Hepatitis C treatment has transformed dramatically. Where a decade ago treatment meant a year of difficult injections with interferon and ribavirin — with severe side effects and inconsistent outcomes — today’s direct-acting antiviral (DAA) regimens cure hepatitis C in more than 95% of patients in just 8 to 12 weeks of oral pills with minimal side effects.
So why does chronic hepatitis C remain a qualifying condition for Pennsylvania’s medical marijuana program?
Because not everyone with hepatitis C has been cured. An estimated 2.2 million Americans still live with chronic HCV infection — many untreated due to access barriers, cost, ongoing drug use, DAA treatment failure, or a diagnosis they don’t yet know they have. And even patients who are successfully cured may carry lasting liver damage, persistent fatigue, chronic pain, and other symptoms that outlive the virus.
Pennsylvania’s Medical Marijuana Advisory Board added chronic hepatitis C to the qualifying conditions list in 2022, recognizing that cannabis can provide meaningful relief for the real symptom burden these patients carry — and, for patients still on older interferon-based regimens, may help them stay on treatment long enough to achieve a cure.
Does Chronic Hepatitis C Qualify for a PA MMJ Card?
Yes. Chronic hepatitis C — also called chronic HCV (hepatitis C virus) infection — is an explicitly named qualifying condition under Pennsylvania’s Medical Marijuana Program, added following the Advisory Board’s recommendation in March 2022.
A diagnosis of chronic hepatitis C means HCV RNA is detectable in the blood for six months or more. This covers:
- Active, untreated chronic HCV infection — patients who have not yet received or completed antiviral therapy
- Patients currently receiving treatment — on DAA regimens, on older interferon/ribavirin-based regimens, or combinations thereof, who are managing treatment side effects
- Patients with DAA treatment failure — a small but real subset (~2–5% of treated patients) for whom first-line and salvage regimens have not achieved sustained virologic response
- Patients who have achieved SVR (sustained virologic response / cure) but have residual liver damage, cirrhosis, chronic fatigue, pain, or other lasting consequences of the infection
The PA certifying physician will confirm your HCV diagnosis from your medical records. Laboratory documentation showing a positive HCV RNA test or a current HCV specialist’s notes are the standard documentation.
- Source: Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Source: 28 Pa. Code Appendix A – Serious Medical Conditions
- Source: PennsylvaniaStateCannabis.org – Advisory Board Added Chronic Hepatitis C in 2022
Who Is This Qualifying Condition Actually For?
Patients Still Living with Active HCV
Despite DAA therapy being highly effective and widely recommended, treatment gaps remain substantial. CDC data show that only a fraction of the estimated 2.2 million Americans with chronic HCV infection have initiated treatment. Barriers include: lack of diagnosis (an estimated half of people with HCV don’t know they have it), cost and insurance access issues, substance use disorders that complicate treatment engagement, mental health comorbidities, and simply not yet being connected to a provider who manages HCV.
For these patients — living with active HCV infection and managing its symptoms — cannabis can help with the fatigue, abdominal discomfort, nausea, appetite loss, sleep disruption, and anxiety that chronic HCV commonly produces.
Patients on Interferon-Containing Regimens
While DAAs have largely replaced interferon-based therapy in standard U.S. clinical practice, pegylated interferon plus ribavirin continues to be used in some clinical scenarios — including certain genotypes where DAAs are contraindicated, patients with specific co-infections, resource-limited settings, and some patients awaiting insurance authorization for newer regimens.
Interferon-ribavirin therapy produces a notoriously difficult side effect profile: fatigue affecting up to 85% of patients, flu-like symptoms in nearly half, nausea and appetite loss, depression and irritability, insomnia, muscle and joint pain, and weight loss. These symptoms are severe enough that approximately 10–20% of patients in clinical trials discontinued therapy early due to adverse events — a problem because incomplete treatment substantially reduces the chance of cure.
This is where cannabis has its most documented clinical role in hepatitis C management.
Patients with Residual Liver Damage or Post-SVR Symptoms
Achieving SVR (cure) does not always resolve all the consequences of years of chronic HCV infection. Patients who developed significant liver fibrosis or cirrhosis before treatment may continue to have:
- Fatigue that does not fully resolve after viral clearance
- Chronic abdominal discomfort related to portal hypertension or cirrhosis
- Pain from hepatic complications
- Sleep disturbances
- Anxiety related to ongoing liver monitoring and risk of hepatocellular carcinoma (HCC) in patients with advanced fibrosis
For these patients, the PA MMJ qualifying condition remains appropriate even after the virus has been eliminated.
What the Research Shows: Cannabis for HCV Symptoms
Treatment Adherence — The Most Important Role
The foundational cannabis-and-hepatitis-C research was conducted in the era of interferon-ribavirin treatment, and it identified a clinically significant finding: cannabis helped patients stay on treatment.
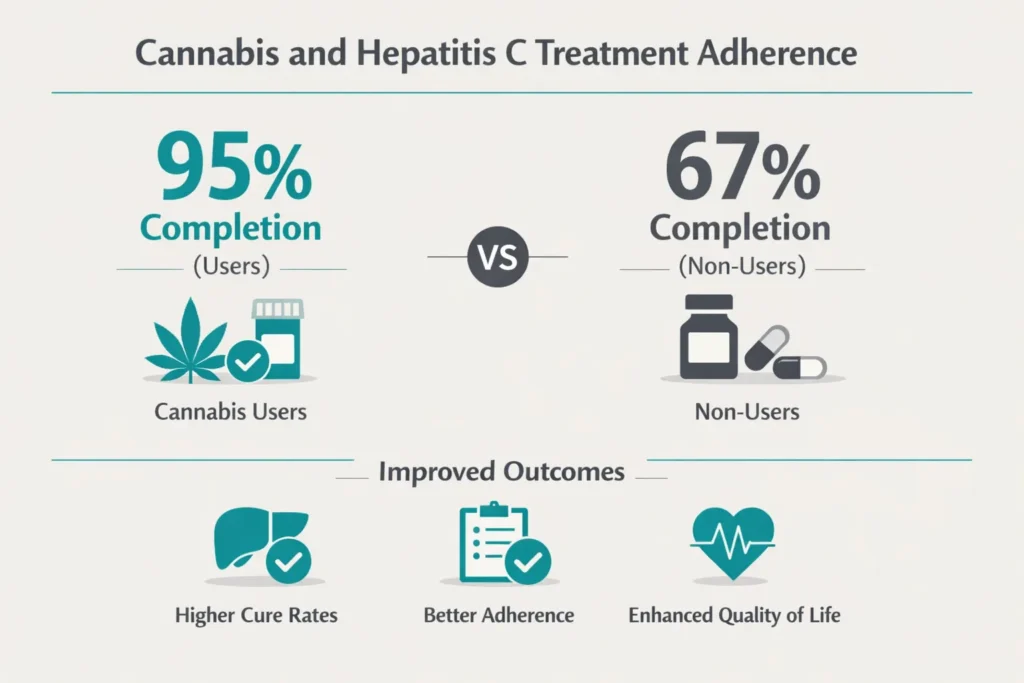
A landmark 2006 prospective observational study by Dr. Diana Sylvestre of the University of California, San Francisco (European Journal of Gastroenterology and Hepatology) followed 71 recovering substance users undergoing interferon-ribavirin treatment for HCV. Cannabis users in this cohort were significantly more likely to remain on treatment: 95% of cannabis users completed at least 80% of the projected treatment duration, compared to 67% of non-users (P=0.01). Among those completing treatment, 54% of cannabis users achieved sustained virologic response compared to 18% of non-users (P=0.009) — a difference the researchers attributed to the better treatment adherence in the cannabis group rather than any direct antiviral effect of cannabis.
A separate retrospective study from the University of Ottawa’s Viral Hepatitis Clinic examined patients who received oral cannabinoid medications (nabilone or dronabinol) alongside interferon-ribavirin. Among patients using oral cannabinoids, 78% completed the full course of HCV therapy, compared to 49% of non-recipients (P=0.02). The oral cannabinoids helped stabilize weight loss and manage anorexia and nausea — the specific side effects most likely to derail treatment adherence.
The mechanism is practical rather than pharmacological: cannabis reduces the symptom burden enough that patients can tolerate the full duration of treatment. For interferon-ribavirin regimens, where completing the full prescribed course is closely tied to cure rates, this is clinically significant.
- Source: PubMed – Cannabis Use Improves Retention and Virological Outcomes in Patients Treated for Hepatitis C (Sylvestre et al., European Journal of Gastroenterology and Hepatology, 2006)
- Source: PMC – Oral Cannabinoids for Management of Interferon and Ribavirin-Induced Anorexia, Nausea, and Weight Loss in HCV (Ottawa Viral Hepatitis Clinic)
Fatigue — The Most Persistent Symptom
Fatigue is the most common and often most debilitating symptom of chronic HCV, affecting the majority of patients whether or not they are on treatment. Unlike fatigue from many other conditions, HCV-related fatigue frequently persists even after viral clearance in patients who had prolonged infections, complicating what should be a recovery.
Cannabis, particularly CBD-dominant and balanced THC:CBD products, has documented effects on fatigue in inflammatory and chronic disease contexts. The mechanism involves both direct endocannabinoid system modulation of energy regulation and indirect effects through improving sleep quality — poor sleep being a major driver of daytime fatigue in HCV patients.
Nausea, Appetite Loss, and Weight Maintenance
Nausea and appetite loss are central symptoms of both active HCV infection and its treatments. THC’s antiemetic properties — mediated through CB1 receptors in the brainstem’s vomiting center — are among the most reliably documented effects in cannabinoid medicine. Dronabinol (synthetic THC) has been FDA-approved as an antiemetic since 1985. For HCV patients managing nausea from ribavirin or from advancing liver disease, cannabis offers an accessible and generally well-tolerated antiemetic option.
Weight maintenance is particularly important in HCV treatment because ribavirin-induced anorexia and weight loss can compound anemia and worsen the overall clinical picture during therapy. Cannabis-mediated appetite stimulation is the mechanism behind the Ottawa clinic’s finding of improved weight outcomes in oral cannabinoid users.
Pain and Discomfort
Chronic HCV is associated with abdominal discomfort (right upper quadrant pain from hepatomegaly or portal hypertension), generalized musculoskeletal pain, and in patients with advancing cirrhosis, more complex pain syndromes. Cannabis’s analgesic properties are applicable across these presentations, particularly for neuropathic and inflammatory pain components.
Sleep and Anxiety
Sleep disruption is nearly universal in active HCV infection and common in patients with advanced liver disease. Anxiety — related to HCV stigma, uncertainty about disease progression, fear of liver cancer monitoring, and the cognitive burden of managing a chronic infection — is also prevalent. Cannabis’s effects on sleep and anxiety are discussed in more detail on the anxiety disorders and terminal illness pages of this site; they apply equally to HCV patients navigating a serious chronic liver condition.
The Most Important Question: Is Cannabis Safe for the Liver in HCV?
This is the central question this page exists to answer honestly, and no competing PA MMJ site addresses it. The answer is nuanced — and the distinction between daily heavy smoking and moderate use matters enormously.
The Fibrosis Concern — Where It Comes From
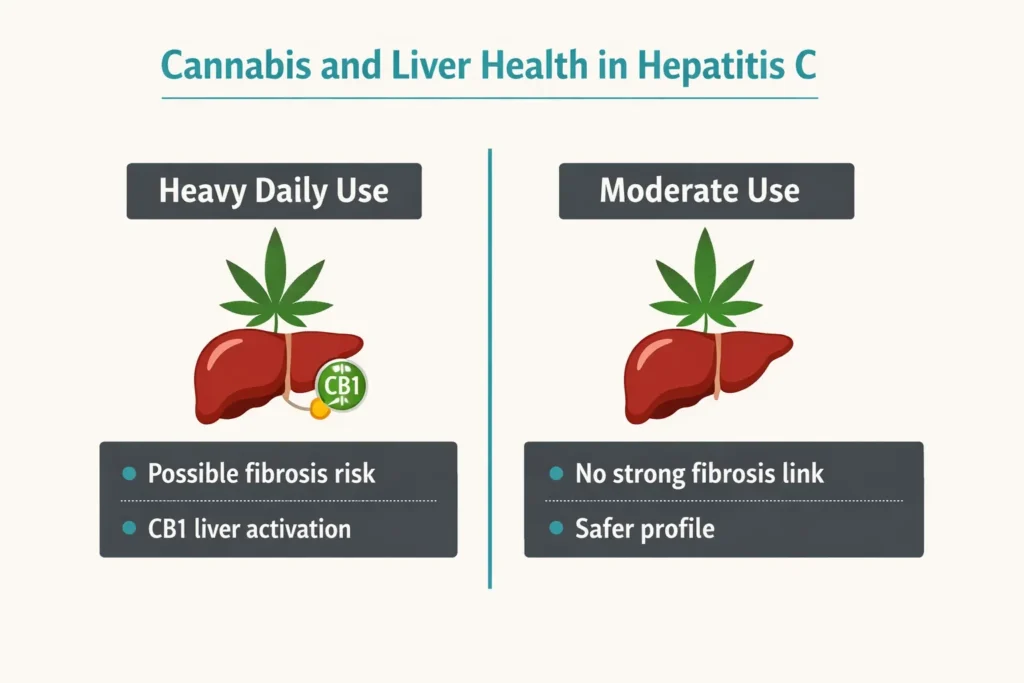
Two influential French studies, published in 2005 and 2008 (Hepatology and Gastroenterology), examined patients with chronic HCV who underwent liver biopsy. They found that daily cannabis smoking was independently associated with faster liver fibrosis progression and greater liver steatosis (fat accumulation) in patients with untreated HCV.
The proposed mechanism involves CB1 receptors in the liver. In HCV infection, CB1 receptor expression is upregulated — it increases with fibrosis stage and is associated with steatosis. THC, as a CB1 agonist, may therefore stimulate the same hepatic pathway that drives fibrosis and fat accumulation in already-inflamed liver tissue.
This is a real finding and should be taken seriously. The researchers’ conclusion from the fibrosis study was unambiguous: “Patients with ongoing CHC should be advised to refrain from regular cannabis use.”
The Counterbalancing Evidence
A 2018 systematic review and meta-analysis that pooled data from multiple studies found no statistically significant association between marijuana use and progression of hepatic fibrosis in HCV and HCV-HIV co-infected patients. On the contrary, the meta-analysis found a lower prevalence of hepatic steatosis in marijuana users compared to non-users in certain subgroups.
A 2014 retrospective study from the Ottawa Viral Hepatitis Clinic directly assessed whether cannabis use affected liver biopsy histology and found no significant effect of marijuana use on liver fibrosis or steatosis in their cohort of treated patients.
The reconciliation: The fibrosis concern appears most relevant to daily, heavy cannabis smoking in patients with untreated, active HCV infection. The weight of the broader evidence, particularly from cohorts of patients receiving treatment, suggests that moderate cannabis use does not significantly accelerate fibrosis. The French studies may reflect a confound: patients with more advanced liver disease (who were suffering more severely from their infection) may have been more likely to use cannabis heavily to self-medicate.
- Source: PubMed – Daily Cannabis Smoking as a Risk Factor for Fibrosis in Chronic Hepatitis C (Hézode et al., Hepatology, 2005)
- Source: PMC – Marijuana Is Not Associated with Progression of Hepatic Fibrosis in Liver Disease: Systematic Review and Meta-Analysis
- Source: PMC – Marijuana Use in Hepatitis C Does Not Affect Liver Biopsy Histology or Treatment Outcomes (Ottawa, 2014)
The Practical Guidance
Given this landscape, the most defensible recommendations for HCV patients considering cannabis are:
- Discuss with your hepatologist or gastroenterologist before starting cannabis, particularly if you have active (uncured) HCV infection with any fibrosis or steatosis on biopsy.
- Avoid daily heavy smoking of high-THC cannabis flower if you have active HCV infection with liver fibrosis. This is the pattern most associated with the concerning French findings.
- Oral products (tinctures, capsules) avoid the additional risks of combustion products on liver and lung health. For HCV patients, oral administration is the preferred route for any cannabis use.
- Moderate, intermittent use — targeting specific symptoms rather than constant background dosing — is a more cautious approach for patients with active liver disease.
- Alcohol avoidance remains far more important. Even moderate alcohol use is a major independent risk factor for fibrosis progression in HCV and should be the first thing eliminated. Cannabis is not in the same category of hepatotoxic risk.
Critical Warning: Drug Interactions with HCV Medications
This section is absent from every competing PA MMJ page and represents a genuine patient safety issue.
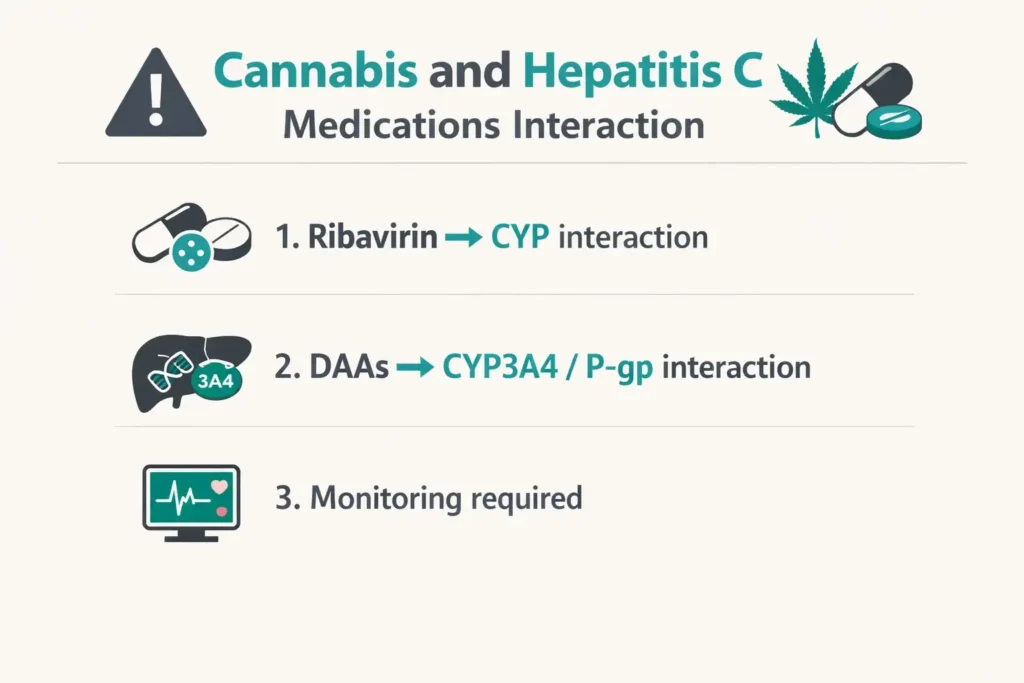
Ribavirin and cannabis: Both ribavirin and cannabinoids (particularly CBD) are metabolized through the cytochrome P450 (CYP) enzyme system — primarily CYP2C8, CYP2C9, and CYP3A4. CBD is a potent inhibitor of several CYP enzymes. In theory, CBD could reduce ribavirin clearance, potentially raising ribavirin plasma levels and increasing the risk of ribavirin’s known toxicities (particularly hemolytic anemia). Clinical interaction data in humans is limited, but this theoretical interaction should be disclosed to the treating HCV physician when cannabis is introduced.
Sofosbuvir (Sovaldi, Harvoni, Epclusa, Mavyret components): Sofosbuvir and most other DAA components are substrates of P-glycoprotein (P-gp) and CYP3A4. Cannabis — particularly CBD — can inhibit these transporters and enzymes. The clinical significance of these interactions in HCV treatment is not well-characterized, but patients should inform their HCV treating physician and pharmacist when starting cannabis, enabling them to monitor for any unexpected changes in drug efficacy or side effects.
The key rule: Tell your HCV doctor. Do not start cannabis while on antiviral therapy without first informing your treating hepatologist or gastroenterologist and pharmacist. In most cases, moderate cannabis use with standard DAA regimens is unlikely to cause significant interactions, but the physician needs to know in order to monitor appropriately.
PA Dispensary Guidance for HCV Patients
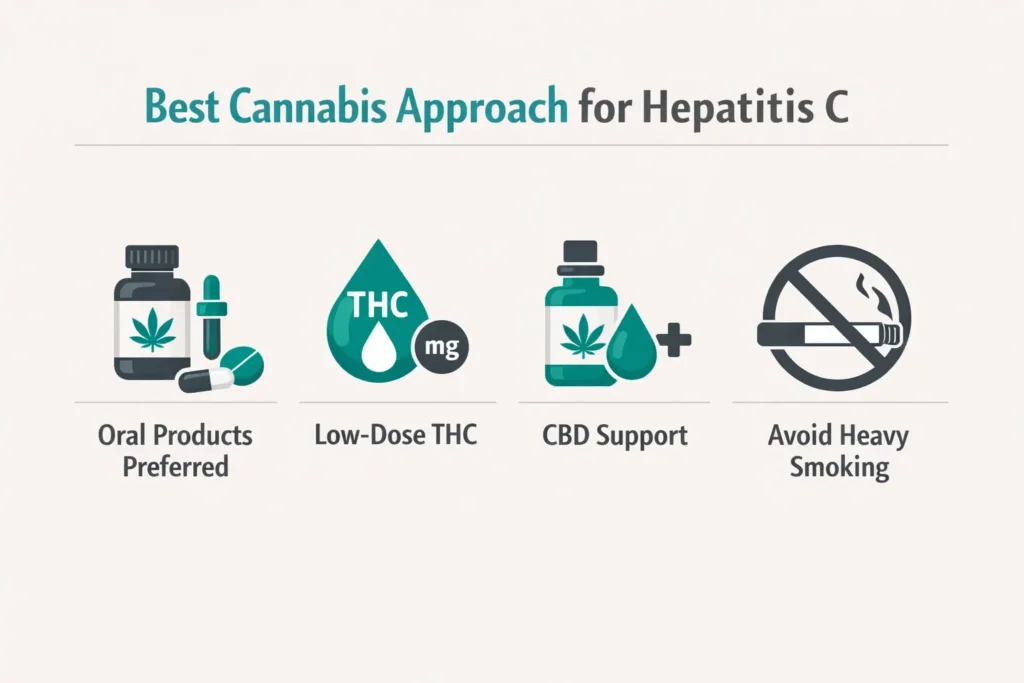
For patients on treatment (particularly ribavirin-containing regimens): Oral cannabis products — tinctures, capsules, or soft gels — are the most appropriate route. They provide consistent dosing for nausea and appetite management, avoid combustion products, and are easier to time around medication schedules. Starting doses should be low: 2.5–5mg THC equivalent with moderate to high CBD ratios. The goal is to manage nausea, stimulate appetite, and improve sleep without excessive psychoactive effects that could interfere with daily function during treatment.
For patients managing HCV symptoms without active treatment (chronic infection, or post-SVR residual symptoms): The product approach depends on the dominant symptom. For fatigue and cognitive fog: CBD-dominant products during the day. For pain: balanced THC:CBD oral products or low-dose THC tinctures. For sleep disruption: moderate THC oral products 1–2 hours before bedtime.
Products to approach with caution: High-potency smoked flower (20%+ THC) and combusted cannabis products present an additional concern for HCV patients given the theoretical liver concerns associated with heavy smoking. Vaporized flower reduces combustion products but does not eliminate them entirely. Oral products are cleanest from a liver-safety standpoint.
Tell the dispensary pharmacist: “I have hepatitis C and I’m looking for products to help with [specific symptom: nausea / fatigue / pain / sleep]. I need something I can use orally. What are your lowest-dose oral options?”
How to Get Your PA MMJ Card for Hepatitis C
Step 1 — Documentation
Gather recent medical records showing your HCV diagnosis. This can include a positive HCV RNA test result, recent HCV specialist notes, or records from a gastroenterologist or hepatologist confirming chronic HCV infection. If your HCV has been cured (SVR) but you have ongoing symptoms from liver damage or cirrhosis, bring documentation of your liver disease status.
Step 2 — Telehealth certification appointment
Schedule with a PA DOH-registered medical marijuana physician. The appointment takes 10–15 minutes. Be prepared to describe your HCV history, current treatment status, and the specific symptoms you’re seeking to address with cannabis.
Step 3 — State registration
Register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com) using your certification, a valid PA driver’s license or state-issued ID, and the $50 annual registration fee. Fee waivers are available for Medicaid, PACE/PACENET, CHIP, SNAP, or WIC enrollees.
Step 4 — Dispensary visit
Bring your PA MMJ card to any Pennsylvania dispensary. Tell the pharmacist your specific symptoms and that you have a liver condition — this is relevant to their product recommendations. Ask specifically about oral products and low-to-moderate THC:CBD ratio options.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Anxiety Disorder
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: I was cured of hepatitis C (achieved SVR). Can I still get a PA MMJ card for HCV?
Q: Is cannabis safe to use if I still have active hepatitis C and liver fibrosis?
Q: Can cannabis cure or treat hepatitis C directly?
Q: My hepatitis C is being managed with Mavyret (glecaprevir/pibrentasvir) — is it safe to add cannabis?
Q: I have cirrhosis from hepatitis C. Does that change how I should use cannabis?
HCV Resources in Pennsylvania
Pennsylvania Hepatitis Coalition (pahep.org) connects Pennsylvanians with hepatitis C testing, treatment referrals, and support services throughout the Commonwealth.
Pennsylvania Department of Health – Viral Hepatitis Program provides information on testing, treatment access, and resources for Pennsylvanians living with hepatitis C.
Hep Free PA (hepfreepa.org) — Pennsylvania’s program working to eliminate viral hepatitis through testing, linkage to care, and treatment access advocacy.
HRSA – Find a Health Center (findahealthcenter.hrsa.gov) — federally qualified health centers offer low-cost and sliding-scale HCV testing and treatment, including DAA therapy, for uninsured or underinsured patients.
National Association of Free and Charitable Clinics (nafcclinics.org) — can help uninsured patients find low-cost clinical care for hepatitis C management.
Chronic hepatitis C sits in an unusual position among Pennsylvania’s qualifying conditions: it is one of the few conditions for which an effective cure now exists — yet millions of Americans still live with untreated or treatment-resistant infection, and millions more who were cured carry lasting consequences of the virus. Pennsylvania’s decision to add it to the qualifying list in 2022 reflects the real and ongoing burden of HCV on patients’ quality of life, whether from the disease itself, from treatment, or from its aftermath.
Cannabis cannot cure hepatitis C. What it can do is meaningfully reduce the fatigue, nausea, pain, appetite loss, and sleep disruption that make this condition — and its treatment — so difficult to endure. For patients on interferon-based regimens where treatment completion directly determines cure outcomes, helping patients stay on therapy may be its most clinically significant contribution.
Used thoughtfully, at moderate doses, via oral administration, in communication with your treating hepatologist, cannabis represents a legitimate adjunct in the management of chronic HCV. The PA MMJ card is the legal pathway to accessing it.