
Crohn’s disease is one of the most physically and emotionally demanding chronic conditions a person can live with. The abdominal pain, unpredictable flares, diarrhea, nausea, and appetite collapse don’t follow a schedule. The medications that work for some patients don’t work for others. And even when treatment controls the inflammation, the daily symptom burden — pain, fatigue, anxiety about flares — often persists.
Pennsylvania recognized this when it included Crohn’s disease as a qualifying condition in its Medical Marijuana Act from day one. The research behind this decision is more nuanced than most websites explain, and understanding that nuance matters — both for setting the right expectations and for getting the most out of cannabis if you choose to pursue it.
This page gives you an honest account of what the clinical evidence actually shows, including a finding that every Crohn’s patient considering cannabis should understand before starting, what symptoms respond most consistently, and exactly how to get your PA MMJ card.
Does Crohn’s Disease Qualify for Medical Marijuana in Pennsylvania?
Yes. Crohn’s disease is an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016) and is recognized by the Pennsylvania Department of Health (DOH) for both adult and minor patients.
Any confirmed Crohn’s disease diagnosis qualifies — there is no requirement that the disease be severe, active, or treatment-resistant. Patients in remission qualify just as those in active flare do, because the symptom burden and quality-of-life impact of Crohn’s extends well beyond active inflammation. The certifying physician will discuss which specific symptoms cannabis is intended to address, and that shapes product guidance.
Crohn’s disease also qualifies separately under Pennsylvania’s “inflammatory bowel disease” (IBD) condition — making it one of the few conditions on Pennsylvania’s list covered under two distinct qualifying categories. Your certifying physician may note one or both on your certification.
- Source: Pennsylvania Department of Health – Medical Marijuana Program
- Source: Pennsylvania Medical Marijuana Act – Act 16 of 2016
What Is Crohn’s Disease?
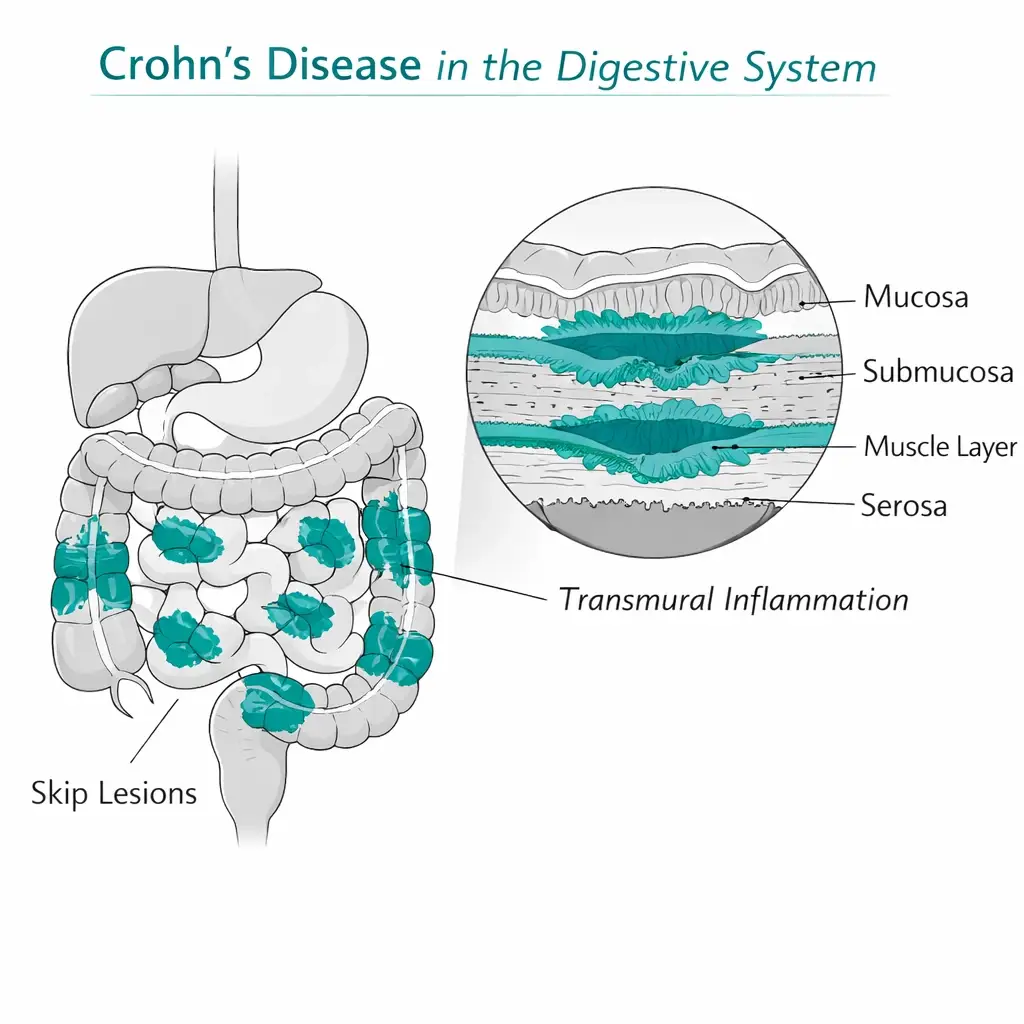
Crohn’s disease is a chronic inflammatory bowel disease (IBD) that can affect any part of the gastrointestinal tract from the mouth to the anus, though it most commonly involves the small intestine and the beginning of the large intestine. Unlike ulcerative colitis — which is limited to the colon — Crohn’s can produce transmural inflammation (affecting all layers of the intestinal wall) and can skip areas, leaving patches of normal tissue between inflamed sections.
The disease course is characterized by cycles of flares and remission, but many patients experience persistent symptoms even in nominal remission. Common symptoms include:
- Abdominal pain and cramping, often severe
- Chronic or episodic diarrhea
- Nausea and vomiting
- Significant appetite loss and unintended weight loss
- Fatigue — frequently debilitating, independent of active inflammation
- Anxiety and depression driven by symptom unpredictability and quality-of-life disruption
- Joint pain (extraintestinal manifestation in roughly 20% of patients)
Standard medical treatment includes aminosalicylates, corticosteroids, immunomodulators (azathioprine, 6-mercaptopurine, methotrexate), and biologic therapies (anti-TNF agents like infliximab and adalimumab, anti-integrin therapies, and newer IL-12/23 inhibitors). Response rates to current therapies are limited: only 40–60% of patients achieve adequate control on initial treatment, and many cycle through medications seeking adequate symptom management.
According to a 2023 analysis published in BMJ Open (Wang et al.), the global burden of IBD has risen significantly across 204 countries from 1990 to 2019 — a trajectory that reflects both improved diagnosis and genuinely increasing incidence in higher-income countries.
Why the Endocannabinoid System Is Directly Relevant to Crohn’s Disease
Understanding why cannabis is scientifically relevant to Crohn’s specifically — not just as a general symptom reliever — helps set realistic expectations and makes sense of the clinical trial results.
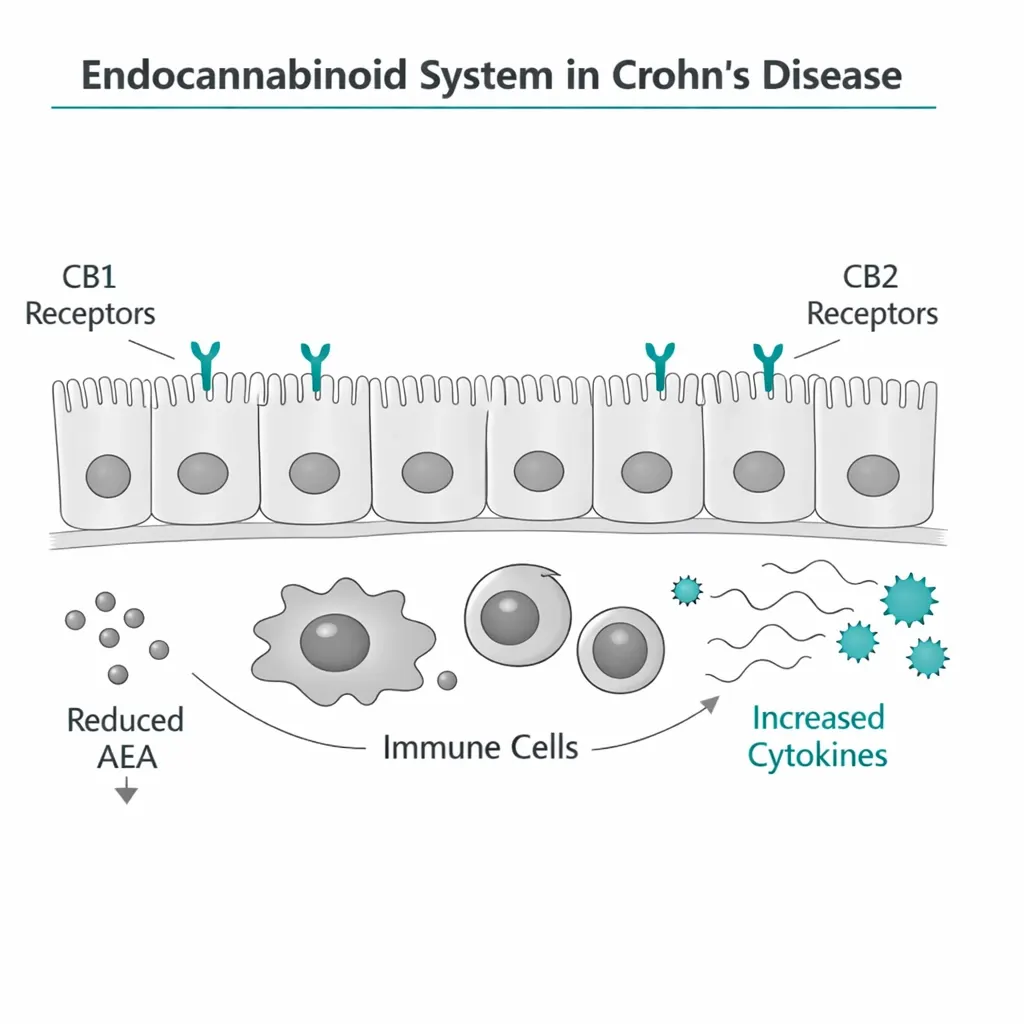
The endocannabinoid system (ECS) is densely expressed throughout the gastrointestinal tract: in enteric nerve fibers (the gut’s own nervous system), in intestinal epithelial cells, in immune cells in the gut wall, and in the smooth muscle that controls motility. The ECS plays a direct role in regulating intestinal motility, gut permeability, visceral pain signaling, and the inflammatory immune response in the gut.
In Crohn’s disease specifically, research has found that ECS function is disrupted. A study published in Mucosal Immunology found significantly lower levels of anandamide (AEA — a key endocannabinoid) in inflamed Crohn’s mucosa compared to non-inflamed tissue, alongside elevated FAAH enzyme activity (the enzyme that breaks down anandamide). The effect: the gut’s natural anti-inflammatory endocannabinoid signaling is being rapidly degraded precisely where inflammation is highest.
A 2024 study in Applied Biosciences and Bioengineering measured endocannabinoid levels in adolescent Crohn’s patients and found that AEA concentrations were consistently lower throughout the disease course — in active disease, during treatment, and in remission — compared to healthy controls. This persistent deficit suggests the ECS dysregulation is a feature of Crohn’s pathophysiology, not just an acute inflammatory response.
What this means practically: exogenous cannabinoids (THC, CBD) are not simply acting as general painkillers or anti-nausea agents in Crohn’s. They are interacting with a system that is specifically disrupted in this disease — CB1 and CB2 receptors that regulate gut motility, inflammation, and pain, in a tissue where the body’s own cannabinoid tone is depleted.
This is the scientific basis for why Crohn’s has been among the IBD conditions most consistently studied for cannabis, and why the results, while imperfect, are directionally meaningful.
- Source: PMC – Cannabis, Cannabinoids, and the Endocannabinoid System in IBD (Journal of Crohn’s and Colitis, 2019)
- Source: PMC – Endocannabinoid System as a Promising Therapeutic Target in IBD (Frontiers in Immunology, 2021)
- Source: MDPI – Endogenous Cannabinoids in Crohn’s Disease in Children (2024)
The Most Important Thing to Understand About the Research: Clinical vs. Endoscopic Response
Before reviewing the individual studies, there is one finding that every Crohn’s patient considering medical cannabis needs to understand — because it defines what cannabis realistically can and cannot do for this disease.
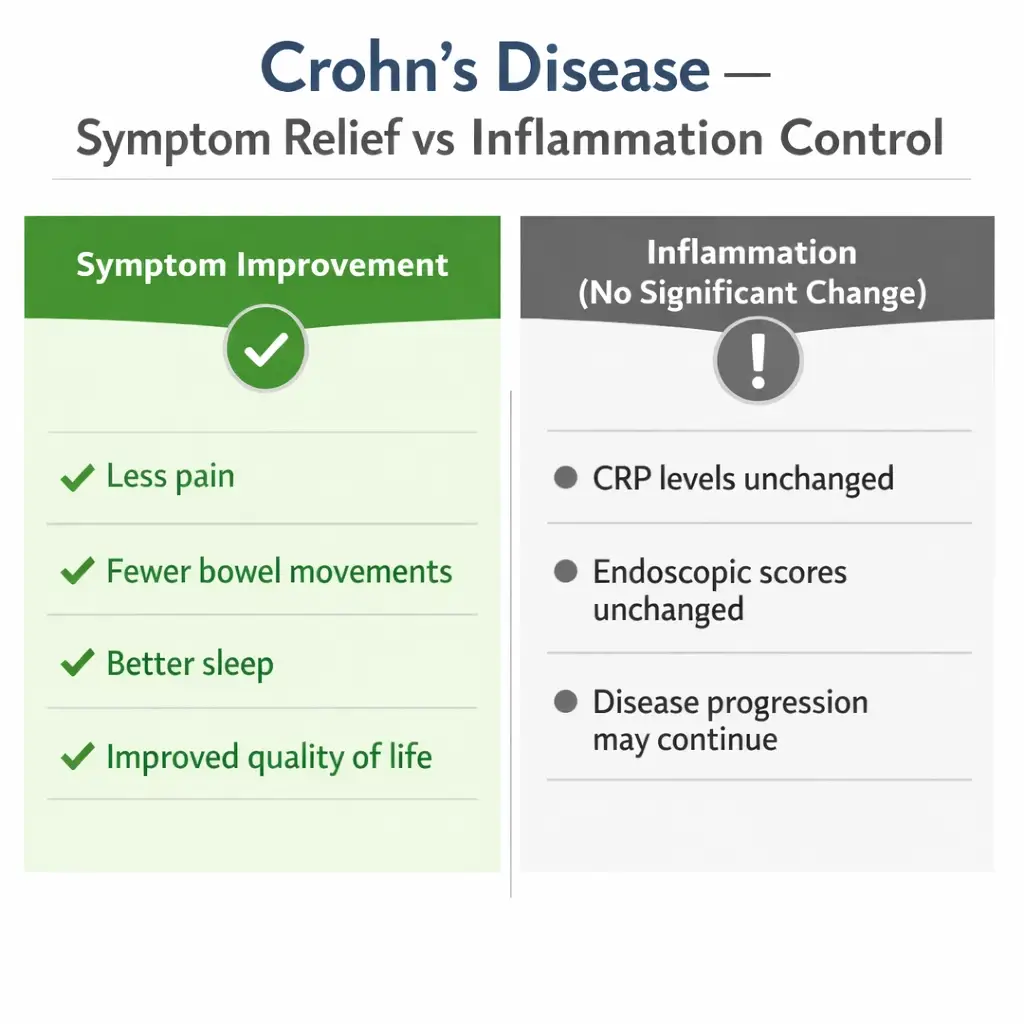
Cannabis consistently improves how Crohn’s patients feel. It does not consistently reduce the underlying intestinal inflammation as measured by objective tests.
This is called the clinical versus endoscopic response gap, and it appears across multiple randomized controlled trials. In plain terms:
- Patients report meaningful improvement in abdominal pain, bowel movements, quality of life, sleep, appetite, and overall wellbeing
- Endoscopic scores (what the camera sees inside the bowel), CRP levels, and fecal calprotectin (objective markers of gut inflammation) typically do not show significant improvement
This matters enormously for treatment decisions. Crohn’s care has moved toward a “treat-to-target” strategy where the goal is mucosal healing — visible reduction in intestinal inflammation — not just symptom control. A patient can feel significantly better while the underlying disease progresses. Cannabis appears to address the former reliably without addressing the latter.
This is not a reason to dismiss cannabis. Symptom control is a legitimate and important treatment goal in Crohn’s, particularly when standard therapies are inadequate. But it means cannabis is a symptom management tool, not a disease-modifying treatment — and decisions about your core Crohn’s treatment regimen need to remain with your gastroenterologist.
The editorial response to the landmark 2021 Naftali RCT in Journal of Crohn’s and Colitis summarized this precisely: “Quality of life improvements are real and robust, but again cannabis falls short in treating inflammation.”
What the Clinical Research Shows
The 2025 Meta-Analysis of RCTs — The Strongest Current Evidence
The most current and rigorous synthesis of the RCT evidence is a January 2025 meta-analysis published in the Irish Journal of Medical Science, registered with PROSPERO (CRD42023479375), covering five randomized controlled trials in Crohn’s disease.
The key finding: the cannabis group showed significantly higher clinical remission rates at 8 weeks compared to the control group, with low heterogeneity between studies. However, a statistically significant improvement in quality of life was observed in the placebo group — reflecting the high placebo response rate common in Crohn’s trials. CRP levels showed a trend toward reduction in the cannabis group that did not reach statistical significance.
The meta-analysis concluded that cannabis shows promise as a therapeutic option for Crohn’s disease, with higher clinical remission rates and symptom management benefits, while calling for larger, standardized studies to confirm efficacy, safety, and biomarker responses.
The Naftali 2021 CBD-Rich Oil RCT — The Most Rigorous Single Trial
The most methodologically sound single trial is a 2021 double-blind, randomized, placebo-controlled study by Naftali et al. published in the Journal of Crohn’s and Colitis. Patients with active Crohn’s received either a CBD-rich cannabis oil (160 mg/ml CBD, 40 mg/ml THC) or placebo for eight weeks.
Results showed significant improvement within the cannabis group in Crohn’s Disease Activity Index (CDAI) scores, number of bowel movements, abdominal pain, and quality of life. Improvement in sleep, pain, abdominal swelling, appetite, and general wellbeing was significantly more pronounced in the cannabis group than placebo.
However — and this is the clinical vs. endoscopic gap — there were no significant changes in inflammatory markers or endoscopic scores. CRP, fecal calprotectin, and Simple Endoscopic Score for Crohn’s (SES-CD) did not significantly differ between groups. The authors concluded: “eight weeks of CBD-rich cannabis treatment induced significant clinical and QOL improvement without significant changes in inflammatory parameters or endoscopic scores.”
The Naftali 2013 THC-Rich Placebo-Controlled Study — The Original Signal
The foundational clinical evidence for cannabis in Crohn’s came from an earlier Naftali et al. placebo-controlled study published in Clinical Gastroenterology and Hepatology (2013). Patients with active Crohn’s who had failed at least one conventional therapy received either THC-rich cannabis cigarettes (115 mg THC daily) or placebo for eight weeks.
Ten of 11 patients in the cannabis group experienced significant clinical benefit versus 4 of 10 in the placebo group. Five cannabis patients achieved complete clinical remission (CDAI < 150) versus 1 in the placebo group. There was also a steroid-sparing effect: several cannabis patients reduced or discontinued corticosteroid use.
This was the study that cemented Crohn’s as a qualifying condition in multiple state medical marijuana programs. Its limitation is the same as every subsequent trial: no significant reduction in CRP or endoscopic improvement was observed.
The 2022 MDPI Meta-Analysis — Cannabinoids as Adjuvant Therapy
A 2022 meta-analysis published in Biomedicines (MDPI) covering five randomized controlled trials and 208 IBD patients found that cannabinoid supplementation as adjuvant therapy has the potential to increase the success rate of standard Crohn’s treatment during the induction period. Pooled CDAI reduction was statistically significant in the CD patient group. The analysis found low heterogeneity between studies.
Critically, the authors recommended cannabis only as an adjunct to — not a replacement for — conventional Crohn’s treatment, and noted the evidence for maintenance therapy is insufficient.
The 2025 Scoping Review — Real-World Use Patterns
A comprehensive 2025 scoping review in Cannabis and Cannabinoid Research (Brodaric et al.) analyzed 40 studies — including 7 RCTs, 6 cohort studies, 10 surveys, and 3 meta-analyses — on cannabis use in IBD patients. Key findings: between 11% and 17.6% of IBD patients surveyed were active cannabis users for symptom control, with lifetime prevalence of 39.8–78.2%. Patient-reported outcomes consistently showed reduced abdominal pain, emotional distress, stool frequency, and anorexia. Crohn’s patients consistently reported more symptom relief than ulcerative colitis patients across specific symptom categories.
- Source: Cannabis and Cannabinoid Research – Cannabinoids for IBD: Scoping Review (Brodaric et al., 2025)
Symptom by Symptom: Where Cannabis Helps Crohn’s Patients Most

Abdominal Pain
This is the most consistently reported area of benefit across every category of Crohn’s cannabis research — RCTs, cohort studies, and patient surveys alike. THC is the primary analgesic cannabinoid. CB1 receptors in enteric nerves and spinal pain pathways respond to THC by reducing visceral pain signal transmission. Over 50% of IBD cannabis users in survey studies reported significant relief from abdominal pain. Pain improvement is among the most robust and consistent findings in the Crohn’s-cannabis literature.
Diarrhea and Bowel Frequency
Cannabis acts on CB1 receptors in the gut to reduce intestinal motility — slowing transit time and reducing stool frequency. Multiple clinical trials have shown reductions in bowel movement frequency in THC-rich cannabis groups. This is a direct pharmacological effect on gut physiology, not just a subjective perception shift. For patients whose bowel frequency is a major driver of quality-of-life impairment, this is a meaningful clinical target.
Nausea
Nausea in Crohn’s arises both from active intestinal disease and from medications (methotrexate and many biologics cause nausea). Cannabis’s antiemetic properties are among its most established pharmacological effects — dronabinol has been FDA-approved for nausea since 1985. For Crohn’s patients managing both disease-related and medication-induced nausea, cannabis addresses both mechanisms simultaneously.
Appetite Loss and Weight Maintenance
Appetite loss and unintended weight loss are serious features of active Crohn’s disease and can persist even between flares in patients with significant disease burden. THC’s appetite-stimulating effect via hypothalamic CB1 receptors is well-documented. Multiple Crohn’s clinical trials have noted improvements in appetite as part of broader quality-of-life scores. For patients with significant cachexia risk, this is a clinically important benefit.
Sleep Disruption
Chronic pain, nocturnal bowel urgency, and anxiety about symptom control are major drivers of sleep disruption in Crohn’s. Short-term improvements in sleep are among the most consistently reported benefits across the Crohn’s-cannabis literature. The 2021 Naftali RCT specifically found that improvement in sleep was significantly more pronounced in the cannabis group than placebo. CBD-dominant formulations at lower doses are generally preferred for sleep improvement, as high-dose THC can fragment sleep architecture.
Anxiety and Emotional Distress
The unpredictability of Crohn’s disease — not knowing whether a day will be manageable or severely symptomatic — drives significant anxiety, and roughly 60% of Crohn’s patients meet criteria for clinically significant psychological distress at some point. The 2025 scoping review specifically identified reduced emotional distress as one of the consistently reported patient benefits. CBD-dominant formulations are most appropriate for anxiety management.
Fatigue
Fatigue in Crohn’s is multifactorial — driven by active inflammation, nutritional deficiencies, sleep disruption, and the psychological toll of chronic illness. Cannabis has not shown consistent effects on fatigue as a primary outcome in IBD trials, but improvements in sleep, pain, and general wellbeing likely contribute to reduced fatigue perception in patients who respond.
What Cannabis Does Not Do for Crohn’s Disease
This section is as important as what cannabis does do, and most websites skip it.
Cannabis does not reduce intestinal inflammation in Crohn’s disease as measured by objective markers. Across every well-designed randomized trial — the 2021 Naftali CBD-rich oil RCT, the original 2013 THC study, multiple smaller trials — endoscopic scores, CRP, and fecal calprotectin have consistently not shown significant improvement versus placebo. This is not a minor technical point.
It means that while cannabis reliably makes patients feel better, the disease process in the bowel wall continues. Decisions about your biologic therapy, immunomodulator, or steroid management must be based on objective disease activity — not on how you feel, because cannabis will improve how you feel regardless of what the inflammation is doing.
Cannabis is not a first-line treatment for Crohn’s disease. The 2022 MDPI meta-analysis specifically recommends cannabis only as adjunctive therapy alongside standard treatment. Using cannabis as a replacement for evidence-based Crohn’s medications is likely to result in worsening disease activity over time, even if symptoms appear to improve.
Cannabis does not prevent flares or maintain remission. There is no RCT evidence showing that cannabis reduces relapse rates in Crohn’s disease.
The appropriate frame: cannabis is a symptom management adjunct — potentially a very good one for pain, diarrhea, nausea, appetite, and sleep — that works best alongside, not instead of, your gastroenterologist’s treatment plan.
Drug Interactions for Crohn’s Patients on Standard Medications
CBD inhibits several CYP450 enzymes relevant to Crohn’s medications. These interactions require clinical awareness, not necessarily avoidance.
Azathioprine and 6-mercaptopurine (6-MP): These immunomodulators are metabolized in part by pathways that CBD can affect. Some cannabis clinicians recommend monitoring blood counts more closely when combining CBD with thiopurines, though formal interaction studies in Crohn’s are lacking.
Methotrexate: CBD inhibits CYP2C9, an enzyme involved in methotrexate metabolism. Increased methotrexate plasma levels theoretically possible. Liver enzyme monitoring — already standard with methotrexate — becomes more important.
Biologic agents (infliximab, adalimumab, vedolizumab, ustekinumab): Monoclonal antibodies are not metabolized by CYP enzymes, so direct pharmacokinetic interactions are unlikely. However, cannabis’s immunomodulatory properties are a theoretical concern for patients on immunosuppressive biologics — a more cautious interaction consideration than a hard contraindication.
Corticosteroids: The 2013 Naftali study observed a steroid-sparing effect in some Crohn’s patients using cannabis. This is a potential benefit — but steroid dose changes in Crohn’s should always be managed with gastroenterologist involvement, not adjusted independently based on cannabis use.
Always bring your full Crohn’s medication list to the physician certification appointment, including biologics, immunomodulators, and any supplements. Your certifying physician will note interaction considerations, and your gastroenterologist should know about your cannabis use.
Which PA Cannabis Products Work Best for Crohn’s Symptoms
Pennsylvania’s approved forms include oils and tinctures, capsules and pills, vaporizable dry leaf (for vaporizer use only — smoking is not permitted), liquid solutions including metered-dose inhalers, dermal patches, and topicals.
For abdominal pain and diarrhea: THC-dominant or balanced THC:CBD formulations are typically most effective. THC directly reduces gut motility and provides visceral analgesia. Tinctures and oils allow dose titration and have a longer duration than inhaled forms — suitable for persistent daily pain management. Inhaled (vaporized) forms provide faster onset for acute pain spikes but shorter duration.
For nausea: Onset timing matters. For acute chemotherapy-like nausea from methotrexate or other agents, faster-onset inhaled or sublingual forms are more practical. For chronic, lower-level nausea, oral tinctures on a scheduled basis work well. THC-dominant formulations are more reliably antiemetic than CBD alone.
For appetite stimulation: THC-dominant products, typically tinctures or capsules taken 30–60 minutes before meals. Low starting doses (2.5–5 mg THC) are recommended to avoid anxiety or discomfort, particularly for patients new to cannabis.
For anxiety and sleep: CBD-dominant formulations are generally preferred. High-THC products can paradoxically worsen anxiety in some patients — particularly relevant for Crohn’s patients whose anxiety is already elevated. Lower THC, higher CBD ratios (10:1 or 20:1 CBD:THC) are a reasonable starting point for anxiety management.
For fatigue and general wellbeing: CBD-dominant formulations during daytime avoid cognitive impairment that would otherwise limit daily functioning.
Your dispensary pharmacist is your most practical guide. Tell them you have Crohn’s disease and describe which symptoms you are primarily targeting. Experienced dispensary pharmacists can recommend specific product formulations that match your symptom profile.
How to Get Your Pennsylvania Medical Marijuana Card for Crohn’s Disease
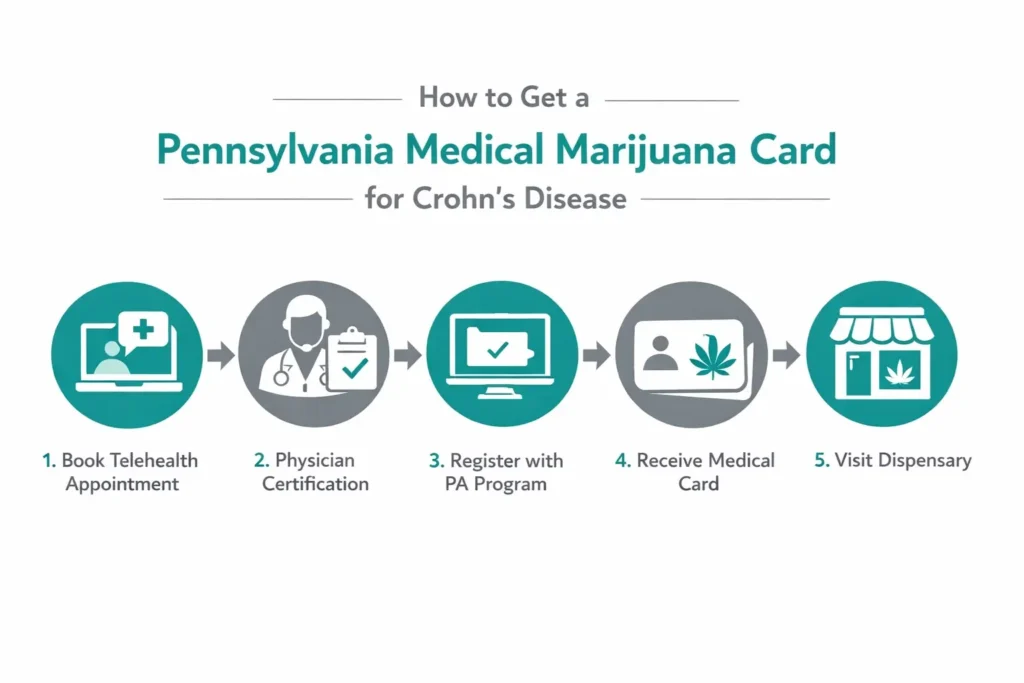
Step 1 — Physician Certification (Same-Day Telehealth)
Schedule a telehealth appointment with a PA DOH-registered medical marijuana physician. Evaluations typically take 10–15 minutes. The certifying physician does not need to be your gastroenterologist — any PA-registered physician who has a continuing care relationship with you and is familiar with your Crohn’s diagnosis can certify you. Have your diagnosis documentation available — endoscopy reports, gastroenterology records, or a recent clinic note confirming your Crohn’s diagnosis.
Bring a complete medication list. This is particularly important if you are on immunomodulators or biologics. The certifying physician will note relevant interaction considerations as part of the evaluation.
Step 2 — State Registration
After your certification is issued, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com). You will need your certification, a valid Pennsylvania driver’s license or state-issued ID, and the $50 annual fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 3 — Visit a Licensed PA Dispensary
Your temporary approval is issued immediately after registration. Use the PA DOH dispensary locator to find a licensed dispensary near you. Tell the dispensary pharmacist you have Crohn’s disease and describe which symptoms you are targeting — they will advise on appropriate products and starting doses. Be specific: “abdominal pain and diarrhea” leads to different product recommendations than “anxiety and sleep disruption.”
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
Frequently Asked Questions
Q: My Crohn’s is currently in remission. Do I still qualify?
Q: Will cannabis replace my biologic or immunomodulator?
Q: My gastroenterologist doesn’t know I’m using cannabis. Should I tell them?
Q: I have Crohn’s and ulcerative colitis in my family. Does UC also qualify?
Q: How long does the card take to get?
Q: Is medical marijuana for Crohn’s covered by insurance in Pennsylvania?
Crohn’s Disease Support Resources
Crohn’s & Colitis Foundation (crohnscolitisfoundation.org) is the leading national patient advocacy and research organization for IBD. Their patient resources include information on complementary therapies including cannabis on their website. The Foundation’s helpline is 888-694-8872.
Crohn’s & Colitis Foundation – Pennsylvania Chapter provides local support groups, educational events, and connection to gastroenterology specialists throughout the state.
NCI PDQ – Cannabis and Cannabinoids at cancer.gov is one of the most authoritative regularly updated summaries of the cannabis-IBD evidence, written for patients and clinicians.
NOTE: Crohn’s disease is a condition where the gap between how a patient feels and what is happening at the mucosal level can be significant. Cannabis addresses the former — reliably, according to the best available evidence, for pain, diarrhea, nausea, appetite, and sleep — without addressing the latter. That is not a limitation unique to cannabis; it describes most symptom management medications. Used with that understanding, and alongside rather than instead of your gastroenterologist’s treatment plan, a Pennsylvania MMJ card gives you legal access to a therapy with a meaningful evidence base and a genuine role in improving daily life with Crohn’s disease.