannabis with sleep, a critical domain given how sleep disruption compounds other PTSD symptoms.
- Read More: Is Indica or Sativa Better for Sleep?
17. Severe Chronic or Intractable Pain of Neuropathic Origin; or Severe Chronic or Intractable Pain in Which Conventional Therapeutic Interventions Are Contraindicated or Have Been Ineffective
This is the broadest and most commonly cited qualifying condition in Pennsylvania’s program and it is written carefully. There are actually two distinct pathways within this single condition entry:
Pathway A: Severe chronic or intractable pain of neuropathic origin. This covers nerve-related pain specifically and does not require prior treatment failure, if the pain is neuropathic and severe/intractable, that meets the standard.
Pathway B: Severe chronic or intractable pain (of any type) where conventional therapeutic interventions are contraindicated or have been ineffective. This covers the broader universe of chronic pain conditions: musculoskeletal, fibromyalgia, chronic back and neck pain, complex regional pain syndrome, and others but requires that standard treatments have failed or cannot be used.
Research context: A landmark 2022 JAMA Network Open meta-analysis of 32 trials covering 5,174 patients found that cannabinoids showed a statistically significant advantage over placebo for chronic pain. A 2017 National Academies of Sciences, Engineering, and Medicine report concluded there was “substantial evidence” that cannabis is effective for chronic pain in adults, the highest certainty level they assigned to any cannabis finding.
The practical significance of the language here: patients with fibromyalgia, chronic back pain, or other non-neuropathic pain conditions qualify but only if they can document that conventional treatments have been tried and have not adequately controlled their pain. Your certifying physician will review your treatment history as part of the evaluation.
- Read More: Best Cannabis Strains for Nausea
18. Sickle Cell Anemia
Sickle cell disease produces episodes of severe vaso-occlusive pain crises, among the most acutely painful conditions in medicine, alongside chronic pain between crises, fatigue, organ complications, and stroke risk. Pain management in sickle cell is both critical and difficult, often under-treated due to stigma and the high opioid requirements some patients develop.
Research context: The American Society of Hematology’s 2020 guidelines for sickle cell pain management acknowledged cannabis as a consideration for chronic pain in adults. A 2020 survey study in Blood Advances found that cannabis use in sickle cell patients was associated with lower opioid use, fewer emergency department visits, and improvements in pain, sleep, and anxiety. A small randomized controlled trial (Abrams et al., 2020) found inhaled cannabis reduced pain in adults with sickle cell disease.
The opioid-sparing signal in sickle cell is particularly meaningful given the clinical complexity of managing opioid tolerance in this population over a lifetime of pain crises.
19. Neurodegenerative Diseases (Including Alzheimer’s Disease)
Pennsylvania’s neurodegenerative disease category is broader than just Alzheimer’s, it covers all neurodegenerative conditions, using Alzheimer’s as the leading example. This includes Parkinson’s disease (also separately listed), Lewy body dementia, frontotemporal dementia, progressive supranuclear palsy, and other degenerative neurological conditions.
Research context: The endocannabinoid system is involved in neuroprotection, neuroinflammation & neuroplasticity all relevant to neurodegenerative processes. For Alzheimer’s specifically, preclinical work has shown that cannabinoids may reduce amyloid beta aggregation and neuroinflammation. A 2019 randomized crossover trial published in Neuropsychopharmacology found cannabis oil did not significantly reduce behavioral symptoms in dementia patients (the primary outcome), though it was well tolerated. Survey and observational data more consistently show benefit for behavioral symptoms, agitation, appetite, sleep rather than cognitive outcomes.
The most honest position for dementia: cannabis evidence for behavioral symptoms (especially agitation and sleep) is more supportive than for cognitive preservation or slowing. The certifying physician conversation will focus on which specific symptoms the patient or their caregiver hopes cannabis will address.
20. Terminal Illness

A terminal diagnosis qualifies under Pennsylvania’s program when a licensed physician has determined the patient has a terminal condition with a life expectancy generally defined as six months or less if the disease runs its normal course (though physician judgment applies). This is deliberately broad any terminal diagnosis qualifies, not just cancer.
⚠️ Critical hospice note: If you are enrolled in Medicare-funded hospice, your hospice organization cannot certify you for medical marijuana, administer it, or include it in your care plan. Cannabis remains Schedule I under federal law, and Medicare-funded hospices risk their federal certification if they formally facilitate cannabis use. You must obtain your PA MMJ card independently, purchase cannabis products out of pocket from a licensed PA dispensary, and use them alongside (not through) your hospice program. This is frequently misunderstood and is the most important practical fact for terminally ill patients considering medical cannabis.
For obtaining a PA MMJ card when terminally ill: the telehealth evaluation is brief and can be facilitated by a family member or caregiver. Pennsylvania allows up to two designated caregivers per patient who can register with the program and make dispensary purchases on the patient’s behalf.
21. Dyskinetic and Spastic Movement Disorders
This category covers movement disorders characterized by abnormal involuntary movements (dyskinesia) or increased muscle tone and involuntary spasms (spasticity). It is intentionally broad and serves as a qualifying pathway for conditions including:
- Cerebral palsy (spastic and dyskinetic types)
- Dystonia
- Tardive dyskinesia (a movement disorder caused by prolonged antipsychotic use)
- Dyskinesias arising from Parkinson’s disease or its treatments
- Spastic paraplegia
- Other spastic conditions not covered under the CNS damage category
Research context: As with spasticity of MS origin, cannabis has meaningful evidence for movement disorder control. The THC component is generally thought to be the primary driver of antispastic effects, though the combined CBD:THC ratio may provide better tolerability. Sativex trials in MS spasticity, by showing reduction in both spasticity and spasm frequency, have established cannabinoids as a mechanistically validated option for this symptom class.
22. Opioid Use Disorder (Where Conventional Therapeutic Interventions Are Contraindicated or Ineffective, or as Adjunctive Therapy in Combination with Primary Therapeutic Interventions)

Pennsylvania added opioid use disorder (OUD) as a qualifying condition in 2018, making it one of the first states to formally recognize cannabis as a potential tool in addressing the opioid crisis. The condition language is nuanced and important: cannabis qualifies either as an adjunctive therapy (used alongside medications like buprenorphine or methadone) or when conventional interventions are contraindicated or ineffective.
This is not a replacement for evidence-based OUD treatment (MOUD – medications for opioid use disorder). Pennsylvania’s program recognizes cannabis as a potential component of a comprehensive OUD management approach, not as a standalone treatment.
Research context: An increasing body of evidence suggests that cannabis access is associated with reduced opioid use and opioid-related deaths at the population level. A frequently cited study in JAMA Internal Medicine (2014) found states with medical marijuana laws had significantly lower opioid overdose mortality rates. A 2019 study in PLOS ONE found that medical cannabis patients reported substituting cannabis for opioids with a high rate of success. These are largely observational findings and cannot establish causation but they have driven policy attention.
⚠️ Drug interaction note: CBD significantly inhibits CYP3A4 and CYP2D6 enzymes that metabolize methadone and buprenorphine. If you are on MOUD, discuss cannabis use explicitly with your prescribing physician, dose adjustments may be needed.
23. Anxiety Disorder
Anxiety disorder was added to Pennsylvania’s qualifying conditions list and represents one of the most significant expansions of the program, anxiety is among the most prevalent mental health conditions in the state and the country, and a large portion of PA MMJ patients are certified under this condition.
Research context: The relationship between cannabis and anxiety is more nuanced than most other qualifying conditions. At moderate, controlled doses, particularly CBD-dominant formulations and low-THC products, cannabis generally reduces anxiety. At higher doses and with high-THC products, cannabis can precipitate or worsen anxiety, including acute panic in susceptible individuals. This dose-dependent and product-dependent response is the single most important clinical consideration for anxiety patients choosing cannabis.
A 2015 review in Neurotherapeutics found preclinical and some clinical evidence supporting CBD specifically as an anxiolytic. A 2019 study in The Permanente Journal found CBD administration was associated with decreased anxiety scores in 79% of patients with primary anxiety complaints.
Product guidance matters: For anxiety, most clinicians experienced with medical cannabis recommend CBD-dominant formulations, starting at very low doses, and titrating slowly. High-THC products should be approached with particular caution by anxiety patients, especially those with panic disorder or social anxiety.
Read More:
24. Chronic Hepatitis C
Chronic hepatitis C is a viral infection causing persistent liver inflammation that can progress to cirrhosis, liver failure, and hepatocellular carcinoma. While direct-acting antiviral (DAA) therapies have transformed HCV treatment outcomes, a significant patient population has challenges with treatment, including side effects from therapy, treatment-related fatigue, pain, nausea, and patients in whom treatment is delayed or not yet initiated.
Research context: A 2006 study in the European Journal of Gastroenterology & Hepatology found that cannabis use was associated with improved adherence to interferon-ribavirin therapy, largely because it helped manage the significant nausea and appetite suppression caused by older regimens. With modern DAA therapies, the treatment burden is much lower than with interferon, but symptom management remains relevant for many patients, particularly those with advanced fibrosis or concurrent symptoms from liver disease.
Cannabis for liver disease carries a genuine complexity: some preclinical and observational data suggests heavy cannabis use may be associated with progression of liver fibrosis via CB1 receptor activation, though moderate use has not shown this pattern. This should be discussed openly with the certifying physician.
What Approved Forms of Medical Marijuana Are Available in Pennsylvania?
Pennsylvania’s Medical Marijuana Act specifies approved forms. These include:
- Oils and tinctures
- Pills and capsules (including tablets and gelcaps)
- Topical creams, ointments, and gels
- Vaporizable flower (dry leaf – for use in a vaporizer; smoking is prohibited)
- Liquids and solutions (including metered-dose inhalers)
- Patches
Edibles in the traditional sense (gummies, chocolates) are not approved. The current approved forms list is maintained on the PA DOH website at health.pa.gov.
How to Get Your Pennsylvania Medical Marijuana Card?
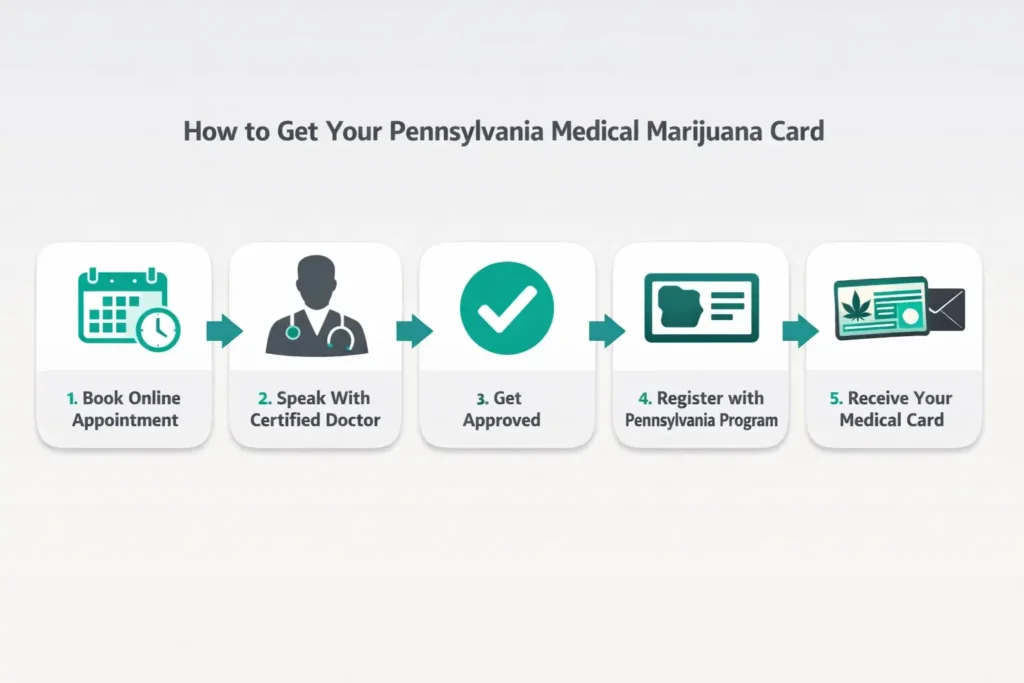
Step 1: Get a Physician Certification
Schedule a telehealth appointment with a physician registered with the PA DOH’s medical marijuana program. The physician will review your diagnosis, medical history, symptoms, and current medications. They do not prescribe marijuana, they issue a certification confirming you qualify.
Step 2: Register with the PA DOH Patient Registry
After your certification is issued, register at the PA Patient and Caregiver Registry https://padohmmp.custhelp.com/app/login. You’ll need:
- Your physician certification (electronically transmitted or uploaded)
- A valid Pennsylvania driver’s license or state ID
- Payment of the $50 annual fee (fee waivers available for patients on SNAP, Medicaid, or WIC – see below)
Step 3: Receive Your Card
Your temporary approval is issued immediately upon registration approval. Your physical card follows by mail.
Step 4: Visit a Licensed PA Dispensary
Use the PA DOH dispensary locator to find a licensed dispensary near you. Your dispensary pharmacist can advise on product selection for your specific condition and symptom profile.
Fee Reduction:
Pennsylvania offers a reduced registration fee for patients who demonstrate financial hardship. The DOH’s fee reduction application is available at the patient registry portal.
Caregiver Registration:
Patients who need assistance can designate up to two caregivers. Caregivers must register separately, submit to a background check, and pay a $25 fee. Caregivers may purchase and assist with cannabis on behalf of qualifying patients.
Learn more about becoming a Pennsylvania medical marijuana caregiver and the registration process.
- Source: PA DOH – Dispensary Locator
Frequently Asked Questions
Q: Can I qualify for more than one condition?
Q: Do I need records or documentation at the evaluation?
Q: Does my primary care doctor need to be involved?
Q: How long does Pennsylvania registration take?
Q: Is medical marijuana covered by insurance in Pennsylvania?
Official Pennsylvania Medical Marijuana Program Resources
- PA DOH Medical Marijuana Program (main page): health.pa.gov – Medical Marijuana
- PA Qualifying Conditions (official list)
- PA Medical Marijuana Act (Act 16 of 2016, as amended): PA General Assembly – Act 16
- PA Patient & Caregiver Registration Portal
- PA DOH Dispensary Locator: PA DOH – Dispensaries
- PA DOH – Approved Forms of Medical Marijuana: PA DOH – Patients
- PA Medical Marijuana Advisory Board: PA DOH – Advisory Board
NOTE: “Medical cannabis is not a cure for any of the conditions listed above. This page provides general information about Pennsylvania’s qualifying conditions and is not a substitute for medical advice from a licensed physician. Always disclose cannabis use to your treating physicians, particularly regarding potential interactions with prescribed medications.“