
Glaucoma holds a unique place in the history of medical cannabis. It was one of the first documented medical uses of marijuana, a glaucoma patient in the early 1970s noticed that smoking cannabis made the halos around lights disappear, a symptom of elevated eye pressure, and successfully petitioned the courts to use it legally. That case sparked decades of research, and glaucoma became a founding qualifying condition in medical marijuana programs across the country, including Pennsylvania’s.
But the relationship between cannabis and glaucoma is more complicated than most medical marijuana websites acknowledge. The science has moved significantly since those early 1970s studies, and any patient or caregiver making decisions about glaucoma care needs to understand both what cannabis can and cannot do, including a finding about one particular cannabinoid that actively surprises most patients.
This page gives you the full picture: What qualifies in Pennsylvania, what the research actually shows, the critical practical limitations that the American Academy of Ophthalmology and the American Glaucoma Society have documented, the emerging science that may point toward a different cannabinoid future for glaucoma, and how to get your PA MMJ card if you decide to pursue it.
Does Glaucoma Qualify for Medical Marijuana in Pennsylvania?
Yes. Glaucoma is an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016) and is recognized by the Pennsylvania Department of Health for patients of all ages. A confirmed glaucoma diagnosis of any type qualifies, open-angle glaucoma (the most common form), normal-tension glaucoma, angle-closure glaucoma, secondary glaucomas, and pediatric glaucoma all fall within the condition’s scope.
There is no requirement that glaucoma be advanced, that standard medications have failed, or that a specific IOP threshold be met. A confirmed diagnosis is sufficient.
- Source: Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Source: Pennsylvania Medical Marijuana Act – Act 16 of 2016
What Is Glaucoma?
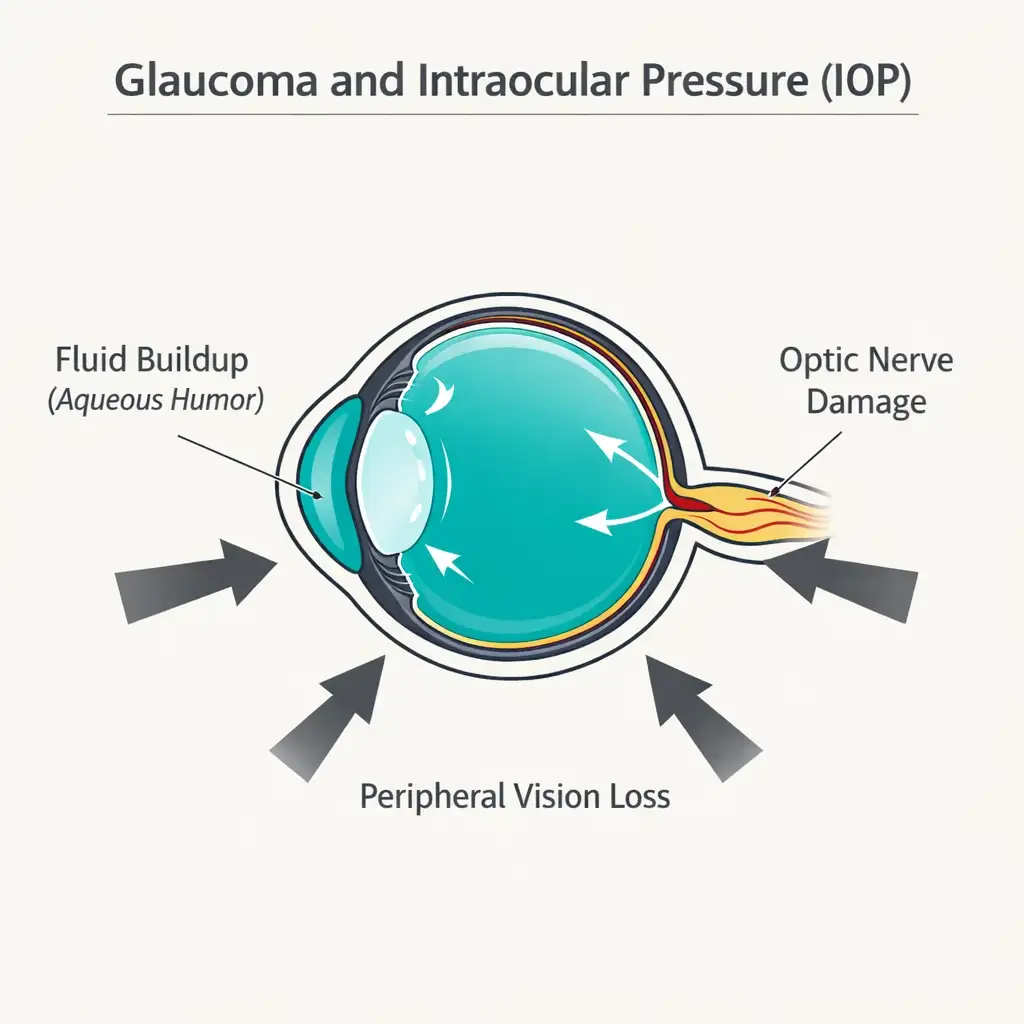
Glaucoma is a group of progressive optic neuropathies, diseases that damage the optic nerve, that together represent the world’s leading cause of irreversible blindness, affecting more than 60 million people globally. In the United States, it affects over 4 million people, with millions more undiagnosed.
The most common form, primary open-angle glaucoma (POAG), develops when the drainage channels of the eye become less efficient over time, causing intraocular pressure (IOP) to rise. This elevated pressure compresses and damages the optic nerve, producing gradual peripheral (side) vision loss that the patient often doesn’t notice until significant damage has occurred. By the time central vision is affected, substantial irreversible harm has been done.
Intraocular pressure (IOP) is the only modifiable risk factor currently validated for glaucoma treatment. Every approved glaucoma medication, laser procedure, and surgery works by reducing IOP. No treatment currently approved for clinical use has demonstrated neuroprotection, direct protection of the retinal ganglion cells in a definitive human trial.
This distinction between IOP reduction and neuroprotection is central to understanding where cannabis research stands today for glaucoma.
The Cannabis-Glaucoma Story: Where It Started and Where It Actually Stands
The Original Finding — 1971
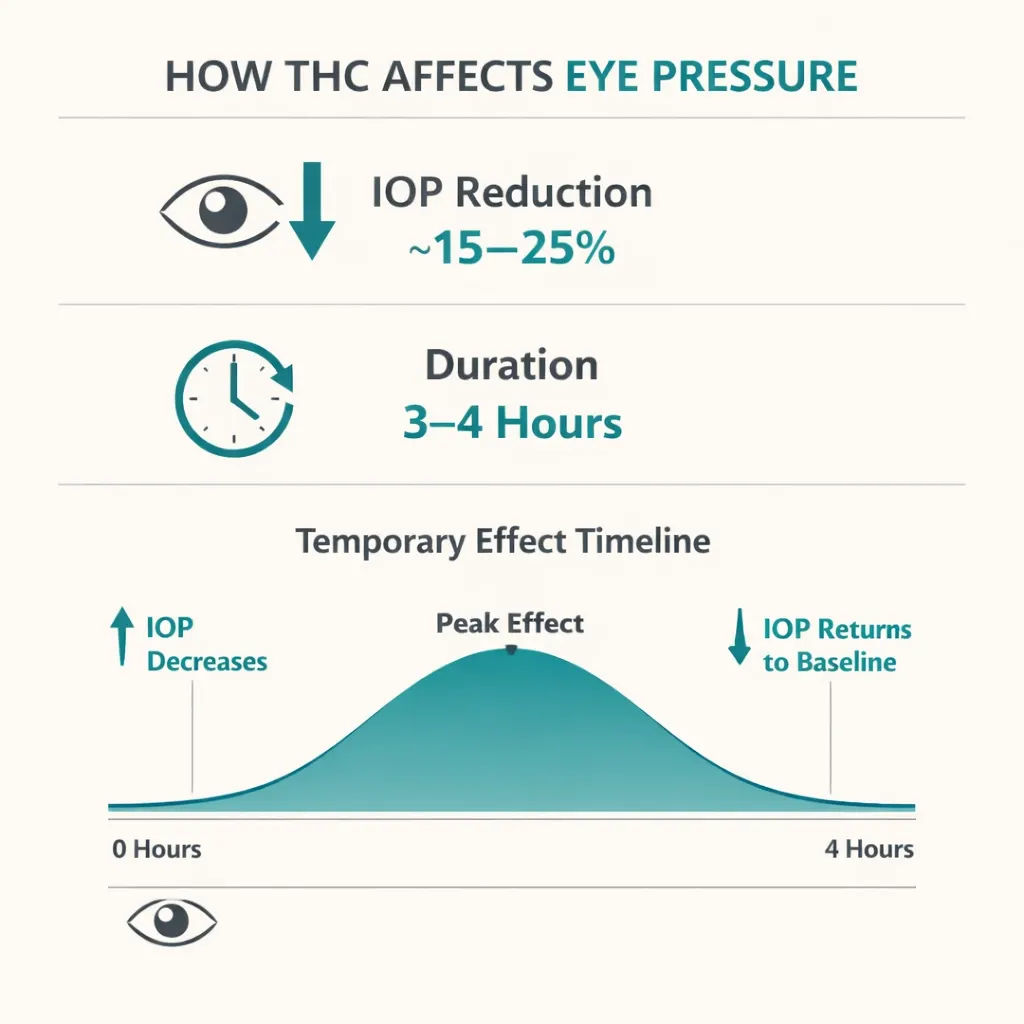
In 1971, Hepler and Frank published a landmark observation in JAMA: marijuana smoking reduced intraocular pressure in their subjects. The reduction was roughly 25% and lasted 2–4 hours. This was genuinely exciting at a time when available glaucoma medications had significant side effect profiles and the idea of a plant-based IOP-lowering agent seemed promising.
Subsequent studies through the 1970s and early 1980s confirmed that systemically administered THC, smoked, eaten, or given intravenously, reduces IOP in both glaucoma patients and people with normal IOP. The IOP-lowering effect is real and reproducible.
The Problem That Never Got Solved: Duration
Here is where the science departed from popular belief, and where most cannabis websites still fail their readers.
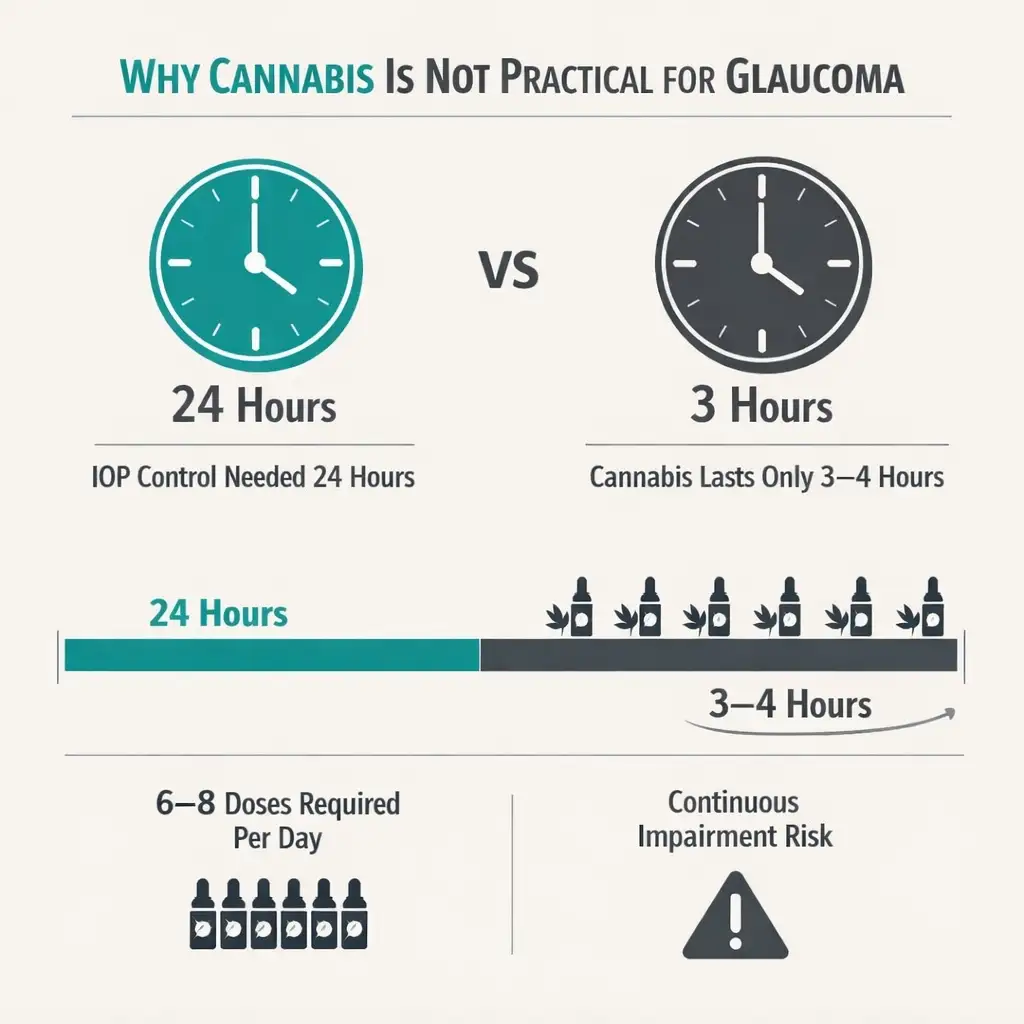
Glaucoma requires IOP control 24 hours a day, every day. The optic nerve doesn’t get a break from elevated pressure when you’re asleep. Cannabis reduces IOP for only 3–4 hours. A more recent study by Mosaed et al. (2022), the first randomized, double-blind, placebo-controlled trial of inhaled THC versus placebo, confirmed an average IOP reduction of approximately 15% lasting an average of 3 hours, consistent with the 1970s data, and confirming nothing had changed regarding duration.
To maintain IOP reduction continuously using cannabis, a patient would need to consume THC-containing cannabis approximately 6–8 times every 24 hours, including through the night. The amount of THC required, estimated at 18–20 mg, 6–8 times daily, would cause constant psychoactive impairment, cardiovascular effects, and for many patients would simply be incompatible with functioning. This dosing burden is why every major ophthalmology organization concluded that cannabis is not a practical primary treatment for glaucoma.
As glaucoma specialist Craig Chaya, MD, of the Moran Eye Center put it directly: “Glaucoma needs to be treated 24 hours a day, so you would need to smoke marijuana six to eight times a day, around the clock, to get the benefit of a consistently lowered IOP. Smoking that much marijuana would leave you unable to function normally.”
- Source: University of Utah Health – Glaucoma and Cannabis: What Ophthalmologists Want You to Know (2025)
- Source: Review of Ophthalmology – Cannabis, Glaucoma and Intraocular Pressure
- Source: NCBI Bookshelf / StatPearls – Cannabis Use for Glaucoma and Associated Pain (Updated 2023)
The CBD Paradox: Why the Most Popular Cannabinoid May Actually Harm Glaucoma
This is the finding that most surprises glaucoma patients and the one most completely absent from competing medical marijuana websites.
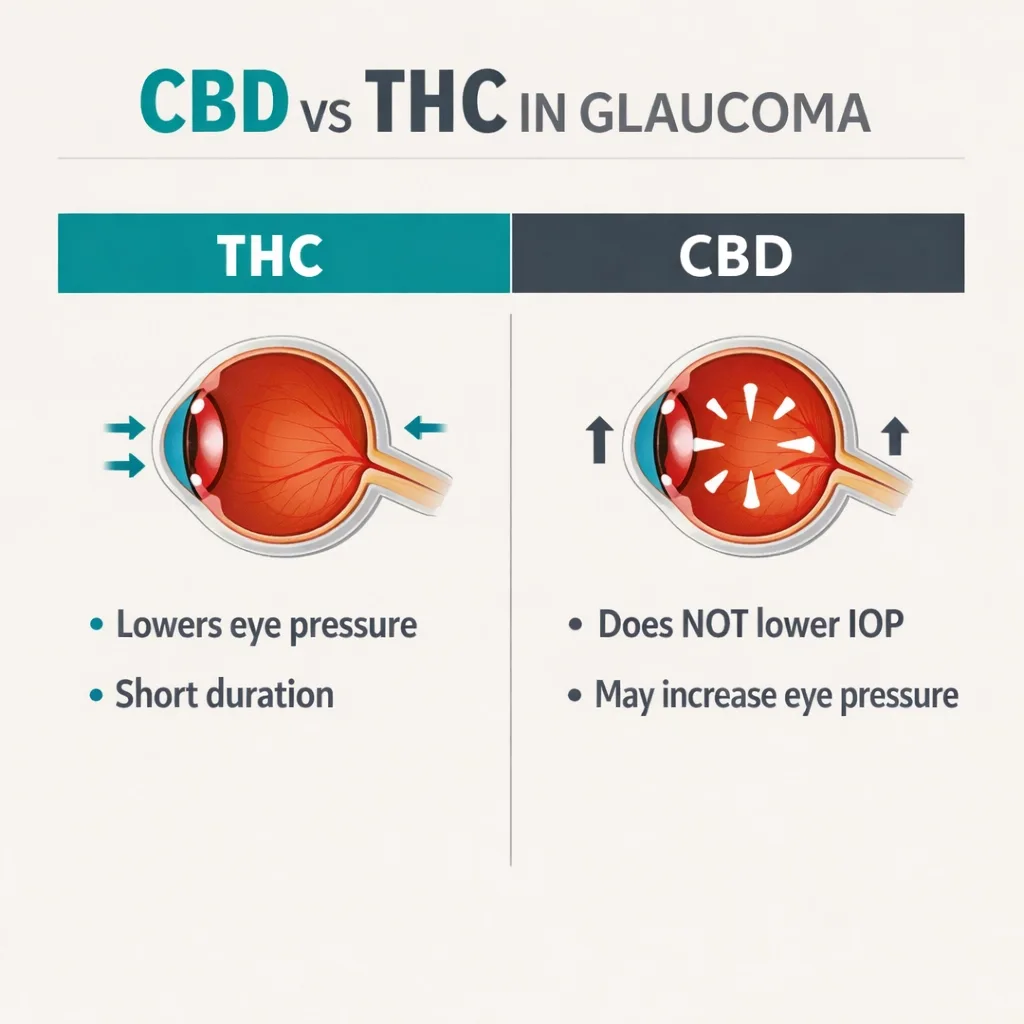
CBD (cannabidiol) does not lower IOP in glaucoma. At higher doses, it may raise it.
This is not a theoretical concern. A pivotal randomized, double-masked, placebo-controlled crossover study (Tomida et al.) in six patients with ocular hypertension or mild POAG tested sublingual THC, low-dose CBD (20 mg), high-dose CBD (40 mg), and placebo after a washout of their usual medications. Results: THC produced a modest decrease in IOP. The high dose of CBD produced a slight increase in IOP.
This finding is supported by basic science. A 2018 study by Miller et al. in live mice tested topical THC and CBD on IOP. THC lowered IOP for 8 hours. CBD produced a substantial increase in IOP. When CB1 knockout mice were tested, CBD’s IOP-raising effect was absent, suggesting CBD acts as an antagonist to the CB1 receptor that THC activates for IOP reduction. When THC and CBD were applied simultaneously, their effects cancelled each other out, neither lowering nor raising IOP meaningfully.
What this means in practice: balanced THC:CBD products (1:1 ratio) and CBD-dominant formulations are not appropriate for glaucoma IOP management. The CBD component may neutralize or reverse the THC component’s IOP-lowering effect. For a glaucoma patient hoping cannabis will help manage eye pressure, product selection matters enormously and CBD-dominant products work against that goal.
The American Academy of Ophthalmology’s current position explicitly states: “Just like cannabis that’s smoked or eaten, there is no compelling research that shows CBD to be an effective treatment for glaucoma. In fact, one recent study showed that CBD may actually increase eye pressure, which could make glaucoma worse.”
- Source: American Academy of Ophthalmology – Does Marijuana Help Treat Glaucoma?
- Source: Glaucoma Today – Cannabis and Glaucoma (2020)
- Source: PMC – Cannabinoids for the Treatment of Glaucoma: A Review (Med Cannabis Cannabinoids, 2024)
The Systemic Hypotension Concern: A Risk Specific to Glaucoma
A third clinical concern goes beyond the IOP duration limitation and the CBD paradox and is specific to glaucoma in a way that doesn’t apply to most other qualifying conditions.
Cannabis lowers blood pressure systemically. In most patients, this is either neutral or potentially beneficial. In glaucoma patients, it is concerning.
The optic nerve in glaucoma is already compromised and depends on adequate blood flow for the oxygen and nutrients it needs to survive. Optic nerve perfusion pressure is the difference between blood pressure and IOP. If THC lowers IOP while also lowering blood pressure, the net effect on optic nerve perfusion may be neutral or even harmful, the optic nerve could receive less blood flow even as the eye pressure drops.
A 2023 review in Pharmaceutical Medicine and Cannabis and Cannabinoids noted this concern directly: systemic hypotension from cannabis could lead to decreased ocular perfusion pressure, potentially accelerating progressive glaucomatous damage. The American Glaucoma Society’s position statement specifically lists decreased blood pressure as one of the adverse effects that “preclude recommending this drug in any form for the treatment of glaucoma.”
This does not mean every glaucoma patient who uses cannabis is harming themselves. It means that for a condition where optic nerve blood flow is already at stake, adding a substance that lowers blood pressure warrants explicit discussion with the treating ophthalmologist.
- Source: American Glaucoma Society Position Statement – Marijuana and the Treatment of Glaucoma
- Source: MDPI Pharmaceuticals – Therapeutic Potential of Cannabinoids in Glaucoma (2023)
What Both Major Ophthalmology Organizations Say

The two most authoritative bodies in ophthalmology hold clear, current positions on cannabis and glaucoma:
American Academy of Ophthalmology (AAO): “Cannabis, CBD and other marijuana derivatives are not a practical treatment for glaucoma or any eye condition. The American Academy of Ophthalmology does not recommend marijuana or other cannabis products for treatment of glaucoma.”
American Glaucoma Society (AGS): “Although marijuana can lower the intraocular pressure, its side effects and short duration of action, coupled with a lack of evidence that its use alters the course of glaucoma, preclude recommending this drug in any form for the treatment of glaucoma at the present time.”
Note carefully the language in the AGS statement: “lack of evidence that its use alters the course of glaucoma.” This is not just about IOP reduction, it is about whether cannabis actually slows optic nerve damage, prevents vision loss, or changes the disease trajectory. That evidence does not currently exist.
- Source: AAO – Does Marijuana Help Treat Glaucoma? (2026 updated)
- Source: AGS – Position Statement: Marijuana and the Treatment of Glaucoma
So Why Is Glaucoma Still on Pennsylvania’s Qualifying List?
This is a legitimate question that deserves a direct answer.
Glaucoma was included in Pennsylvania’s Medical Marijuana Act from the beginning, as it was in most early state MMJ programs, based on the longstanding evidence that THC does lower IOP, even if transiently. Pennsylvania’s legislature recognized that patients have the right to try a therapy with documented pharmacological activity for their condition, even if that therapy has practical limitations compared to conventional medications.
There are also circumstances where cannabis may be a reasonable adjunctive option for some glaucoma patients despite its limitations:
- Patients with intractable glaucoma whose IOP is not controlled by standard medications or surgical approaches, and who are willing to accept the dosing frequency
- Patients with glaucoma-related pain (particularly in advanced or terminal glaucoma) where cannabis’s analgesic properties are relevant
- Patients whose primary burden is anxiety about vision loss or glaucoma-related sleep disruption, where CBD-dominant products for anxiety/sleep may be appropriate as long as the patient understands the IOP considerations
- Patients in palliative or advanced-disease contexts where quality of life rather than disease modification is the goal
For all of these cases, the PA MMJ card provides legal access to a range of cannabis products and the practical question becomes less about treating glaucoma and more about treating the patient.
The Emerging Science: Cannabinol (CBN) and Why the Future Looks Different
While systemic THC from dispensary cannabis has significant practical barriers as a glaucoma treatment, the broader cannabinoid pharmacology research is pointing toward more promising directions and this is worth understanding even if it doesn’t affect your PA MMJ card decision today.
Cannabinol (CBN) – a lesser-known, non-intoxicating cannabinoid, has produced the most interesting recent preclinical results in glaucoma. Unlike THC (which requires frequent dosing and produces psychoactive effects) and CBD (which may raise IOP), CBN has shown:
- Direct IOP-lowering effects in animal glaucoma models via intravitreal administration
- Direct neuroprotection of retinal ganglion cells — protecting the actual cells that glaucoma kills, in both in vitro and in vivo models
- A potentially longer therapeutic window than THC
- Non-intoxicating properties, removing the psychoactive barrier
A 2022 study by InMed Pharmaceuticals in collaboration with the University of British Columbia, published in Molecular Genetics and Metabolism, demonstrated that CBN in a topical eye drop formulation reduced IOP and improved retinal function (pattern electroretinogram amplitudes) in a rat glaucoma model. This is the first cannabinoid ever to show both IOP reduction and direct retinal ganglion cell neuroprotection, a combination that existing glaucoma medications do not offer.
A clinical drug development program for a CBN-based topical eye drop (INM-088) was reported as being in development. As of the current evidence base, this research remains preclinical and not yet in human trials, but it represents a genuinely different therapeutic approach from smoked or ingested cannabis.
This is not a reason to delay treating your glaucoma or to rely on PA dispensary cannabis for optic nerve protection today. It is a reason to follow the research space, and a reminder that the story of cannabinoids and glaucoma is not finished.
- Source: ScienceDirect – Cannabinol Modulates Neuroprotection and Intraocular Pressure: A Potential Multi-Target Therapeutic Intervention for Glaucoma (2022)
- Source: Ophthalmology Times – Cannabinol, a Rare Cannabinoid, Shows Unique Therapeutic Potential in Glaucoma
- Source: MDPI Pharmaceuticals – Therapeutic Potential of Cannabinoids in Glaucoma (2023)
What This Means for PA Dispensary Product Selection
If you choose to pursue a PA MMJ card for glaucoma, the practical guidance on product selection follows directly from the science:
THC-dominant products — if the goal is IOP reduction (with full understanding of limitations): Oral tinctures or capsules dosed approximately every 3–4 hours provide the most consistent blood levels. Vaporized forms have faster onset but shorter duration. The fundamental limitation remains: sustained IOP control requires very frequent dosing. This approach should be discussed with your ophthalmologist, who should know you’re using cannabis alongside prescribed glaucoma medications.
CBD-dominant or balanced products — NOT for IOP management: Based on the current evidence, CBD does not lower IOP and may raise it. If your reason for using cannabis is glaucoma IOP control, CBD-dominant products work against that goal. However, if your reason for using cannabis is anxiety, sleep disruption, or pain related to your glaucoma diagnosis, separate from IOP management, CBD-dominant products may be appropriate for those secondary targets.
Do not replace prescribed glaucoma medications with cannabis. This point cannot be stated firmly enough. Stopping an effective IOP-lowering eye drop in favor of cannabis that provides 3–4 hours of IOP reduction and then wears off puts the optic nerve at risk during the hours of uncontrolled pressure. Any changes to your glaucoma medication regimen require your ophthalmologist’s involvement.
Tell your ophthalmologist you’re using cannabis. IOP measurement at your glaucoma appointment may be temporarily lower than usual if you used cannabis within 24 hours of the visit. A 2023 survey study at the University of Minnesota found that glaucoma patients who used cannabis within 24 hours were significantly more likely to know that marijuana lowers IOP, but were also creating a scenario where their ophthalmologist might be measuring artificially reduced IOP, potentially missing inadequately controlled disease.
- Source: PubMed – Assessment of Cannabis Use in Eye Clinic Patients: Implications for Glaucoma Diagnosis and Management (2025)
- Source: PA DOH – Approved Forms of Medical Marijuana
How to Get Your Pennsylvania Medical Marijuana Card for Glaucoma
Step 1 — Inform Your Ophthalmologist First
Before getting a PA MMJ card for glaucoma, tell your treating ophthalmologist. This serves two practical purposes: they can advise on interaction with your current glaucoma medications, and they know to interpret your IOP measurements with awareness of recent cannabis use. This is particularly important if you use IOP monitoring as your primary disease management metric.
Step 2 — Physician Certification (Telehealth)
Schedule a telehealth appointment with a PA DOH-registered medical marijuana physician. The evaluation typically takes 10–15 minutes. The certifying physician will confirm your glaucoma diagnosis and discuss the symptoms you’re hoping to address. Have your current glaucoma medication list available, this includes eye drops, oral carbonic anhydrase inhibitors, and any surgical history.
Step 3 — State Registration
After certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com) with your certification, a valid PA driver’s license or state-issued ID, and the $50 annual fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 4 — Dispensary Visit
Tell the dispensary pharmacist that you have glaucoma and be specific about your treatment goals: IOP reduction requires THC-dominant formulations; anxiety or sleep targets require CBD-dominant formulations. Given the CBD-IOP paradox, being explicit about which symptom you’re treating helps the pharmacist make an appropriate recommendation.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Anxiety Disorder
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: My ophthalmologist said cannabis doesn’t help glaucoma. Are they right?
Q: Will CBD eye drops from a health food store help my glaucoma?
Q: I have glaucoma but my main problems are anxiety about losing my vision and poor sleep. Can cannabis help with those?
Q: I’ve heard cannabis can protect the optic nerve. Is that true?
Q: Does cannabis use before my glaucoma appointment affect my IOP reading?
Glaucoma Support Resources
Glaucoma Research Foundation (glaucoma.org) provides authoritative patient education on all forms of glaucoma, treatment options, and current research including emerging approaches. Their patient resources include a clear summary of the cannabis evidence at glaucoma.org.
American Glaucoma Society (americanglaucomasociety.net) provides the most current clinical position on cannabis and glaucoma for patients and the physicians who treat them.
American Academy of Ophthalmology – EyeSmart (aao.org/eye-health) offers patient-facing resources on glaucoma management, medications, and surgical options, including the current AAO position on cannabis.
National Eye Institute (nei.nih.gov) provides authoritative information on glaucoma epidemiology, risk factors, and treatment approaches.
Note: Glaucoma has one of the most complex evidence pictures of any qualifying condition in Pennsylvania’s medical marijuana program — a condition where the drug qualifies, where the pharmacological mechanism for IOP reduction is real and established, and where the major ophthalmology organizations simultaneously recommend against it as a primary treatment. That apparent contradiction resolves when you understand the duration problem and the CBD paradox.
For Pennsylvania glaucoma patients, the most appropriate use of a PA MMJ card is not replacing your prescribed eye drops with cannabis — it is supplementing the overall quality of life impact of a serious vision-threatening disease, with honest expectations about what cannabis will and won’t do for your optic nerve.