
Huntington’s disease is one of the cruelest diagnoses in neurology. It is inherited. It is progressive. It is fatal. And today, in 2025, there is still no treatment that stops or slows its course. Every therapy available conventional or otherwise, is aimed at managing symptoms, preserving function, and protecting quality of life for as long as possible.
Medical cannabis fits squarely within that framework. Pennsylvania recognized Huntington’s disease as a qualifying condition from the moment the Medical Marijuana Act became law in 2016 and for good reason. The science connecting the endocannabinoid system to Huntington’s pathology is among the most biologically compelling of any condition on the state’s list. The endocannabinoid system doesn’t just happen to exist in the brain; in the striatum, the region destroyed by Huntington’s, it plays a central regulatory role. And when HD takes hold, one of the first measurable neurochemical changes is a dramatic loss of cannabinoid receptors.
This page gives Huntington’s patients and caregivers the full picture: what qualifies in Pennsylvania, what the disease actually does to the brain, what the research shows cannabinoids can and cannot do, the honest state of the clinical trial evidence, emerging neuroprotection science, product guidance, and a direct path to a PA MMJ card. No overselling. No hiding the complexities. Just everything you need to make an informed decision.
Does Huntington’s Disease Qualify for Medical Marijuana in Pennsylvania?
Yes – and the biology tells you exactly why.
Huntington’s disease is an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016), as recognized by the Pennsylvania Department of Health. A confirmed diagnosis of Huntington’s disease at any stage, qualifies a patient for a PA MMJ card.
There are no additional hurdles. The qualification criteria are patient-friendly by design:
- All stages of HD qualify – from the pre-manifest phase (gene-positive, not yet symptomatic) through advanced disease
- Both adult and juvenile Huntington’s disease are covered
- There is no requirement that conventional medications have failed first
- Caregivers of HD patients who cannot manage their own medical affairs can register and obtain cannabis on their behalf
- Patients already diagnosed and on symptomatic medications can pursue a MMJ card as an adjunct to existing treatment
The confirmation you need is a formal HD diagnosis from a qualified physician. Once documented, that diagnosis is what a PA DOH-registered certifying physician will review.
Sources:
- Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Marijuana Policy Project – Pennsylvania Medical Marijuana Law Summary
What Is Huntington’s Disease? Understanding the Condition
Huntington’s disease (HD) is a rare, inherited, autosomal dominant neurodegenerative disorder. It is caused by an expansion of the CAG trinucleotide repeat in the HTT gene on chromosome 4, which produces a mutant form of the protein huntingtin that is toxic to neurons. Because it is autosomal dominant, a child of an HD-positive parent has a 50% chance of inheriting the disease.
Globally, HD affects approximately 5 to 10 people per 100,000 in Western populations. In the United States, around 30,000 people are currently living with the disease, and an estimated 200,000 more are at risk due to family history.
The disease typically manifests in adults between the ages of 30 and 50, though a juvenile form (Juvenile HD, or JHD) affects children and adolescents and tends to present differently, with rigidity and seizures rather than chorea as the dominant early features. The mean survival after symptom onset is approximately 15–20 years.
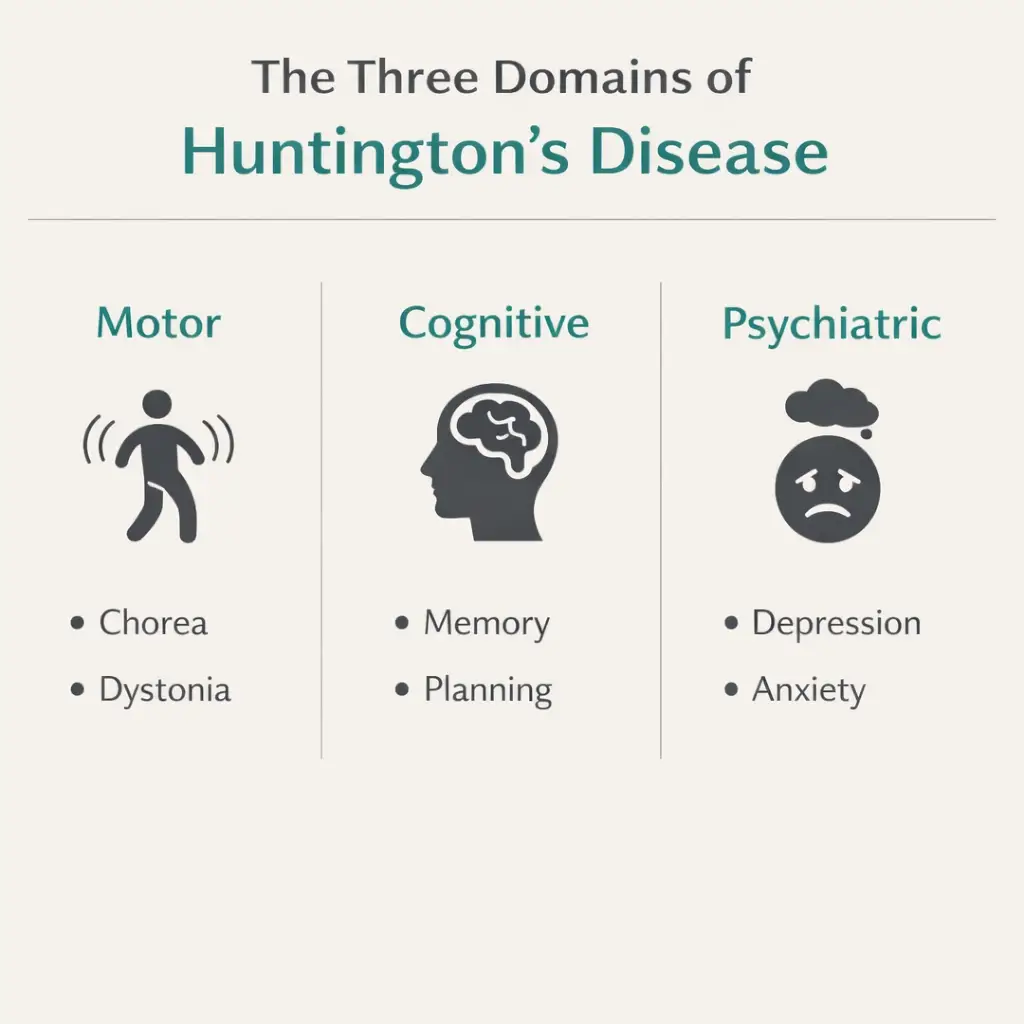
The Three Domains of Huntington’s Disease
HD affects three interconnected areas of function, all progressive and all eventually severe:
| Domain | Key Symptoms |
|---|---|
| Motor | Chorea (involuntary, dance-like movements), dystonia (abnormal posturing), bradykinesia (slowed movement), gait instability, swallowing difficulties (dysphagia), slurred speech (dysarthria) |
| Cognitive | Executive function decline, slowed processing speed, memory impairment, difficulty with planning and organization, eventually progressing to dementia |
| Psychiatric / Behavioral | Depression (affects up to 50% of patients), anxiety, irritability and apathy, obsessive-compulsive behaviors, psychosis in some patients, and significantly elevated suicide risk |
It is important to understand that HD is not just a movement disorder. The psychiatric and behavioral symptoms frequently emerge years before the motor symptoms and for many patients, they are more disabling than the physical changes. Any honest discussion of medical cannabis for Huntington’s disease must address all three domains, not just chorea.
Sources:
- NIH – National Institute of Neurological Disorders and Stroke: Huntington’s Disease
- Huntington’s Disease Society of America – About HD
- NCBI – StatPearls: Huntington Disease
The Endocannabinoid Connection: Why HD and Cannabis Are Biologically Linked
This is the section that separates a thorough Huntington’s disease page from every other PA MMJ site. The connection between HD and the endocannabinoid system is not a marketing claim, it is one of the most extensively documented neurochemical findings in HD research. Understanding it is essential to understanding why cannabis may help, and what it is realistically able to do.
What the Endocannabinoid System Does in a Healthy Brain
The endocannabinoid system (ECS) consists of two primary receptor types, CB1 and CB2 receptors, along with endogenous cannabinoids (anandamide and 2-AG) and the enzymes that produce and break them down. The ECS functions as a retrograde signaling system: it allows neurons to send feedback signals upstream to regulate the activity of the neurons that are communicating with them.
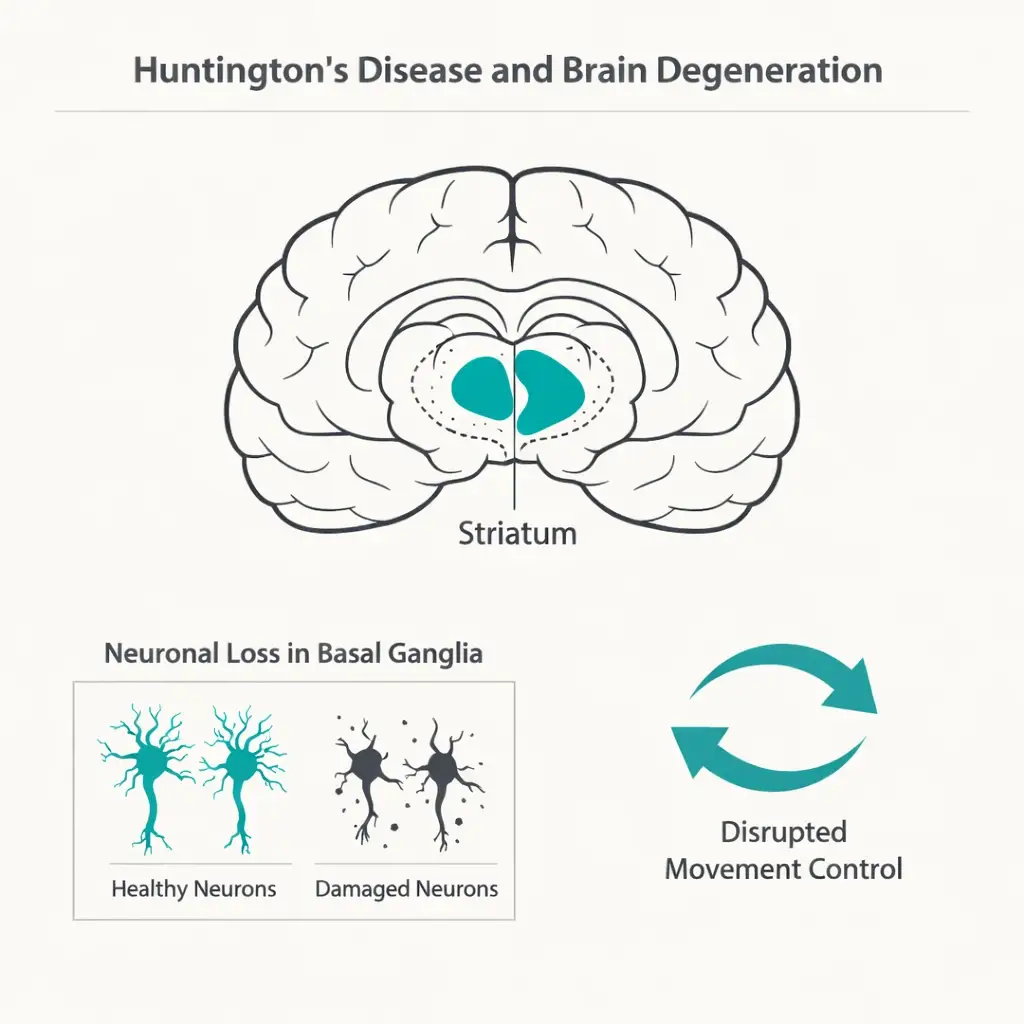
In the striatum, the brain region at the center of HD pathology, CB1 receptors are expressed at extraordinarily high density. This is not coincidental. CB1 receptors in the striatum serve a critical regulatory function: they suppress excessive glutamate release at corticostriatal synapses, acting as a natural brake against the excitotoxic neuronal death that glutamate overactivation can cause.
What Huntington’s Disease Does to the Endocannabinoid System
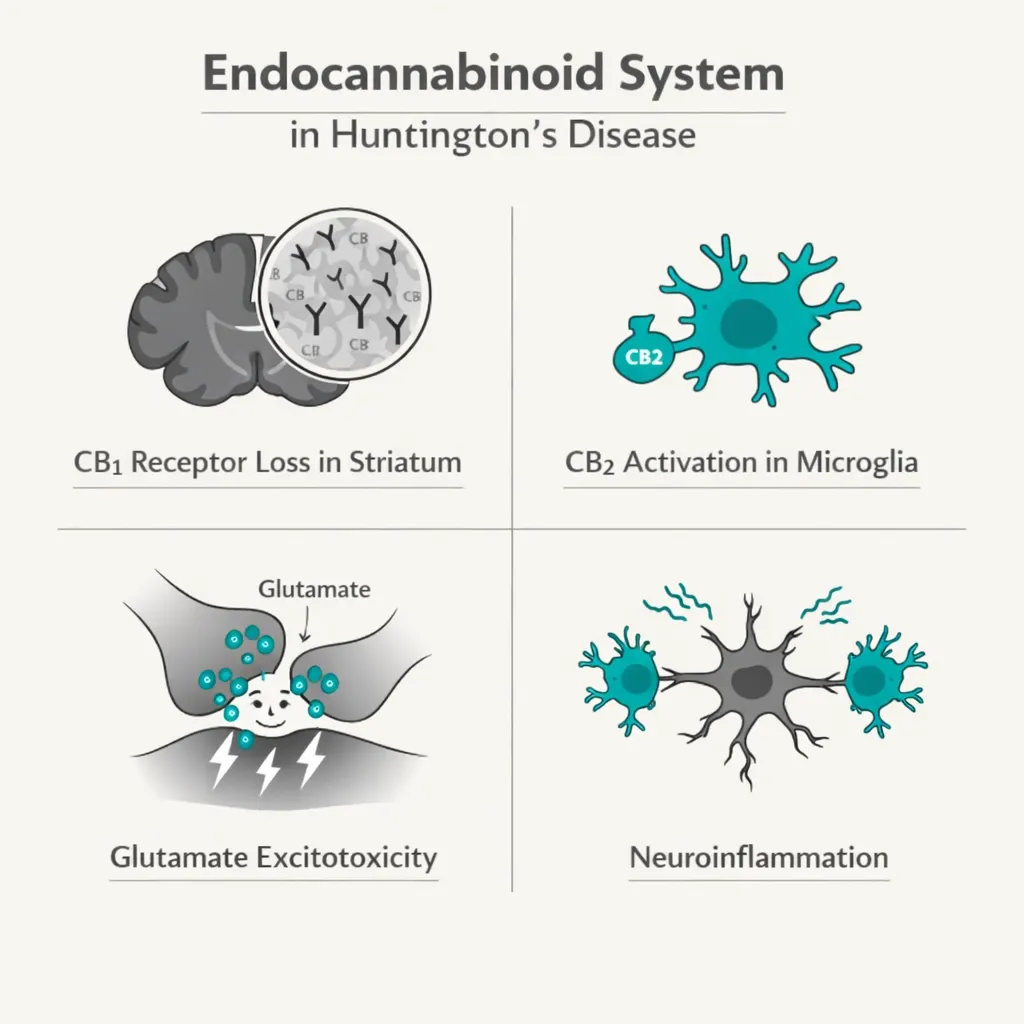
One of the earliest and most consistent neurochemical findings in HD is a profound loss of CB1 receptors in the striatum and basal ganglia. This loss occurs before other neurological changes and before motor symptoms appear, making it one of the earliest detectable biomarkers of HD progression.
Research published in leading neuroscience journals has established that this CB1 receptor loss has direct clinical consequences. The loss of CB1 signaling in corticostriatal glutamatergic projections removes the natural brake on excitotoxicity. This contributes to the runaway neuronal death that characterizes HD. Studies using mouse models in which CB1 receptors were selectively eliminated from corticostriatal neurons showed significantly worsened motor behavior compared to controls, confirming that intact CB1 signaling is neuroprotective in this circuit.
Separately, CB2 receptors — predominantly expressed on microglial cells (the brain’s immune cells) are upregulated at sites of neurodegeneration in HD. This upregulatory response appears to be a compensatory attempt by the brain’s immune system to protect damaged tissue. Activating CB2 receptors in animal models of HD has shown neuroprotective effects, reducing the inflammatory cascade that drives striatal neurodegeneration.
In short: Huntington’s disease dismantles the very system that external cannabinoids act upon. This makes the ECS one of the most scientifically rational therapeutic targets in HD research.
Sources:
- Frontiers in Computational Neuroscience – Cannabinoid Signaling and Risk in Huntington’s Disease (2022)
- PubMed – The Endocannabinoid System in Huntington’s Disease
- IntechOpen – Endocannabinoid System as a New Therapeutic Avenue for Huntington’s Disease (2022)
- Springer – Cannabinoids and Neuroprotection in Basal Ganglia Disorders
What the Clinical Research Shows: Symptom by Symptom
The clinical trial landscape for cannabinoids and Huntington’s disease is honest, limited, and genuinely interesting. No competitor page tells patients the whole story. Here it is.
Chorea — The Most-Studied Target
Chorea — the involuntary, jerking movements that are the most recognizable symptom of HD, has been the primary endpoint in most cannabinoid trials for HD. The results are mixed in a way that is scientifically instructive.
The first controlled trial of a cannabinoid in HD used CBD (10 mg/kg/day orally) in 15 neuroleptic-free patients over 6 weeks in a double-blind, crossover design. The results showed CBD was safe and well-tolerated, but produced no significant effect on chorea severity or other outcomes. This was published in 1991 by Consroe et al. and remains the foundational human trial for CBD in HD.
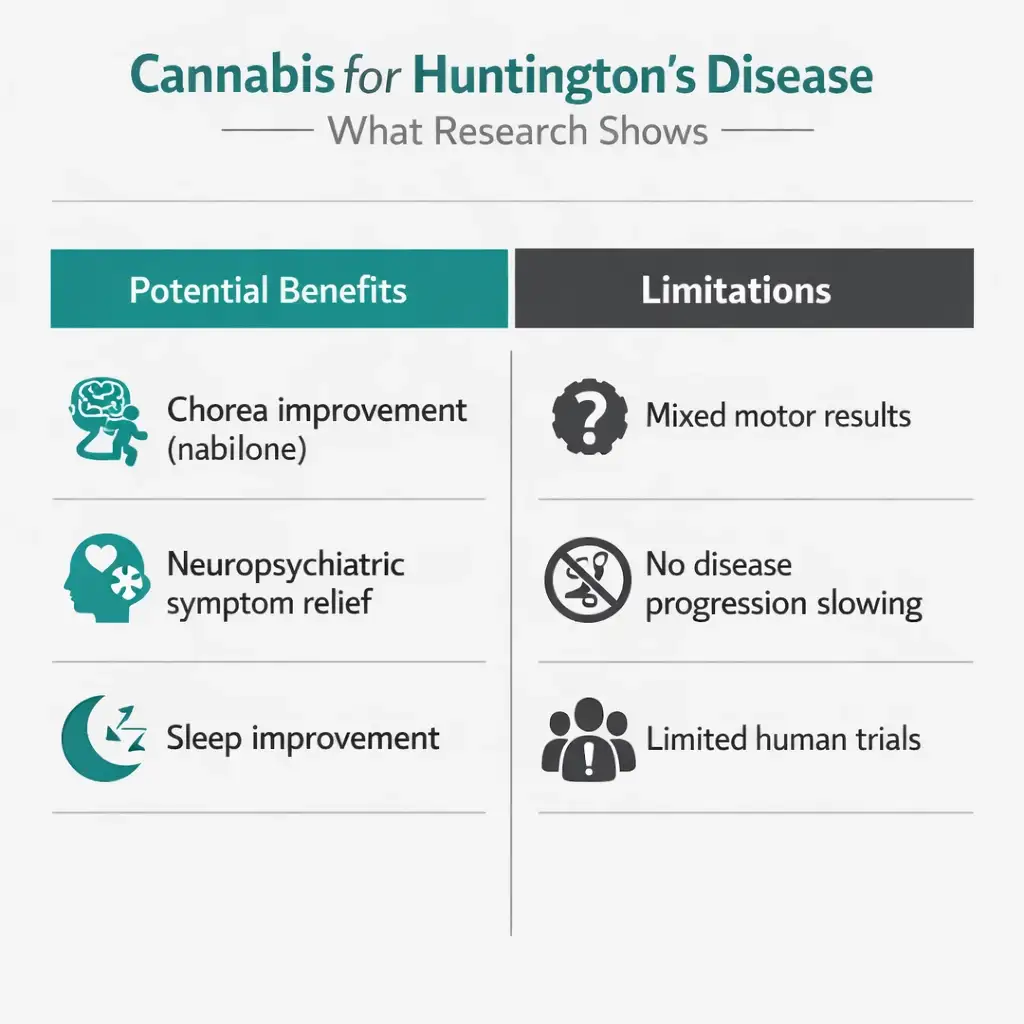
Subsequent trials turned to nabilone, a synthetic CB1 agonist similar to THC. A double-blind, randomized, placebo-controlled crossover trial (Curtis et al., 2009) administered 1–2 mg/day of nabilone to 37 HD patients across two 5-week treatment periods. The primary endpoint, total motor score on the Unified Huntington’s Disease Rating Scale (UHDRS), showed only a modest, non-statistically-significant improvement. However, two secondary endpoints did reach statistical significance: the UHDRS chorea subscale and the Neuropsychiatric Inventory (NPI) both improved meaningfully with nabilone compared to placebo. Nabilone was safe and well-tolerated, with no difference in side effects between drug and placebo groups.
In 2016, a double-blind, crossover, placebo-controlled trial used Sativex (nabiximols – an oromucosal spray delivering approximately 2.7 mg THC and 2.5 mg CBD per dose) in 24 HD patients over two 12-week periods. The trial found Sativex was safe and well-tolerated but showed no statistically significant effect on the primary motor endpoints. Notably, a separate study by Saft et al. (2018) using cannabinoids in HD patients where dystonia was the predominant symptom did observe motor score improvements, suggesting that the motor benefit profile may differ between chorea-dominant and dystonia-dominant HD.
The Honest Summary on ChoreaCBD alone did not reduce chorea in the one controlled trial to test it. THC-containing preparations (nabilone, Sativex) showed improvements on chorea subscales in some trials but not consistent results on total motor scores. The most supportive evidence is for nabilone’s effect on chorea severity and neuropsychiatric symptoms as secondary outcomes. Larger definitive trials are needed. Current evidence is preliminary, but not absent.
Sources:
- PubMed – Controlled Clinical Trial of Cannabidiol in Huntington’s Disease (Consroe et al., 1991)
- PubMed – A Pilot Study Using Nabilone for Symptomatic Treatment in Huntington’s Disease (Curtis et al., 2009)
- NORML – Huntington’s Disease Medical Marijuana Research Summary
- Fundación CANNA – Cannabinoids and Huntington’s Disease (Expert Review)
Psychiatric and Behavioral Symptoms — The Strongest Practical Case
This is where the practical, day-to-day case for cannabis in Huntington’s disease is arguably most compelling and where most PA MMJ websites say the least.
Irritability, depression, anxiety, and sleep disruption are among the most distressing and functionally limiting symptoms in HD, and they respond poorly to many conventional medications. Cannabis has well-established evidence for each of these symptom categories across a broad population, including patients with neurodegenerative diseases.
In the nabilone trial by Curtis et al. (2009), the Neuropsychiatric Inventory, which captures behavioral symptoms including agitation, irritability, anxiety, and apathy, showed statistically significant improvement with nabilone. A 2021 literature review of 22 studies assessing cannabis and cannabinoids for HD-related motor symptoms and quality of life concluded that the majority of studies showed statistically significant results favoring medical marijuana, especially for improving motor symptoms and quality of sleep.
The cannabinoid nabilone has also been studied for agitation in Alzheimer’s disease with positive results, suggesting a broader anti-agitation mechanism that is consistent with its effects in HD.
For sleep disruption specifically, THC at modest doses reliably reduces sleep onset latency and increases total sleep time. For a disease where nighttime movement symptoms, anxiety, and overall neurological burden severely disrupt sleep, this is a meaningful quality-of-life benefit.
Pain and Dystonia
Dystonia — involuntary sustained muscle contractions causing abnormal posturing, is a painful and often overlooked symptom of HD, particularly in juvenile-onset cases and in later-stage adults. Cannabinoids have established analgesic properties for musculoskeletal and neuropathic pain, and the Saft et al. (2018) study specifically reported motor score improvements in HD patients where dystonia was the dominant symptom.
For patients experiencing significant pain from HD-related muscle dysfunction, cannabis, particularly THC-containing products in moderate doses, represents a reasonable symptomatic option with a favorable side effect profile compared to opioids.
Appetite and Weight Management
Weight loss is a serious and frequently underappreciated complication of Huntington’s disease. Increased metabolic demand from continuous involuntary movements, swallowing difficulties, and anorexia combine to place HD patients at significant risk of malnutrition. Maintaining caloric intake and body weight is strongly associated with better outcomes in HD.
Cannabis is one of the most reliably appetite-stimulating substances available. THC activates the ECS pathways that stimulate hunger, a well-documented pharmacological effect. For HD patients struggling with weight maintenance, this may be among the most practically valuable effects of cannabis.
Sources:
- PMC – Endocannabinoid Modulation in Neurodegenerative Diseases: In Pursuit of Certainty (2022)
- Journal of Huntington’s Disease – Cannabinoids for Treatment of Dystonia in Huntington’s Disease (Saft et al., 2018) [via NORML]
- IntechOpen – Endocannabinoid System as a New Therapeutic Avenue for Huntington’s Disease
The Neuroprotection Question: What the Preclinical Science Shows
Beyond symptom management, there is a separate and scientifically significant question: can cannabinoids slow the progression of Huntington’s disease by protecting striatal neurons from degeneration?
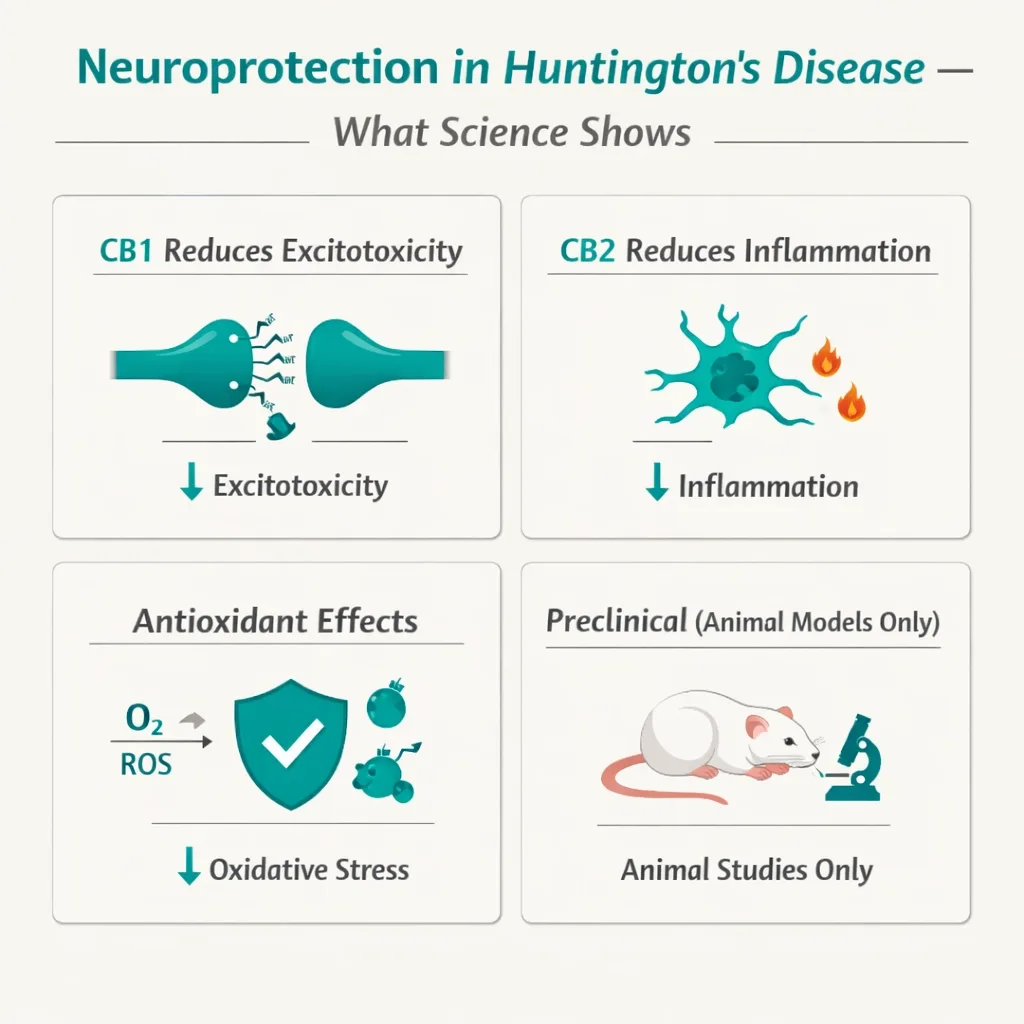
The preclinical data — from cell cultures and animal models, is genuinely encouraging. Multiple cannabinoid compounds have demonstrated neuroprotective properties in HD models through the following mechanisms:
- CB1 receptor activation on corticostriatal glutamatergic neurons suppresses excitotoxic glutamate release, protecting medium spiny neurons (the primary cell type lost in HD) from the most damaging mechanism of HD-related death
- CB2 receptor activation on microglial cells reduces neuroinflammation — the inflammatory cascade driven by activated microglia and astrocytes that accelerates neuronal loss in HD
- CBD has shown neuroprotective effects on striatal neurons in 3-nitropropionic acid (3NP) animal models of HD, specifically reversing reductions in GABA, substance P, and the antioxidant enzyme SOD-2
- Antioxidant properties of cannabinoids reduce oxidative stress, which contributes to mitochondrial dysfunction and neuronal death in HD
A 2025 review published in Exploratory Neuroprotection and Therapeutics by researchers at the University of Toronto catalogued the multilayered neuroprotective effects of cannabinoids in neurodegenerative conditions including HD, confirming that these mechanisms are well-established in preclinical models.
The Critical Limitation Every Patient Deserves to Know: No clinical trial in human HD patients has yet demonstrated that cannabis or any cannabinoid slows disease progression, protects striatal neurons, or delays cognitive or motor decline. Every neuroprotection finding is preclinical. The biological rationale is strong. The animal model data is compelling. But the human evidence for disease modification does not yet exist. This is not a reason to avoid cannabis for HD, it is a reason to understand what it currently can and cannot do.
The gap between the promising preclinical data and the underwhelming human trial results is a known problem in HD research generally, not specific to cannabinoids. HD is notoriously difficult to run clinical trials for due to the rarity of the condition, the long disease timeline, and the challenge of measuring neuroprotection in humans. This gap does not mean the preclinical findings are wrong; it means the definitive human trials have not yet been done.
Sources:
- Exploratory Neuroprotection and Therapeutics – Multilayered Neuroprotection by Cannabinoids in Neurodegenerative Diseases (2025)
- Springer Nature – Recent Advances in the Potential of Cannabinoids for Neuroprotection in Alzheimer’s, Parkinson’s, and Huntington’s Diseases
- IntechOpen – Endocannabinoid System as a New Therapeutic Avenue for Huntington’s Disease
What This Means for PA Dispensary Product Selection
The research shapes very specific product guidance for Huntington’s disease patients. This is not generic dispensary advice, it follows directly from the science.
For Chorea and Motor Symptoms
The most clinically supported cannabinoid for motor symptom management in HD is a CB1 agonist, meaning THC-containing products, not CBD alone. The nabilone trial results (the closest available data to real-world dispensary cannabis) showed improvements specifically on chorea and neuropsychiatric scales with a CB1-active compound.
Practical product guidance: Low-to-moderate dose THC-dominant oral formulations (tinctures or capsules) allow for more precise dosing and a longer duration of action than vaporized products. Starting with a low dose and titrating slowly is critical, excessive THC can worsen disorientation and coordination in HD patients who already have movement impairment.
Important caveat: The Sativex trial (a balanced THC:CBD product) did not show significant results on primary motor endpoints in one trial, while nabilone (THC-only) showed secondary endpoint improvements. This is consistent with the finding in other conditions that CBD may partially antagonize CB1-mediated effects when combined with THC at equal ratios. This does not mean balanced products are ineffective — but it suggests that for motor symptom targeting, THC-dominant formulations may be more pharmacologically aligned with the evidence.
For Psychiatric and Behavioral Symptoms
For depression, anxiety, irritability, and sleep — the behavioral symptoms that frequently precede motor symptoms and affect quality of life throughout the disease course, lower-dose THC:CBD balanced products or CBD-dominant formulations provide relief with a reduced psychoactive burden. Higher doses of THC in a population with cognitive vulnerability require caution.
For sleep specifically: a modest dose of THC (tincture or capsule) administered 1–1.5 hours before bed is well-supported for sleep onset and duration. Using the highest dose of the day at bedtime is a practical strategy consistent with clinical guidance for movement disorders.
For Appetite and Weight
THC-dominant products, particularly edibles or capsules taken before meals, provide the appetite-stimulating effect most relevant to HD-related weight management. This is a well-established pharmacological effect and one of only two indications for which the FDA has approved a synthetic THC analog (dronabinol/Marinol). For HD patients actively losing weight, this is one of the most evidence-based practical targets for cannabis.
Dosing Considerations Specific to HD
Huntington’s disease introduces specific considerations that make careful, conservative dosing especially important:
- Cognitive vulnerability: HD patients experience progressive cognitive decline. High-dose THC can exacerbate disorientation, memory impairment, and confusion. Start with the lowest effective dose and increase only as needed.
- Motor coordination: THC can temporarily worsen coordination and increase fall risk in patients already dealing with gait instability. Seated or lying administration for first doses is advisable.
- Psychiatric sensitivity: Patients with psychosis or a history of psychotic episodes — which can occur in HD — should avoid high-THC products. CBD-dominant formulations are safer for this subgroup.
- Swallowing: In later-stage HD, dysphagia (swallowing difficulty) makes oral capsules or tablets challenging. Sublingual tinctures, vaporization, or transdermal products may be better-tolerated formulations.
Always discuss product selection and dosing with both your certifying PA MMJ physician and your treating neurologist.
How to Get Your Pennsylvania Medical Marijuana Card for Huntington’s Disease
Getting your PA MMJ card is a four-step process that can be completed entirely from home. Here is exactly how it works for Huntington’s disease patients, including what your certifying physician will want to see.
Step 1 — Tell Your Neurologist
Before pursuing a PA MMJ card, inform your treating neurologist. This matters for two reasons: (1) Your neurologist manages your other HD medications, some of which interact with cannabis metabolically. They need to know to watch for changes in drug levels or symptom response. (2) Your medical records from your neurologist will confirm your HD diagnosis, which is what the certifying physician needs to review. Having your records ready shortens and simplifies your certification appointment.
Step 2 — Physician Certification (Telehealth)
Book a telehealth appointment with a PA DOH-registered medical marijuana physician. These appointments typically take 10–15 minutes and can be completed via video from your home. The physician will:
- Review your confirmed HD diagnosis (genetic confirmation, neurological assessment, or both)
- Discuss the specific symptoms you are hoping to address — motor, psychiatric, pain, sleep, or appetite
- Review your current HD medications (tetrabenazine, deutetrabenazine, antidepressants, antipsychotics, etc.)
- Provide a written certification to the PA DOH Medical Marijuana Patient Registry
✨ Ready to get certified? Book your PA MMJ telehealth appointment today.Our PA DOH-registered physicians understand Huntington’s disease and can walk you through exactly what cannabis products may help your specific symptom profile.➡ [BOOK YOUR PA MMJ CERTIFICATION HERE]
Step 3 — State Registration
After your physician certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com). You will need:
- Your physician certification
- A valid PA driver’s license or state-issued ID
- The $50 annual registration fee (fee waivers available for Medicaid, PACE/PACENET, CHIP, SNAP, or WIC recipients)
Your digital MMJ card is typically available within a few days of completing registration.
Step 4 — Dispensary Visit
When visiting a PA dispensary for the first time as an HD patient, be specific with the dispensary pharmacist about your goals. Tell them:
- You have Huntington’s disease
- Whether your primary target is motor symptoms, behavioral/psychiatric symptoms, sleep, appetite, or pain
- What your current medications are, particularly if you take tetrabenazine, deutetrabenazine, or any psychiatric medications
- Whether you have any cognitive sensitivity to THC or a history of psychosis
A knowledgeable dispensary pharmacist will recommend formulations and dose ranges appropriate for your specific symptom targets, not just the strongest or most popular product.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Anxiety Disorder
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
Frequently Asked Questions
Q: Can cannabis slow the progression of Huntington’s disease?
Q: Will cannabis worsen my cognitive symptoms?
Q: I am a caregiver for an HD patient who can no longer manage their own affairs. Can I still get them a PA MMJ card?
Q: Does cannabis interact with tetrabenazine or deutetrabenazine?
Q: I tested gene-positive for HD but do not yet have symptoms. Do I qualify?
Q: Does medical marijuana appear on standard drug tests?
Huntington’s Disease Support Resources
Living with HD — whether as a patient or a caregiver — is one of the most demanding experiences in medicine. The following organizations provide authoritative information, support, and connection to the HD community.
Huntington’s Disease Society of America (HDSA): The primary national organization for HD patients, families, and caregivers. HDSA maintains a network of HD Centers of Excellence and social workers, provides comprehensive disease education, and operates a 24/7 HD helpline. Find resources at hdsa.org.
HDSA – HD Helpline: 1-800-345-HDSA (4372) — available for patients, families, and caregivers.
HDSA Centers of Excellence: HDSA has designated Centers of Excellence across the country with multidisciplinary HD teams experienced in all three symptom domains. These are the recommended care sites for HD management, and their clinical teams are appropriate partners for discussing medical cannabis.
ENROLL-HD: The largest observational study for HD, open to HD patients, pre-manifest gene carriers, and family members. Participants contribute to research that advances treatment knowledge. Learn more at enroll-hd.org.
ClinicalTrials.gov – Huntington’s Disease: The most current listing of open HD trials, including any trials involving cannabinoids. Search at clinicaltrials.gov.
Conclusion
Huntington’s disease is one of the most scientifically justified qualifying conditions in Pennsylvania’s medical marijuana program. The endocannabinoid system is not a peripheral consideration in HD — it is one of the first neurochemical systems to be dismantled by the disease. CB1 receptor loss in the striatum is among the earliest measurable biomarkers of HD progression. The theoretical and preclinical case for cannabinoids in HD is among the strongest of any qualifying condition in the PA program.
What the human clinical evidence currently supports is more targeted: modest but real improvements in chorea and neuropsychiatric symptoms with CB1-active compounds (nabilone), well-established benefits for anxiety, sleep, appetite, and depression that are relevant to HD’s psychiatric domain, and a safety profile in HD trials that was consistently acceptable. What it does not yet support is disease modification or neuroprotection in people.
For Pennsylvania Huntington’s disease patients and their families, a PA MMJ card provides legal access to a range of products that can meaningfully reduce the symptom burden of a disease for which conventional options remain limited. That is a legitimate and valuable goal. Pursue it with accurate expectations, close coordination with your neurologist, and product choices grounded in the science outlined here.