
🎬 Watch This First — ALS Patients in Pennsylvania Are Using This Legal Option for Pain & Relief
If you or someone you love has been diagnosed with ALS, you already know that treatment options are limited. The two FDA-approved medications — riluzole and edaravone — slow progression modestly in some patients but do not stop the disease. What they cannot do, at least not adequately for most people, is manage the full burden of symptoms that ALS brings: the muscle cramps and spasticity, the unrelenting pain, the appetite collapse, the anxiety of watching your own body change.
Medical cannabis cannot cure ALS either. What it can do, for the right patient and the right symptoms, is provide meaningful relief where conventional options fall short.
In Pennsylvania, ALS is a qualifying condition under the Medical Marijuana Act. This page explains exactly what that means, what the research genuinely shows (including where it’s honest about limits), and what the practical path to a PA medical marijuana card looks like for ALS patients and their caregivers.
Does ALS Qualify for Medical Marijuana in Pennsylvania?
Yes. Amyotrophic lateral sclerosis (ALS) is explicitly named as a qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016). It is listed among the 24 approved serious medical conditions recognized by the Pennsylvania Department of Health (DOH).
To qualify, you must have a confirmed ALS diagnosis and receive certification from a physician registered with the PA DOH’s medical marijuana program. There is no requirement that your ALS neurologist be the certifying physician — any DOH-registered physician who has a continuing care relationship with you and is familiar with your diagnosis can certify you.
One additional point worth knowing: If your ALS has advanced to the point where your physician has documented a terminal prognosis, you may also qualify under Pennsylvania’s terminal illness qualifying condition. A certifying physician can list both ALS and terminal illness on a single certification, which is worth discussing if applicable to your situation.
- Official source: Pennsylvania Department of Health – Medical Marijuana Program
Understanding ALS: What the Disease Actually Does?
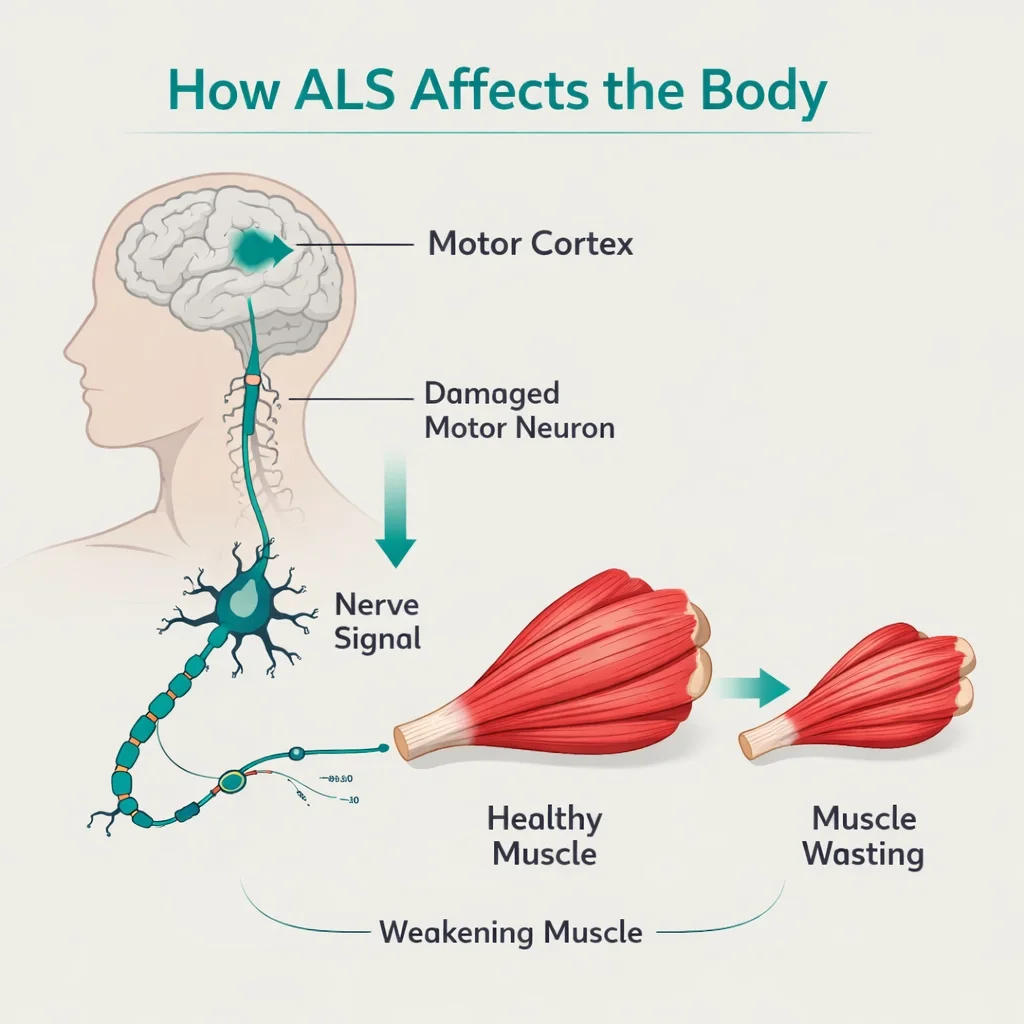
ALS — amyotrophic lateral sclerosis, also called Lou Gehrig’s disease — is a progressive neurodegenerative disease that destroys the motor neurons controlling voluntary muscle movement. Over time, the brain loses its ability to initiate and control muscle activity, and the muscles waste away.
According to the National Institute of Neurological Disorders and Stroke (NINDS), most ALS patients live two to five years after symptom onset, though approximately 10% live ten years or more. The disease most commonly appears between ages 40 and 70, affects men slightly more than women, and has no known cure.
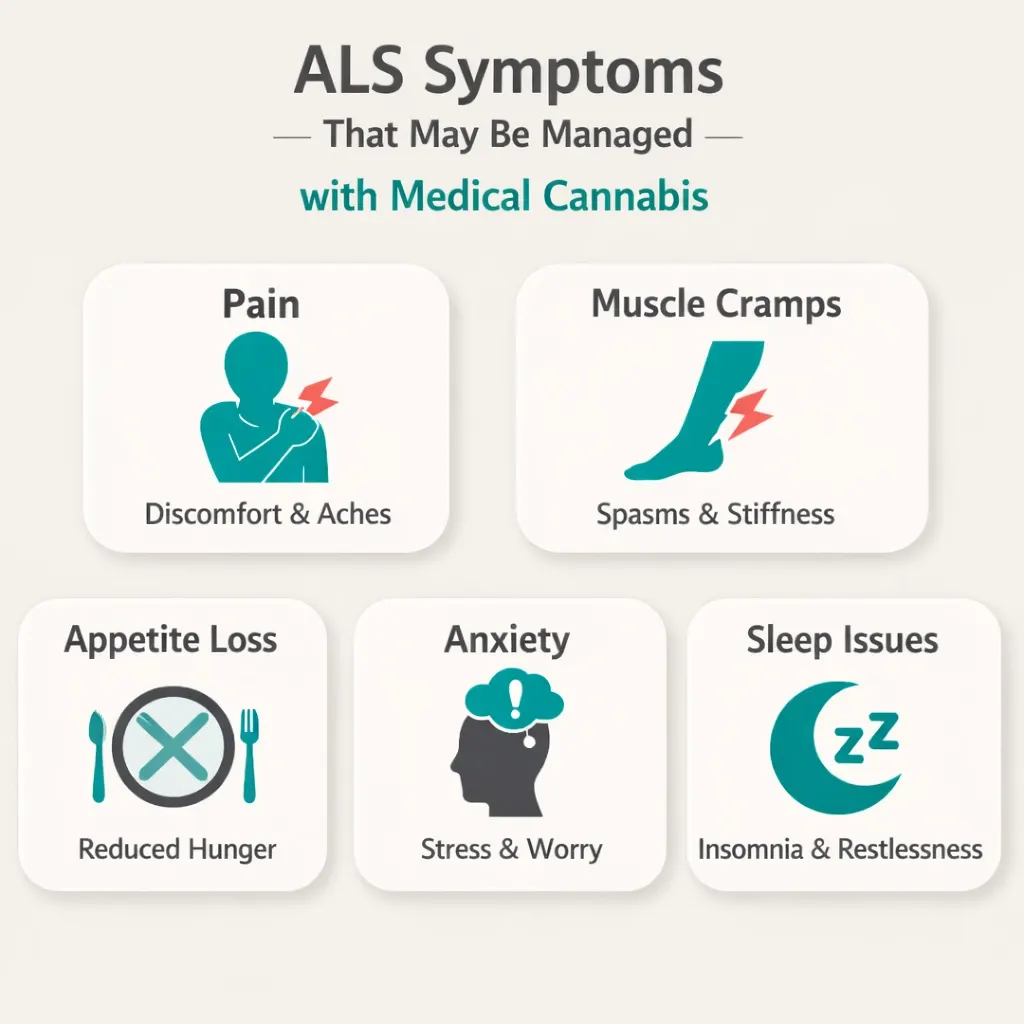
The symptoms ALS patients carry throughout the disease course — and the ones that medical cannabis most directly addresses — include:
- Muscle cramps and fasciculations (involuntary twitching) in the early and middle stages
- Spasticity — painful muscle stiffness and tightness, occurring in roughly one-third of ALS patients
- Pain arising from immobility, muscle strain on joints, muscle spasms, and positioning pressure
- Appetite loss and weight loss (cachexia) — a serious complication that worsens prognosis
- Drooling (sialorrhea) caused by weakening of the muscles that control swallowing
- Sleep disruption from discomfort, breathing difficulties, or anxiety
- Anxiety and depression — natural responses to a devastating diagnosis that also have direct neurological components
Standard ALS care manages these symptoms through a combination of medications, respiratory support, nutritional support, and palliative care. Many patients find the symptom burden imperfectly controlled despite optimal conventional management, which is the clinical context in which medical cannabis becomes relevant.
- Source: ALS Association – What is ALS?
Why Cannabis Is Scientifically Relevant to ALS?
Before getting to the clinical studies, it helps to understand why medical cannabis is mechanistically plausible for ALS — not just as a general symptom reliever, but as a compound with potential relevance to the disease itself.
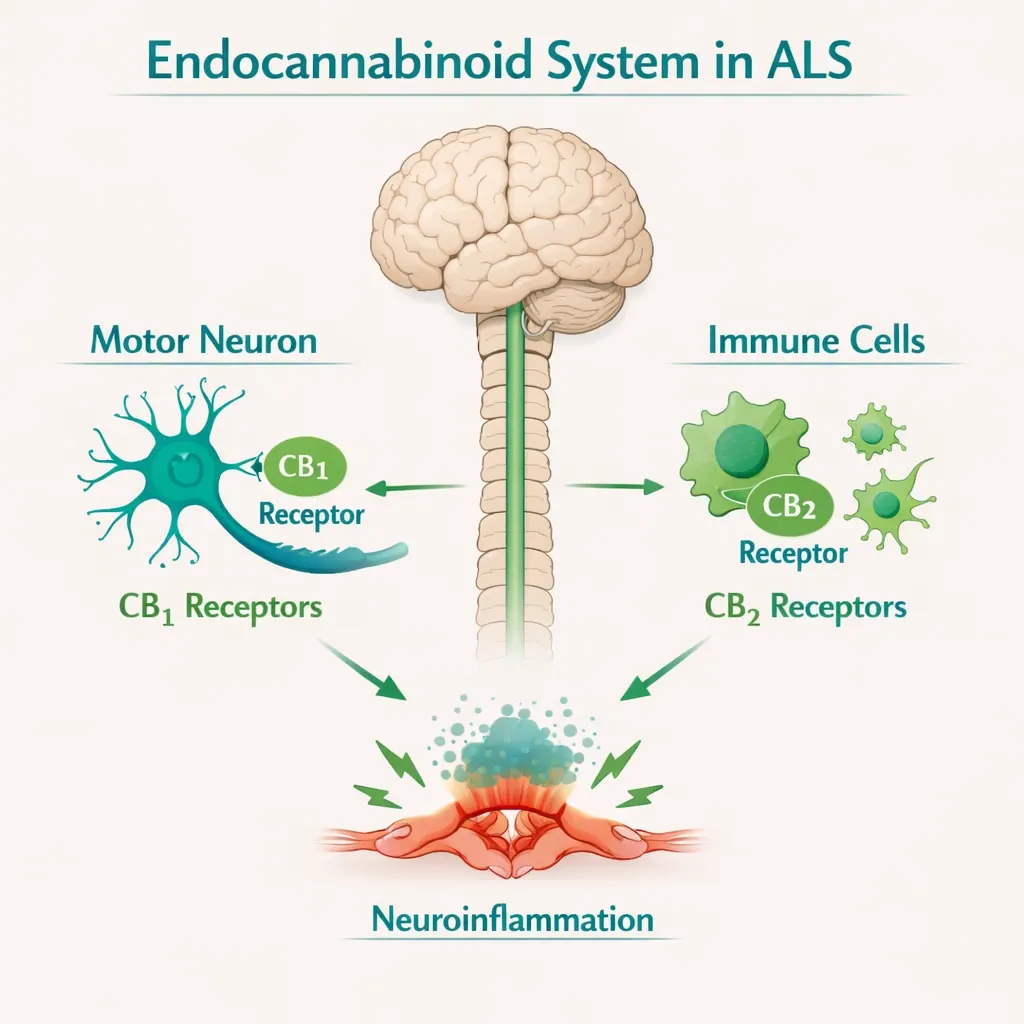
The endocannabinoid system (ECS) is a signaling network throughout the brain and spinal cord. CB1 receptors are concentrated in motor neurons — exactly the cells ALS destroys. CB2 receptors, meanwhile, are found predominantly in immune and glial cells and are significantly upregulated in ALS spinal cord tissue, a pattern that suggests the ECS is responding to the neuroinflammatory processes driving the disease.
Preclinical research has explored this relationship directly. Studies in ALS mouse models (SOD1 transgenic mice, the standard ALS animal model) have found that cannabinoid administration delayed motor neuron loss, reduced oxidative damage in spinal cord cultures, and in some models slowed disease onset. These findings do not translate directly to humans — preclinical results in ALS models have a poor track record of predicting human outcomes — but they establish a neurobiological rationale that isn’t present for every condition on Pennsylvania’s qualifying list.
A 2016 review in Neural Regeneration Research (Giacoppo & Mazzon) described the ECS as “a potential target for the treatment of ALS,” citing the antioxidant, anti-inflammatory, and neuroprotective properties of cannabinoids observed in preclinical settings.
The practical significance: for ALS patients, cannabis isn’t just palliative by general analogy. There is a disease-specific scientific argument for investigating it — which is part of why ALS appeared on so many of the earliest state medical marijuana qualifying lists.
What the Clinical Research Actually Shows
This is the section that matters most for an ALS patient trying to make an informed decision. Here is an honest account of what the evidence shows — including where it falls short.
The 2024 UTHSCSA Retrospective Study (344 Patients) — The Most Current Evidence
The most rigorous ALS-specific medical marijuana dataset published to date comes from a 2024 retrospective cohort study in the Journal of Neurological Sciences, conducted at the University of Texas Health Science Center San Antonio’s ALS Association Certified Treatment Center. Researchers reviewed charts of 344 ALS patients treated over a two-year period and compared outcomes between those who used medical marijuana and those who did not.
The findings were nuanced — and more honest than most cannabis research:
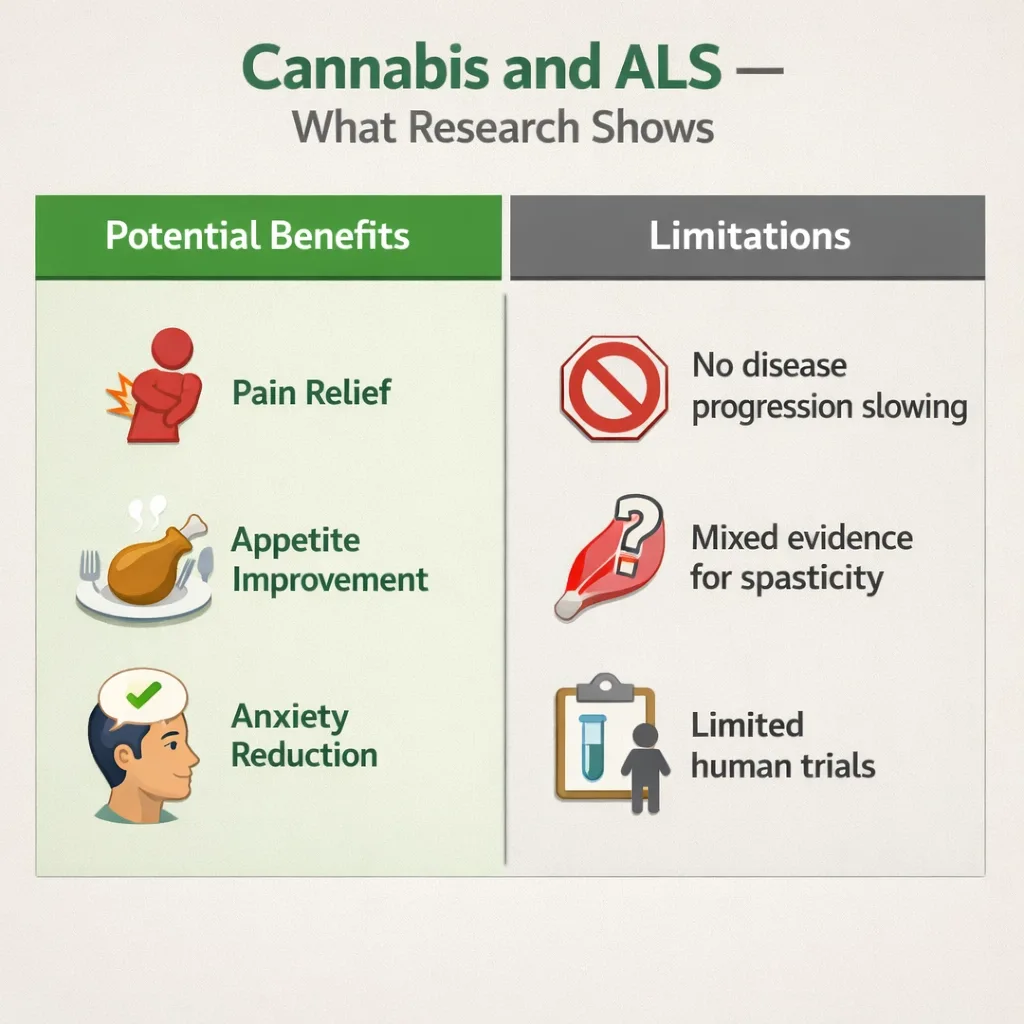
- Medical marijuana use correlated with short-term improvement in pain, poor appetite, and anxiety
- Medical marijuana use did not correlate with improvement in spasticity or insomnia in this dataset
- There was no significant correlation between medical marijuana use and maintenance of BMI
- Medical marijuana use appeared to correlate with faster ALSFRS-R progression — but the researchers noted that patients using cannabis had higher symptom burden and were already progressing faster before starting cannabis, suggesting selection bias rather than a causal relationship
The study’s authors called for a multi-center randomized controlled trial and concluded that cannabis “shows correlation with managing pain, poor appetite, and short-term anxiety in ALS.”
This is important information. Earlier, smaller studies and patient surveys showed broader symptom benefits (including spasticity). This larger, more rigorous dataset tempers those findings — at least for spasticity, where the evidence is not as strong as many ALS resources suggest.
The 2023 French Patient Survey — Real-World Experience
A 2023 survey published in Revue Neurologique (Lacroix et al.) surveyed 129 ALS patients in France, of whom 28 (21.7%) reported cannabis use. This was the first large-scale survey of real-world cannabis use specifically in ALS patients.
Patients reported benefits on both motor and non-motor symptoms, including muscle rigidity and cramps, pain, sleep quality, emotional state, depression, and overall quality of life. Only eight patients reported minor adverse reactions — drowsiness, euphoria, and dry mouth. The researchers called for further research and noted the urgent need to bring cannabis use into formal medical pathways for ALS patients.
The Nabiximols ALS Spasticity Trial
A dedicated clinical trial in ALS patients found that six weeks of treatment with nabiximols (the 1:1 THC:CBD oromucosal spray Sativex, approved for MS-related spasticity in many countries outside the US) improved spasticity scores compared to placebo, in which spasticity worsened. A small German study also found high patient satisfaction with THC/CBD combination for mild to moderate ALS-related spasticity.
This is worth noting because it runs somewhat counter to the 2024 UTHSCSA retrospective finding of no significant spasticity benefit — illustrating that the evidence for spasticity is genuinely mixed and may depend on product, dosing, and patient selection.
Earlier Survey Data
A frequently cited 2004 paper in the American Journal of Hospice and Palliative Care (Carter et al.) surveyed ALS patients and found cannabis beneficial for managing appetite loss, depression, pain, spasticity, and drooling. A 2014 survey presented at the American Academy of Neurology annual meeting (Kaufman et al.) found ALS patients reported preferring cannabis to prescription medications for several symptoms. These older surveys established the initial evidence base that convinced states to list ALS as a qualifying condition — and while they lack the rigor of the 2024 cohort study, their consistent direction matters.
Symptom by Symptom: Where Cannabis May Help ALS Patients
Given the overall evidence picture, here is a realistic assessment by symptom:
Pain
The clearest area of benefit in the current evidence base. Pain in ALS arises from multiple sources — muscle spasms and fasciculations, strain on joints from postural changes, skin and pressure discomfort from immobility, and neuropathic components. The 2024 UTHSCSA study found a statistically significant correlation between medical marijuana use and pain reduction. THC is the primary analgesic cannabinoid; balanced THC:CBD formulations are commonly recommended for pain with better tolerability.
Appetite and Weight Loss
Appetite loss and the resulting cachexia are serious complications in ALS. The 2024 study found a positive correlation between cannabis use and short-term appetite improvement, though not with BMI maintenance. THC’s appetite-stimulating properties are well-documented — this is one of the most reliable effects of THC across multiple disease populations. Tinctures and oral products may be more practical than inhaled formulations for ALS patients with respiratory involvement.
Anxiety and Mood
The anxiety of an ALS diagnosis — and of watching the disease progress — is profound. The 2024 study confirmed a positive correlation between cannabis and short-term anxiety reduction. CBD-dominant formulations are generally preferred for anxiety because high-THC products can worsen anxiety in some patients. For ALS patients who are managing depression alongside anxiety, this is an area where cannabis may provide genuine quality-of-life benefit.
Spasticity
The evidence here is genuinely mixed. The nabiximols ALS trial and several surveys show benefit. The 2024 UTHSCSA retrospective did not find a significant correlation with spasticity reduction. This may reflect differences in product, patient population, or measurement. The biological rationale is sound — cannabinoids have the most robust evidence base for spasticity in MS, and the neurological mechanisms overlap. For ALS patients with significant spasticity inadequately controlled by baclofen or tizanidine, a trial of cannabis is a reasonable clinical consideration, though expectations should be calibrated to the mixed evidence.
Drooling (Sialorrhea)
Excess saliva production is a distressing and practically debilitating symptom for many ALS patients. Cannabis has bronchodilatory and salivary-reducing properties — the anticholinergic component of cannabis reduces secretions. Survey data consistently lists drooling as one of the symptoms patients report improving with cannabis. Formal trial evidence specifically for ALS sialorrhea is lacking, but the mechanistic basis and patient reports support it as a reasonable symptom target.
Sleep
The 2024 retrospective did not find a significant correlation between cannabis and insomnia improvement in ALS patients. Earlier survey data reported sleep improvement. Sleep disruption in ALS has multiple drivers — pain, respiratory compromise, anxiety, and positioning — and cannabis may address some of those drivers (especially pain and anxiety) even if it doesn’t directly improve insomnia as measured. CBD at lower doses before bed is worth exploring, as it avoids the paradoxical sleep-disrupting effect that high-dose THC can produce in some patients.
The Drug Interaction Reality: What ALS Patients and Caregivers Must Know
ALS patients typically take riluzole (Rilutek) as the primary disease-modifying medication, and many receive edaravone (Radicava) as well. Both have interaction considerations with cannabinoids.
Riluzole and CBD
Riluzole is metabolized primarily by the CYP1A2 enzyme. CBD is a moderate inhibitor of CYP1A2. This means CBD can slow riluzole metabolism, potentially increasing riluzole plasma concentrations. Elevated riluzole levels are associated with liver enzyme elevations and other adverse effects. This interaction has not been formally studied in humans, but the pharmacokinetic mechanism is established. ALS patients on riluzole who use cannabis should discuss this with their neurologist and consider monitoring liver enzymes more closely.
Opioid medications
Many ALS patients in the middle and later stages use opioids for pain and respiratory comfort. CBD inhibits CYP3A4 and CYP2D6, the enzymes that metabolize most opioids, which can increase opioid plasma levels and sedation. Dose adjustments may be needed. This is also true in the opposite direction — cannabis can enhance opioid analgesia, potentially allowing lower opioid doses, which is a meaningful benefit for respiratory-compromised ALS patients.
Benzodiazepines
Commonly used in ALS for anxiety and muscle relaxation. Additive CNS depression with cannabis. Monitor for increased sedation and respiratory suppression, particularly as ALS pulmonary function declines.
Baclofen and tizanidine
Standard antispastic medications. Additive muscle relaxation with cannabis. Generally not dangerous but may require dose adjustment.
Always bring a complete, current medication list to the physician certification appointment. The certifying physician will review interactions as part of the evaluation.
Practical Access: What the Telehealth Evaluation Looks Like for ALS Patients
For an ALS patient in the early stages of the disease, a telehealth evaluation is typically straightforward. The certifying physician needs to confirm your ALS diagnosis and discuss which symptoms you want to address. Documentation of your diagnosis — a neurologist’s letter, clinic notes, or nerve conduction study results — is helpful but not always required if your diagnosis is established and your physician is familiar with your case.
For patients in the middle or later stages of ALS, practical challenges emerge:
- Difficulty speaking (dysarthria or anarthria)
- Difficulty typing or using a touchscreen
- Fatigue that makes extended appointments difficult
- Respiratory compromise requiring supplemental oxygen or ventilatory support
These challenges do not disqualify you from participating in the PA medical marijuana program. Here is how they can be accommodated:
Caregiver assistance
Pennsylvania allows up to two designated caregivers per patient. A caregiver can be present during and assist with the telehealth appointment. They can handle the state registration process on the patient’s behalf and make all dispensary purchases. If you have a family member or care aide who will be managing your day-to-day needs, registering them as your caregiver should happen alongside — or shortly after — your patient registration.
Communication accommodations
If speech is affected, inform the practice when scheduling. Many telehealth platforms support text chat as a supplement to video, and some physicians have experience accommodating non-verbal communication during ALS evaluations.
Documentation
If your speaking or typing ability is limited, having a family member or caregiver ready to describe your symptoms, current medications, and treatment history during the evaluation will make the appointment more efficient.
Caregiver registration requirements
PA caregivers must be 21 or older, pass a criminal history background check, and pay a $25 registration fee. The caregiver is then authorized to purchase cannabis from any licensed PA dispensary on the patient’s behalf.
Which Cannabis Products Are Most Practical for ALS Patients?
Pennsylvania’s approved forms include oils/tinctures, capsules/pills, vaporizable dry leaf, topicals, patches, and liquid solutions (including metered-dose inhalers).
For ALS patients, product selection is strongly influenced by motor function and respiratory status:
Oils and tinctures are generally the most practical option for ALS patients at most disease stages. They allow precise dose control, have a longer duration of effect than inhaled forms, do not require fine motor dexterity to use (a dropper can be managed by a caregiver), and avoid any respiratory burden. For appetite stimulation, starting doses of THC-containing tinctures are typically low (2.5–5 mg THC) and titrated based on response.
Capsules and pills are useful for patients who can still swallow comfortably. For patients with swallowing difficulties (dysphagia), which is common in bulbar-onset ALS, capsules become impractical and tinctures or liquid solutions are preferable.
Vaporized dry leaf provides faster onset (helpful for acute spasm or pain episodes) but is generally not appropriate for ALS patients with respiratory involvement. For patients in early stages with full respiratory function and no dysphagia, vaporization may be an option — but as respiratory function declines, inhaled forms should be reconsidered.
Dermal patches provide steady, slow delivery of cannabinoids through the skin. They are particularly useful for ALS patients who need consistent symptom management without repeated dosing — caregivers can apply them once or twice daily without requiring patient action.
Topicals are useful for localized muscle pain and spasticity but do not provide systemic effects. They are worth considering as an adjunct for specific painful areas.
Your dispensary pharmacist is the most important resource for product selection at a specific dispensary — they know their current inventory, can advise on ratios and formulations, and can adjust recommendations as your symptoms change.
How to Get Your Pennsylvania Medical Marijuana Card for ALS?
Step 1 — Physician Certification (Telehealth)
Schedule a telehealth appointment with a PA DOH-registered medical marijuana physician. The appointment typically takes 10–15 minutes. The physician will confirm your ALS diagnosis, discuss your symptom profile and current medications, and issue a certification if you qualify. If a caregiver will be assisting with the appointment, let the practice know when scheduling.
Step 2 — State Registration
After your certification is issued, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com). You will need your certification, a valid Pennsylvania driver’s license or state-issued ID, and payment of the $50 state fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 3 — Caregiver Registration (If Applicable)
Register your designated caregiver at the same portal. The caregiver completes their own registration, submits to a background check, and pays the $25 caregiver fee. Once registered, they can purchase cannabis from any licensed PA dispensary on your behalf.
Step 4 — Visit a Licensed PA Dispensary
Your temporary approval is issued immediately upon successful registration. Use the PA DOH dispensary locator to find a licensed dispensary near you. Tell the dispensary pharmacist that you have ALS and describe which symptoms you are primarily targeting — they will help you select an appropriate product and starting dose.
- Source: PA DOH – Patient and Caregiver Registration Source: PA Medical Marijuana Program Patient Registry
Other Qualifying Conditions
- Chronic Hepatitis C
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
Frequently Asked Questions
Q: I was diagnosed with ALS years ago. Can I still get a PA MMJ card?
Q: My ALS is advanced. Can I still qualify and access dispensaries?
Q: Will cannabis interact with my riluzole?
Q: Can I use cannabis alongside hospice care?
Q: Does cannabis slow ALS progression?
Q: Does Pennsylvania cover medical cannabis costs for ALS patients?
ALS Support Resources
The ALS Association (als.org) is the primary national advocacy and support organization for ALS patients and families. They provide a care services locator, free equipment loan programs, clinical trial information, and ALS-specific guidance on medical marijuana.
ALS Association Pennsylvania Chapter (alsphiladelphia.org for the Philadelphia chapter; alsofwpa.org for the Western PA chapter) offers local support groups, care coordination, equipment lending, and connection to ALS specialists throughout the state.
NIH/NINDS – ALS Information at ninds.nih.gov provides authoritative clinical information about disease progression, current treatments, and ongoing research.
ALS News Today (alsnewstoday.com) covers clinical research developments in ALS including cannabis-related studies with good scientific accuracy and regular updates.
NOTE: An ALS diagnosis is one of the most difficult things a person and a family can face. Medical cannabis is not a solution to that — but for specific symptoms, particularly pain, appetite, and anxiety, it can be a meaningful part of managing the day-to-day burden of the disease. Pennsylvania’s program exists precisely so patients do not have to navigate this without legal protection and proper guidance.
If you are ready to begin the evaluation process, a PA-registered physician can complete your certification by telehealth — from home, with a caregiver present if needed. The process should be the least of your concerns right now.