
When Pennsylvania passed its Medical Marijuana Act in 2016, it made history by becoming the first state in the country to explicitly list autism spectrum disorder as a qualifying condition for all ages, not just adults, not just severe cases. That decision reflected something the research community had been observing for years: that the endocannabinoid system appears to play a meaningful role in the neurological underpinnings of ASD, and that cannabis particularly CBD-dominant formulations shows genuine promise for some of the symptoms that make everyday life most difficult for autistic people and their families.
This page explains who qualifies, what the science actually says, what parents of autistic minors need to know about the caregiver pathway, and how to start the certification process in Pennsylvania.
Does Autism Qualify for Medical Marijuana in Pennsylvania?
Yes. Autism spectrum disorder (ASD) is an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016) and is recognized by the Pennsylvania Department of Health (DOH) for patients of all ages. There is no age floor, both minors and adults with a confirmed ASD diagnosis are eligible. For minors, a parent or legal guardian must register as the patient’s designated caregiver.
There is no requirement that ASD be severe to qualify. The condition itself is qualifying. That said, the certifying physician will discuss which specific symptoms cannabis is intended to address, and that conversation shapes appropriate product recommendations.
Pennsylvania was the first state to include autism as an explicit qualifying condition for patients of all ages, a distinction worth understanding. Many other states have since added ASD, but several limit it to severe presentations or adult patients only. Pennsylvania’s law is deliberately inclusive.
What Is Autism Spectrum Disorder?
Autism spectrum disorder is a neurodevelopmental condition defined by persistent differences in social communication and interaction, alongside restricted or repetitive patterns of behavior or sensory responses. The word “spectrum” matters, ASD presents across an enormous range, from minimally verbal individuals with significant support needs to highly verbal adults who may have gone undiagnosed for decades.
According to the CDC, approximately 1 in 31 children in the United States has been identified with ASD as of the most recent surveillance data. ASD is diagnosed roughly four times more often in boys than girls, though research increasingly suggests girls are underdiagnosed due to different presentation patterns.
There is no cure for ASD and no single medication that addresses its core features. Standard clinical management targets associated symptoms: anxiety, behavioral dysregulation, sleep disruption, attention difficulties, mood instability, seizures in some patients through a combination of behavioral therapies, occupational therapy, speech and language therapy, and when needed, psychiatric medications. That last category is where many families hit a wall: the psychiatric medications commonly used for ASD-associated behaviors carry significant side effect profiles, particularly in children, and many families find them inadequate or intolerable.
Medical cannabis has entered this conversation largely because of two things: a growing body of clinical research showing benefits for ASD-specific symptoms, and the fact that CBD, the primary cannabinoid of interest in pediatric ASD research, does not produce intoxication at therapeutic doses.
- Source: NIH – Autism Spectrum Disorder
Why Cannabis Is Scientifically Relevant to ASD?
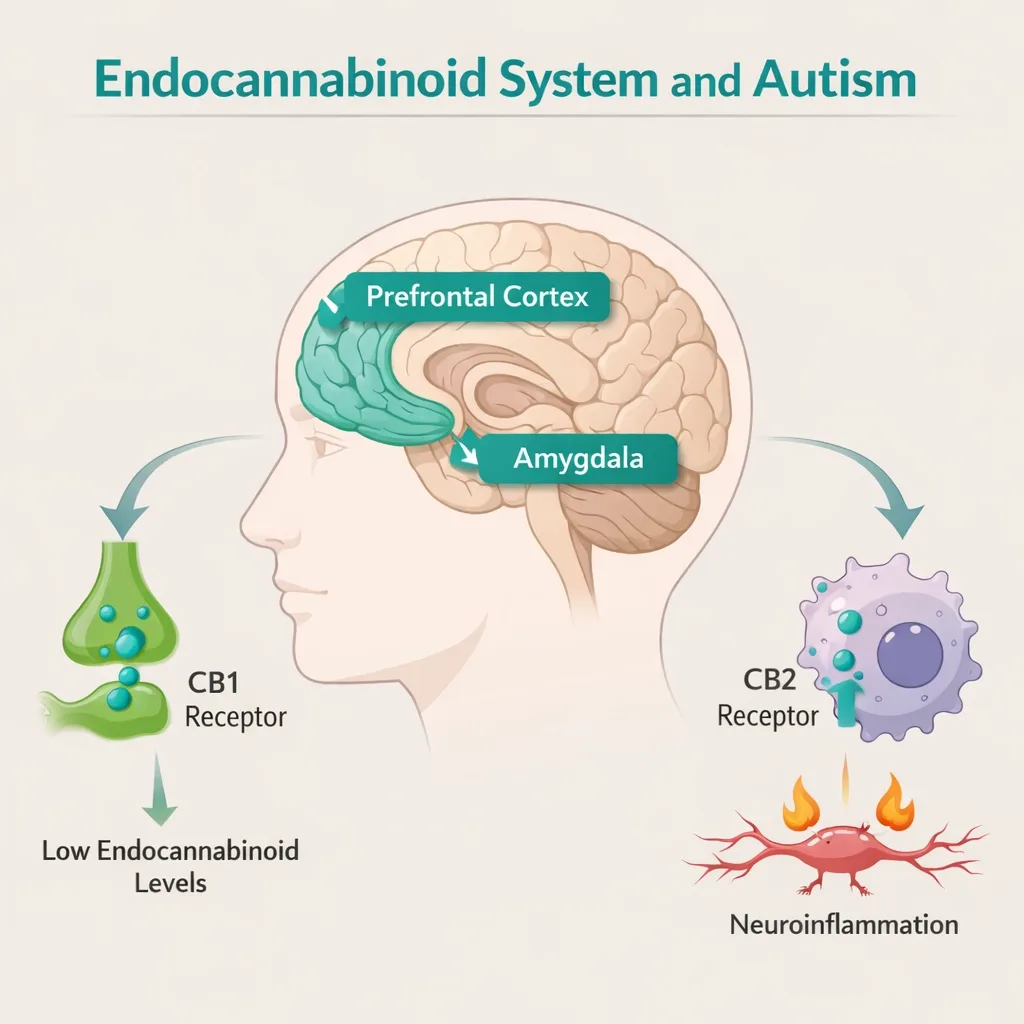
The starting point for understanding cannabis and ASD is the endocannabinoid system (ECS), a signaling network in the brain that helps regulate mood, social behavior, anxiety, sleep, and sensory processing. CB1 and CB2 receptors, the ECS’s primary targets, are distributed throughout regions of the brain relevant to ASD.
Research published in 2013 by Stanford University researchers found that many ASD symptoms are associated with a gene mutation that blocks natural endocannabinoid production and disrupts how cannabinoids interact with the brain. A separate 2013 study in the Journal of Autism and Developmental Disorders found that immune dysfunction, a contributing factor in some forms of ASD — can arise from complications within the endocannabinoid system. Studies in children with ASD have since found measurably lower endocannabinoid levels compared to neurotypical children.
A 2025 systematic review in PMC synthesizing the research literature describes the ECS as directly implicated in ASD through its role in neurotransmitter modulation and neuroinflammation, two processes that are consistently disrupted in ASD neurobiology.
What this means practically: cannabis is not a general anti-anxiety or sedative being tried on ASD by coincidence. There is a disease-specific neurobiological argument for why the endocannabinoid system is relevant to ASD symptoms, which is one reason Pennsylvania included it from the beginning.
What the Clinical Research Actually Shows?
The ASD cannabis evidence base has grown substantially over the past five years. What follows is an honest account of what the best studies found, including where results were mixed or limited.
The 2025 Meta-Analysis (276 Patients, Three RCTs)
One of the most rigorous recent summaries of the ASD cannabis literature is a 2025 meta-analysis presented at the European Psychiatry congress, drawing from three randomized, placebo-controlled trials covering 276 participants with a mean age of 10.5 years (ranging from 5 to 21). CBD extract was titrated from 1 mg/kg/day up to 10 mg/kg/day.
The results were statistically significant across three key domains: CBD-rich extracts significantly improved social responsiveness, reduced disruptive behavior, and alleviated anxiety compared to placebo. This is the strongest controlled-trial evidence to date that CBD-rich cannabis extracts produce measurable, replicable benefits for ASD-associated symptoms.
The 2024 Brazilian RCT (60 Children, Double-Blind, Placebo-Controlled)
A randomized, double-blind, placebo-controlled trial published in Trends in Psychiatry and Psychotherapy (da Silva Junior et al., 2024) enrolled 60 children aged 5 to 11 with ASD and randomized them to 12 weeks of CBD-rich cannabis extract or placebo.
Statistically significant improvements were found in social interaction, anxiety, psychomotor agitation, number of meals per day, and concentration (the last specifically in mild ASD cases). Only three children in the treatment group experienced adverse effects — dizziness, insomnia, colic, and weight gain, all mild and transient. The researchers concluded that CBD-rich cannabis extract improved social interaction (one of ASD’s core diagnostic features), as well as anxiety and behavioral symptoms, with a favorable safety profile.
The Aran et al. Israeli Studies – 188 Patients, Real-World Data
Among the most widely cited ASD cannabis research comes from Dr. Aran’s group in Israel, which has produced multiple analyses of real-world medical cannabis use in autistic children. A 2019 Scientific Reports study followed 188 ASD patients treated with cannabis oil (30% CBD, 1.5% THC) over six months.
After treatment, 30.1% of patients reported significant improvement, 53.7% moderate improvement, and 6.4% slight improvement — meaning roughly 83% of patients reported at least some benefit. Behavioral outbreaks improved in 61% of patients, communication problems in 47%, anxiety in 39%, stress in 33%, and disruptive behavior in 33%.
A subsequent randomized, controlled proof-of-concept trial by the same group found whole-plant cannabis reduced behavioral problems and improved autism-related parental stress scores meaningfully compared to baseline.
The 2026 Crossover RCT (29 Children, Autism Research Journal)
A 2026 randomized, double-blind, placebo-controlled crossover trial published in Autism Research (Parrella et al.) tested CBD oil with terpenes at 10 mg/kg/day in 29 autistic children aged 5–12 over two 12-week periods. While the primary outcome of overall social responsiveness did not reach statistical significance, CBD led to meaningful improvements in specific social behaviors, reduced anxiety, and reduced parental stress. Only two children experienced mild gastrointestinal discomfort. The authors described these as signals warranting larger trials.
The 2025 Springer RCT – Where CBD Did Not Separate from Placebo
An important counterbalance: A 2025 double-blind, placebo-controlled crossover trial published in the Journal of Autism and Developmental Disorders (Springer) tested pharmaceutical-grade CBD (Epidiolex, up to 20 mg/kg/day) for severe problem behaviors, repetitive behavior and overall behavior by CBCL and RBS-R scales — in autistic boys aged 7–14. Both groups improved on the primary behavioral outcome measures, but there was no statistically significant difference between CBD and placebo.
This result is important and should not be minimized. Repetitive behaviors and the primary composite behavioral scales did not show a CBD advantage over placebo in this particular trial. The null result likely reflects a combination of factors, the specific outcome measures used, the patient population (boys with severe behavior problems rather than the broader ASD spectrum), and the high placebo response rate common in pediatric behavioral trials.
The honest picture from the totality of evidence: CBD-rich cannabis shows the most consistent benefit for anxiety, behavioral outbursts, and specific social behaviors in ASD. Benefits for repetitive behaviors and broader behavioral composites are less consistently supported. Response varies meaningfully across individuals.
Symptom by Symptom: Where Cannabis May Help ASD Patients

Anxiety
This is the area with the strongest and most consistent evidence across the ASD cannabis literature. Anxiety is also among the most prevalent and debilitating ASD comorbidities, estimates suggest 40–60% of autistic individuals have clinically significant anxiety. The 2025 meta-analysis, the 2024 Brazilian RCT, the 2026 crossover trial, and multiple observational studies all found statistically significant anxiety reductions with CBD-rich formulations. CBD interacts with serotonin 5-HT1A receptors, the same receptors targeted by SSRIs, which is one likely mechanism for the anxiolytic effect.
For autistic adults in Pennsylvania who qualify primarily through anxiety, it is worth noting that anxiety disorder is also a separate qualifying condition in Pennsylvania’s program. Discuss with your certifying physician which condition best describes your clinical picture.
Behavioral Outbursts, Agitation, and Irritability
Behavioral dysregulation: Meltdowns, emotional outbursts, aggression toward others, is one of the most treatment-resistant and family-affecting aspects of ASD. The Aran et al. Israeli data found behavioral outbreak improvement in 61% of patients. The 2025 meta-analysis found statistically significant reductions in disruptive behavior. This appears to be one of the more consistent areas of benefit across studies.
Self-Injurious Behavior
Self-injurious behavior (SIB): Hitting, biting, or scratching oneself, is among the most serious behavioral features of severe ASD and is among the hardest to manage with standard medications. Multiple observational studies and case reports have noted improvements in SIB with cannabis. The mechanisms likely overlap with behavioral dysregulation more broadly, though formal RCT evidence specifically for SIB remains limited.
Sleep
Sleep disruption affects 40–80% of autistic individuals across the lifespan and is a major driver of daytime behavioral problems. The Aran et al. 2020 study of 150 pediatric ASD patients reported improvements in sleep. The 2025 systematic review found modest but consistent sleep benefits with CBD-rich formulations. Short-term, CBD at lower doses tends to improve sleep quality, particularly by reducing the anxiety and hyperarousal that prevent settling at night. Higher-dose THC can paradoxically disrupt sleep architecture, so product and dose selection matters particularly for children.
Social Interaction and Communication
This is the most contested area and the one where hope must be most carefully calibrated. The 2024 Brazilian RCT found a statistically significant improvement in social interaction. The 2025 meta-analysis found improvement in social responsiveness. The 2026 crossover trial showed improvements in specific social behaviors but not the primary social responsiveness composite score.
The 2025 Springer RCT found no advantage over placebo on behavioral composites. Social communication is a core diagnostic feature of ASD, not a downstream symptom and the evidence that cannabis modifies it meaningfully and reliably is not yet established. These improvements, when they appear, may reflect secondary effects of reduced anxiety rather than direct effects on social cognition.
Sensory Sensitivities
Sensory processing differences: Hypersensitivity to sound, light, texture, or proprioceptive input, affect a large proportion of autistic people and can be enormously disabling. This is an area where formal clinical data is sparse, but patient and caregiver reports of benefit are common. The mechanisms are plausible: the endocannabinoid system regulates sensory gating and pain processing, and CBD modulates TRPV1 channels involved in sensory signaling.
Concentration and Attention
The 2024 Brazilian RCT found significant improvements in concentration specifically in mild ASD cases. Attention difficulties and ADHD-like features are common ASD comorbidities. This is an area where results are likely to vary substantially across individuals, and where THC-containing products may worsen attention in some patients while CBD-dominant formulations may be more consistently beneficial.
Adults With ASD: A Different Clinical Conversation
Most of the clinical research involves children, which reflects both the urgency of pediatric ASD management and the larger pediatric ASD patient population engaging with medical cannabis. But autistic adults are a significant and growing group, including many who received their diagnosis in adulthood after years of misdiagnosis and their needs and risk profile are different.
For autistic adults in Pennsylvania:
- All of the same qualifying pathway applies: ASD diagnosis plus physician certification
- Adults manage their own registration without requiring a caregiver
- For adults whose most debilitating symptom is anxiety, the “anxiety disorder” qualifying condition may also apply, it is worth discussing which designation best reflects your case with the certifying physician
- The risk of cannabis worsening anxiety or triggering paranoia is real for some autistic adults, particularly with high-THC products. CBD-dominant formulations are generally recommended as a starting point
- Adults with concurrent ADHD features, which is common in ASD, should approach high-THC products with particular caution, as THC can worsen attention and executive function in some individuals
A 2025 Scientific Reports study assessed acute cannabis effects in autistic adults and found perceived reductions in symptoms associated with ASD that aligned with pediatric clinical trial results, including anxiety and behavioral features, supporting the relevance of this research to adult patients.
The Minor Patient Pathway: What Parents Need to Know?
Because Pennsylvania allows autistic minors to qualify, and because much of the research base involves pediatric populations, it’s worth being direct about what the process looks like when the patient is a child.
A parent or legal guardian must serve as the patient’s designated caregiver. The minor cannot register independently. The caregiver registers with the PA Medical Marijuana Program, handles all dispensary purchases, and manages product administration. A second designated caregiver can also be registered.
The certifying physician must be willing to certify a minor. Not all PA-registered medical marijuana physicians are comfortable certifying pediatric patients. When scheduling an evaluation for a minor patient, confirm that the practice sees minors before booking.
Documentation is important. The certifying physician will want to see confirmation of the ASD diagnosis, a diagnostic evaluation, developmental pediatrician records, or records from the treating psychiatrist. The physician should also know what behavioral or pharmacological treatments have already been tried and what their outcomes were.
The CHOP PolicyLab perspective: Researchers at Children’s Hospital of Philadelphia completed a natural history study of medical cannabis in autistic youth in Pennsylvania specifically. They found that parents were drawn to cannabis primarily because they perceived it as more natural with fewer side effects compared to standard psychiatric medications — views often rooted in their own experience with cannabis, and reinforced by awareness of FDA-approved Epidiolex for pediatric epilepsy. They called for more rigorous research specifically in the pediatric ASD population to close the gap between parental enthusiasm and clinical evidence.
Product selection for minors: CBD-dominant formulations, oils and tinctures are the standard approach for pediatric ASD patients. Weight-based dosing is typical in clinical research (1–10 mg/kg/day CBD). High-THC products are generally not appropriate for minors. The dispensary pharmacist should be told explicitly that the product is for a pediatric ASD patient so they can advise on the most appropriate formulations available in their inventory.
- Source: CHOP PolicyLab – Autistic Youth and Their Parents Are Excited About Medical Cannabis, But Clinicians Need More Research
- Source: PA DOH – Patient and Caregiver Registration
Drug Interactions: What Families and Caregivers Should Know?
Many autistic individuals, particularly those with moderate to severe presentations, take medications for behavioral management, anxiety, mood, or seizures. CBD can interact with several of these in clinically significant ways.
Antiepileptic drugs (AEDs)
A significant proportion of ASD patients also have epilepsy. CBD is known to interact with clobazam (elevating active metabolites, which can increase sedation) and valproic acid, among others. If an ASD patient is on any antiepileptic medication, this must be discussed explicitly with the prescribing neurologist before starting cannabis.
Antipsychotics (risperidone, aripiprazole)
These are the two FDA-approved medications for ASD-associated irritability and the most commonly prescribed in this population. CBD inhibits CYP3A4 and CYP2D6 enzymes that metabolize both. This can increase plasma levels of these medications, potentially increasing side effects including sedation, weight gain, and metabolic effects. Monitoring and possible dose adjustments may be needed.
SSRIs and SNRIs
Commonly used for anxiety in ASD. CBD also inhibits CYP2C19, which metabolizes several SSRIs. Plasma level increases are possible. This interaction is generally manageable with monitoring rather than being a contraindication to cannabis use.
Stimulants (methylphenidate, amphetamines)
Used for ADHD features in ASD. THC can reduce the efficacy of stimulants and worsen attention and executive function. CBD at lower doses generally does not have this interaction. For ASD patients on stimulants, CBD-dominant formulations are preferable.
Always bring a complete medication list to the physician certification appointment. The certifying physician will review interactions as part of the evaluation.
How to Get a Pennsylvania Medical Marijuana Card for Autism?
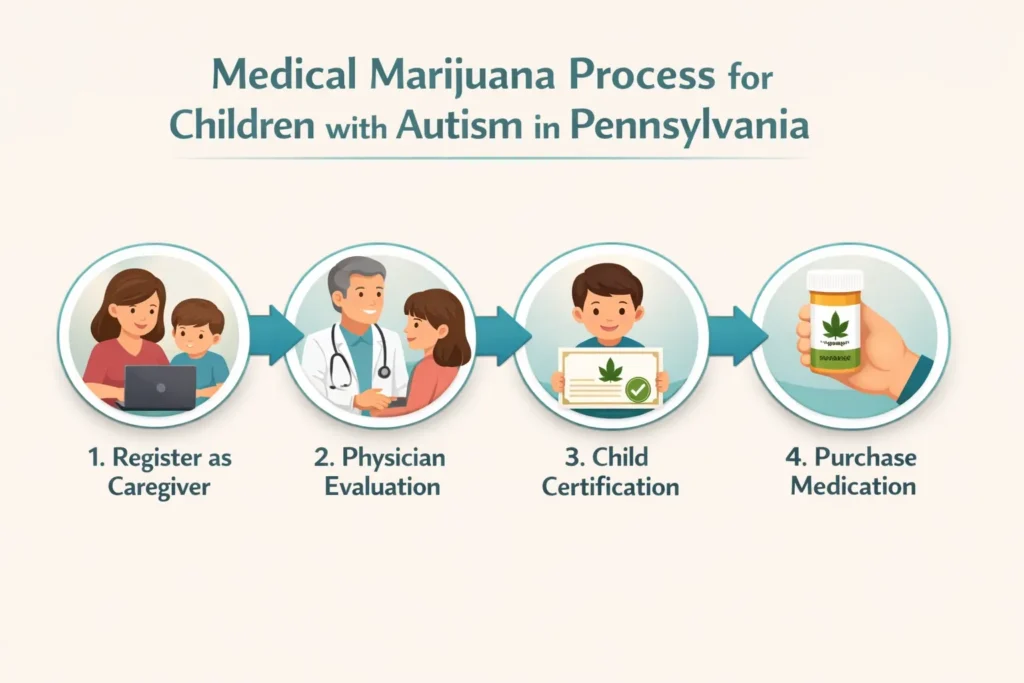
Step 1 — Physician Certification (Telehealth)
Schedule a telehealth appointment with a PA DOH-registered medical marijuana physician. For adult patients, this is a standard 10–15 minute evaluation. For minors, confirm the practice sees pediatric patients when scheduling. The physician will review the ASD diagnosis, symptom profile, current medications, and what has been tried previously. Have any available documentation of the ASD diagnosis ready.
Step 2 — State Registration
After the certification is issued, register at the PA Medical Marijuana Program Patient Registry at patientportal.mmapinc.com. You’ll need the physician certification, a valid Pennsylvania driver’s license or state-issued ID, and the $50 annual fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 3 — Caregiver Registration (Required for Minors; Optional for Adults)
For minor patients, the parent or guardian registers as the designated caregiver at the same portal. Caregivers must be 21 or older, pass a criminal history background check, and pay a $25 fee. Caregivers can purchase cannabis at any licensed PA dispensary on the patient’s behalf.
Step 4 — Visit a Licensed PA Dispensary
Use the PA DOH dispensary locator to find a licensed dispensary. Tell the dispensary pharmacist that the patient has ASD and describe the target symptoms, the pharmacist can recommend appropriate CBD-dominant formulations and advise on starting doses. For pediatric patients, emphasize that the product is for a child so dosing guidance is appropriately conservative.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
Frequently Asked Questions
Q: My child has ASD but it’s considered mild. Do they still qualify?
Q: What age can a child get a PA MMJ card for autism?
Q: Can an autistic adult get certified without a specialist diagnosis?
Q: Will THC make autism symptoms worse?
Q: Does cannabis help autistic children learn or develop?
Q: Is medical cannabis covered by insurance for ASD patients in Pennsylvania?
Autism Support Resources in Pennsylvania
Autism Society of Greater Philadelphia (autismsocietyphila.org) provides resources, advocacy, and community connections for autistic individuals and families throughout the Philadelphia region.
Autism Society of America – Pennsylvania Chapter (autismsociety.org) offers statewide resources, support groups, and guidance on navigating services.
Autism Speaks (autismspeaks.org) maintains a resource guide and 100 Day Kit for newly diagnosed families, as well as a tool kit specifically for navigating school-age services in Pennsylvania.
Children’s Hospital of Philadelphia (CHOP) – Center for Autism Research (carautismroadmap.org) provides research-backed guidance on autism treatment options including emerging therapies, and is the source of the PolicyLab analysis of medical cannabis in PA autistic youth referenced above.
NOTE: Medical marijuana is not a cure for autism and is not a replacement for behavioral therapy, educational supports, or evidence-based clinical care. What it can be, for the right patient and the right symptoms — particularly anxiety, behavioral outbursts, and sleep disruption — is a meaningful addition to a care plan where other options have fallen short. Pennsylvania’s program was designed to include exactly this population, and the research base supporting it has grown substantially since the law was signed.
If you are ready to begin the evaluation process, a PA-registered physician can complete the certification by telehealth. For families with a minor patient, the caregiver pathway is fully accommodated within the program.