
There is a version of your life before the trauma. And then there is this one.
Maybe it was combat. Maybe it was an assault, an accident, losing someone in a way that no one should have to witness. Maybe it was something that happened slowly over years and still lives in your body as if it was yesterday. Whatever it was, PTSD does not ask permission to stay. It shows up in your sleep, in the moments when a sound or a smell or something you cannot quite name suddenly pulls you back. It shows up as the constant alertness that never quite switches off, the exhaustion of being on guard all the time, the relationships that strain under the weight of something you cannot fully explain.
You have probably tried things that helped some. Maybe medication, maybe therapy, maybe both. And maybe you are still here, still looking — because what exists is not quite enough, or comes with its own costs, or simply does not reach the parts of PTSD that are hardest to live with.
Pennsylvania recognises PTSD as a qualifying condition under its Medical Marijuana Act. If you have a diagnosis, you have a legal path to a PA MMJ card. This page explains everything honestly — what the research actually shows, what it does not show, and how to use a PA MMJ card well if you have PTSD.
Does PTSD Qualify for a PA MMJ Card?
Yes. Post-traumatic stress disorder (PTSD) is an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016), as recognised by the Pennsylvania Department of Health.
There is no requirement that your PTSD be severe or treatment-resistant. There is no specific trauma type, no minimum duration of symptoms, no list of medications you must have tried first. A confirmed PTSD diagnosis from a licensed physician is the threshold.
PTSD is consistently among the most common qualifying conditions cited by Pennsylvania MMJ cardholders — and the evidence for why is real, though more nuanced than many cannabis websites present.
Sources:
- Pennsylvania Department of Health – Medical Marijuana Qualifying Conditions
- 28 Pa. Code Appendix A – Serious Medical Conditions
What PTSD Actually Does — And Why the Brain’s Chemistry Matters Here
PTSD is not a character flaw, not a weakness, not something you can reason your way out of. It is a disorder of fear memory — the brain’s threat-detection system getting locked in a state of high alert long after the danger has passed.
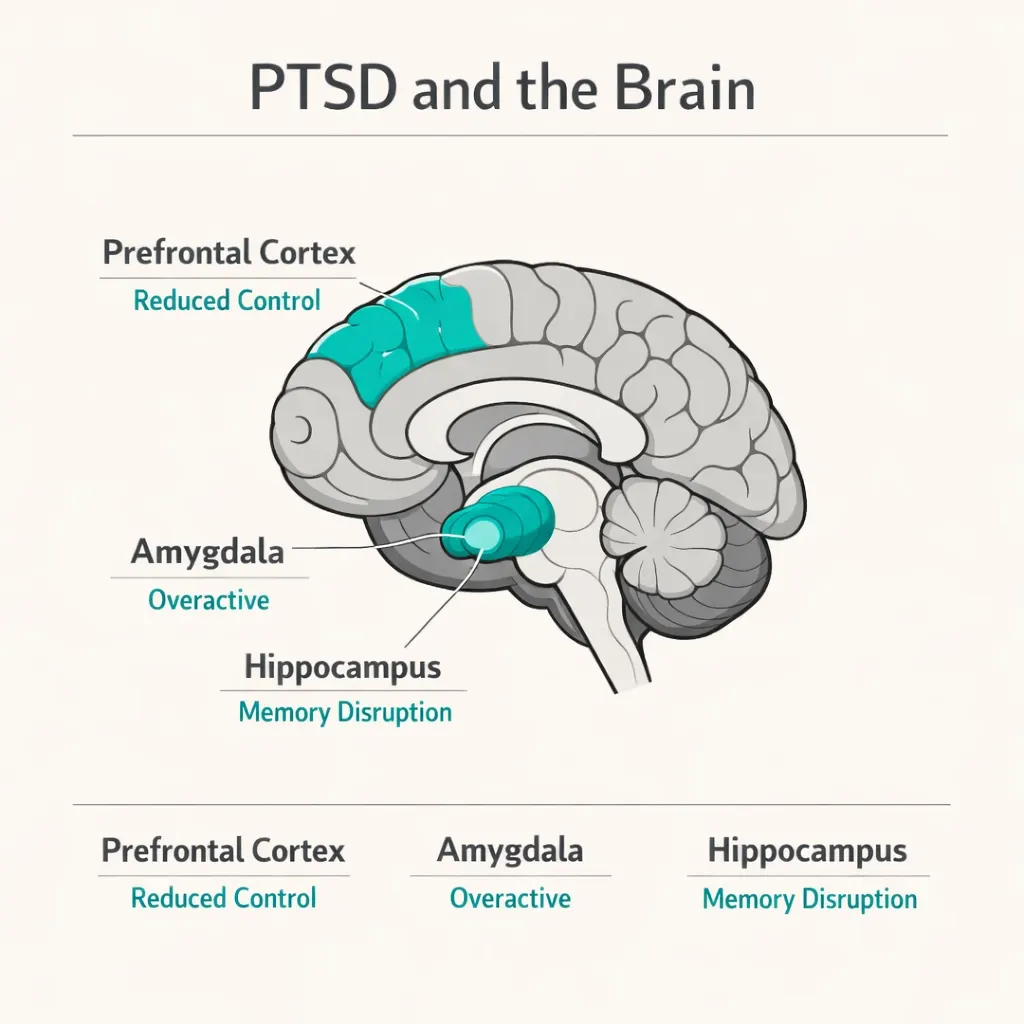
The regions most affected are the amygdala (the brain’s fear centre, which becomes hyperactive in PTSD), the prefrontal cortex (which normally regulates emotional responses but functions less effectively in PTSD), and the hippocampus (involved in memory processing and contextual learning). Together, these changes mean that traumatic memories are not processed and stored the way ordinary memories are — they intrude, they replay, they trigger fear responses that feel as immediate as the original event.
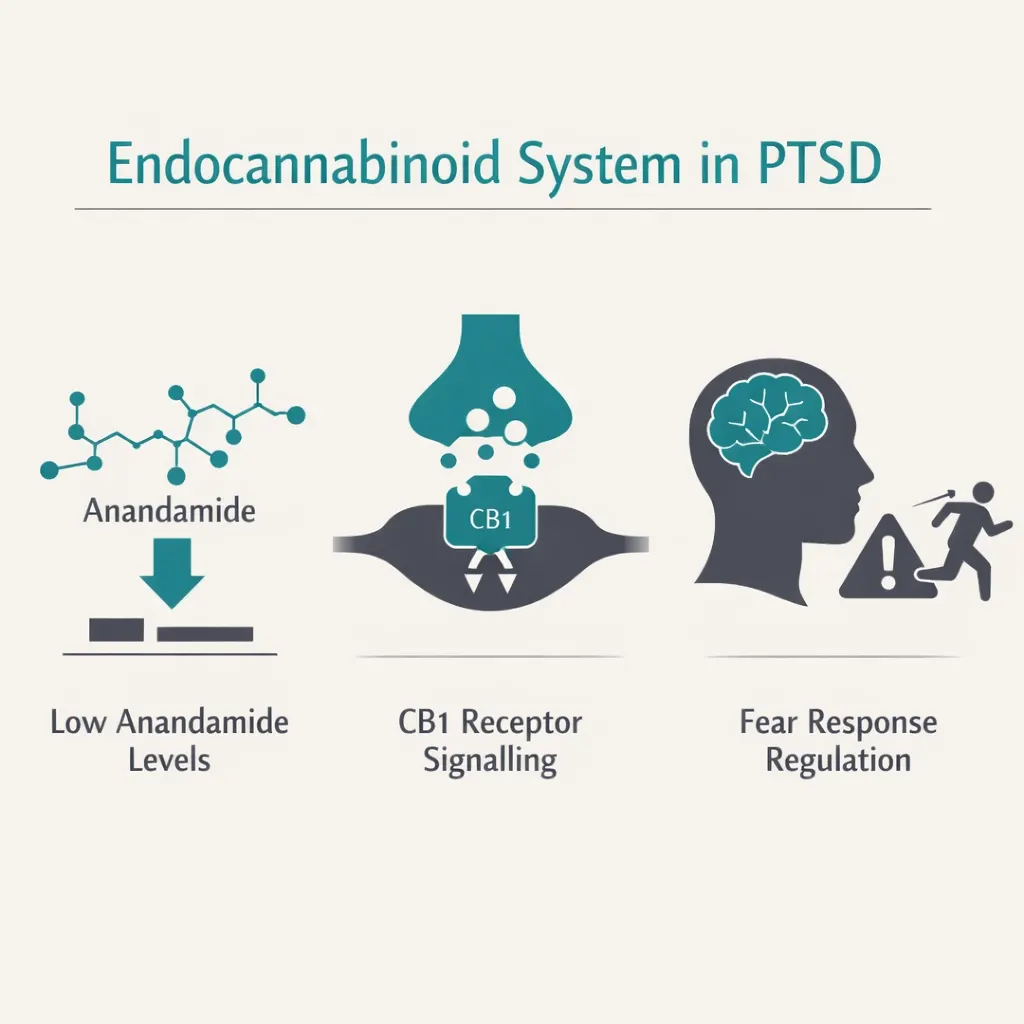
Here is why this matters for cannabis: people with PTSD show measurably lower levels of anandamide — one of the body’s own natural endocannabinoids — and altered cannabinoid receptor activity compared to trauma-exposed individuals who did not develop PTSD. A deficiency in endocannabinoid signalling appears to contribute directly to the amygdala hyperactivation, anxiety, and hyperarousal that make PTSD so hard to live with.
The endocannabinoid system is not peripheral to PTSD’s biology. It is implicated at its core. Restoring endocannabinoid tone is one of the most biologically credible reasons cannabis may help with PTSD symptoms — not just as a sedative, but as something that may interact with the actual mechanisms driving the condition.
Sources:
- Frontiers in Psychiatry – Medical Cannabis for Treatment-Resistant Combat PTSD (2023)
- PMC – Cannabis in the Management of PTSD: A Systematic Review
What the Research Shows
The Honest Picture First
The evidence for cannabis in PTSD is genuinely promising — but it is also genuinely early-stage. There are far fewer large, rigorous placebo-controlled trials for PTSD than for conditions like MS spasticity or Dravet syndrome. Much of what exists is observational data, open-label studies, and real-world registry analyses. That does not make it worthless — it makes it promising evidence that warrants access and continued research, not a definitive clinical recommendation.
The US Department of Veterans Affairs currently states that evidence is insufficient to recommend cannabis as a standard PTSD treatment. This is technically accurate. It does not mean cannabis does not help — it means the formal evidence base has not yet caught up with what hundreds of thousands of PTSD patients are already reporting.
With that context in place, here is what the research actually shows.
Nightmares — The Most Consistent Finding
If there is one PTSD symptom where the cannabis evidence is clearest and most consistent, it is nightmares.
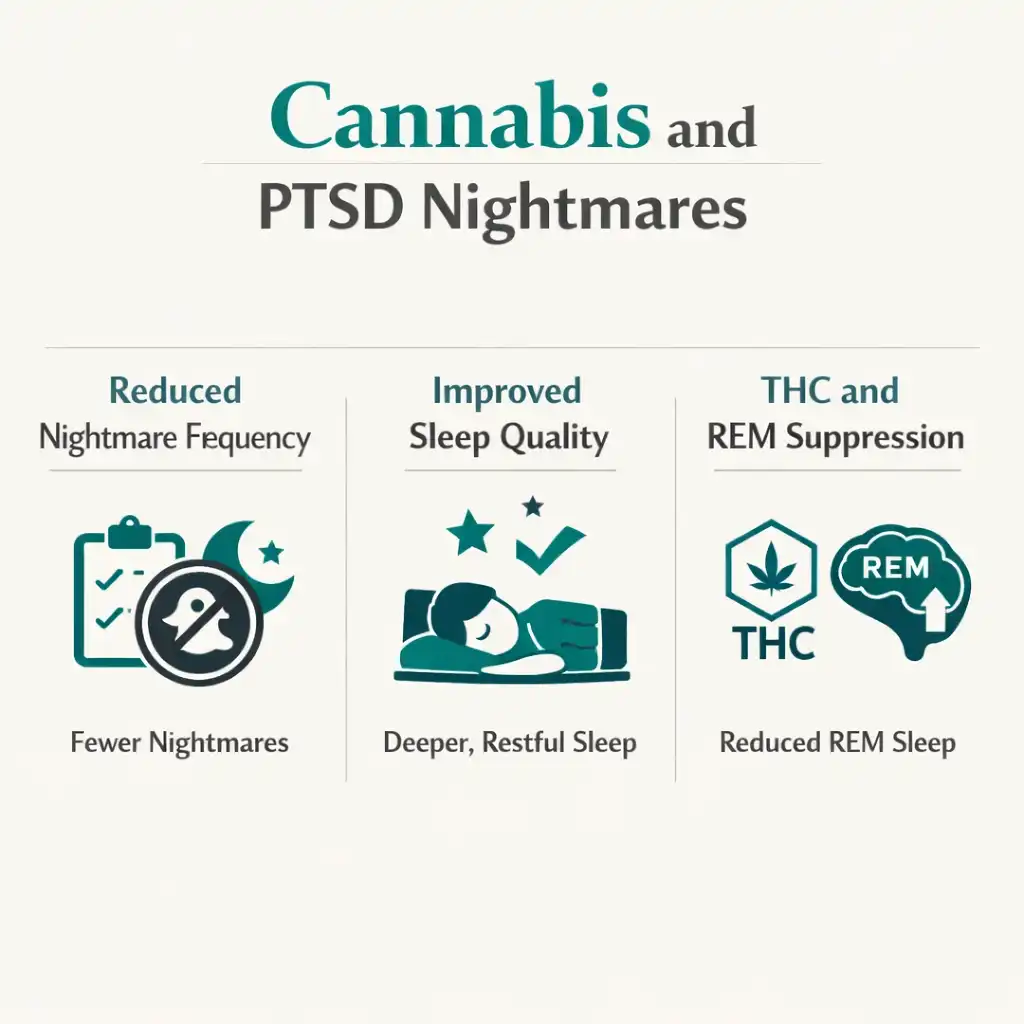
As many as 80–90% of PTSD patients experience sleep impairment, and nightmares are among the most disruptive and persistent features of the disorder. They are not just bad dreams — they are full re-experiencing events that leave you shaking, hyperaroused, and unable to get back to sleep at 3am.
Multiple studies have found that THC-based cannabinoids reduce nightmare frequency and severity in PTSD patients. An open-label study of nabilone (a synthetic THC analogue) found that 34 out of 47 PTSD patients experienced either total cessation or significant reduction in nightmares. A daily diary study of 77 licensed medical cannabis patients with PTSD found that taking cannabis closer to bedtime was associated with a significantly lower likelihood of experiencing nightmares throughout the night.
A 2023 multicenter study of combat veterans with treatment-resistant PTSD found that total sleep score, subjective sleep quality, and sleep duration all significantly improved with medical cannabis treatment (p < 0.01). Total PTSD symptom score — across intrusiveness, avoidance, and alertness — also showed improvement (p < 0.05).
For PTSD patients whose nights are dominated by traumatic nightmares, this is the most immediately practical benefit cannabis offers — and the one supported by the most consistent evidence.
Sources:
- Frontiers in Psychiatry – Medical Cannabis for Treatment-Resistant Combat PTSD (2023)
- PubMed – PTSD, Sleep and Medical Cannabis: A Daily Diary Study
- BMC Psychiatry – Treating Nightmares in PTSD with Dronabinol: Study Protocol (2023)
Hyperarousal and Anxiety
The constant alertness. The startle response that fires at nothing. The inability to feel safe even in safe places. These are hyperarousal symptoms — and they are among the most exhausting aspects of PTSD.
Open trials have found decreases in hyperarousal symptoms with cannabinoid treatment, with 50–72% of participants reporting improvement in nightmare frequency or intensity alongside hyperarousal reduction. Cannabis is theorised to reduce hyperarousal by activating CB1 receptors in the amygdala and hippocampus, dampening the threat-response circuitry that PTSD keeps stuck in overdrive.
CBD specifically has well-documented anxiolytic (anxiety-reducing) effects through its action on serotonin receptors — directly relevant for the anxiety dimension of PTSD’s hyperarousal cluster.
General PTSD Symptom Reduction
A prospective one-year study published by researchers at the University of Pennsylvania compared PTSD symptoms in dispensary cannabis users versus non-users over 12 months. Cannabis users reported a greater decrease in PTSD symptom severity over time, and were more likely to no longer meet diagnostic criteria for PTSD at the end of the study period compared to those who did not use cannabis. These results come with the caveat that this was observational, not a randomised trial — but it is real-world dispensary data, directly relevant to what PA patients experience.
An earlier observational study found that patients with PTSD who used cannabis reported greater than 75% reduction in symptom severity compared to periods when they were not using it. Again, observational — but a signal too consistent across studies to dismiss.
Sources:
- PMC – Effects of Cannabis on PTSD Recovery: Review of the Literature and Clinical Insights
- VA PTSD Research – Long-Term Prospective Study of Dispensary Cannabis and PTSD
Real-World Registry Data (UK, 2024)
A 2024 analysis from the UK’s T21 medicinal cannabis patient registry — covering PTSD patients prescribed cannabis products and followed over three months — found meaningful improvements in PTSD symptom severity, anxiety, mood, and sleep quality from baseline to follow-up. Importantly, the effectiveness of cannabis for PTSD was not impaired in patients who also had comorbid depression — which is extremely common in PTSD. For Pennsylvania patients managing both PTSD and depression, this is a meaningful finding.
An Important Nuance: Does Cannabis Help or Hinder Therapy?
This is the question that matters most for PTSD patients actively engaged in treatment — and the answer is more hopeful than many assume.
Early research raised concerns that cannabis might interfere with exposure-based therapies like Prolonged Exposure (PE) or EMDR, which rely on fear extinction processes. Some animal studies suggested THC could impair extinction learning.
However, more recent neuroimaging research found that acute low-dose THC actually increased activity in the corticolimbic regions involved in fear extinction in PTSD patients. A 2024 meta-analysis of individual patient data found that cannabis use did not impair outcomes from trauma-focused treatment for co-occurring PTSD and substance use disorders.
The picture is more nuanced than a simple “cannabis blocks therapy.” For many patients, cannabis-managed sleep and reduced hyperarousal may actually make engagement with therapy more possible — not less. This remains an active area of research, and discussing it openly with your therapist is the right approach.
What Cannabis Is — and Is Not — for PTSD
Cannabis manages PTSD symptoms. It does not process trauma. It does not replace the work of therapy — and for many people, evidence-based therapies like Prolonged Exposure, Cognitive Processing Therapy, and EMDR are the most effective tools for long-term PTSD recovery.
The most realistic and honest framing: cannabis as a symptom management tool that makes daily life more liveable — better sleep, less hyperarousal, fewer nightmares, lower anxiety — while therapy does the deeper work. These are not mutually exclusive. Many PTSD patients use both, and the evidence does not suggest they should not.
THC or CBD — What Works for PTSD?
THC is the primary driver of nightmare suppression and hyperarousal reduction. The studies showing the strongest effects on nightmares and sleep used THC or THC-based cannabinoids. This is one condition where CBD alone is not the complete answer for the most distressing symptoms.
CBD plays a critical supporting role for anxiety, emotional regulation, and the mood dimension of PTSD. CBD also moderates the psychoactive effects of THC — important because high-THC products without CBD can, paradoxically, worsen anxiety in some people. The combination appears to work better than either alone for most PTSD patients.
A balanced THC:CBD product (1:1 ratio) at low to moderate doses is the most practical starting point for most PTSD patients — particularly for evening/nighttime use to address sleep and nightmares.
One critical warning about high-THC products: At higher doses, THC can increase anxiety rather than reduce it — particularly in people new to cannabis or using it inconsistently. This is dose-dependent. The starting principle is: start very low, go very slow. 2.5–5 mg THC equivalent is a sensible starting dose for someone new to cannabis with PTSD.
PA Dispensary Product Guidance for PTSD
For Nightmares and Sleep
A low to moderate THC dose (5–10 mg) in a balanced or mild THC-dominant tincture or capsule, taken 60–90 minutes before bed, is the most evidence-aligned approach for nightmare reduction and sleep improvement. Capsules provide a more consistent slow release through the night. The daily diary research found that taking cannabis closer to bedtime — rather than earlier in the evening — was specifically associated with lower nightmare likelihood.
Higher CBD concentration in your nighttime product was associated with fewer early awakenings in the same research. A balanced 1:1 tincture or a capsule with meaningful CBD alongside THC is a good choice for this goal.
For Daytime Hyperarousal and Anxiety
CBD-dominant products (20:1 CBD:THC or higher) are more appropriate for daytime use when you need anxiety and hyperarousal relief without significant psychoactive effect. Getting high at work or while caring for children is not a functional solution. High-CBD, low-THC tinctures or capsules are practical for daytime symptom management.
For Acute Anxiety or Flashback Episodes
Some PTSD patients find low-dose sublingual THC/CBD tinctures useful for acute hyperarousal moments — the faster onset (15–30 minutes) makes them more responsive than capsules. Start very low and have a sense of your individual response before relying on this for acute episodes.
What to Avoid
Very high-THC products without CBD are the highest risk choice for PTSD. Anxiety amplification at higher THC doses is a well-documented effect — and the last thing someone in a hyperarousal state needs. Also avoid using cannabis as a way to avoid processing trauma entirely. Numbing and avoidance are already core PTSD symptoms. Cannabis that helps you function and sleep better is helpful. Cannabis used primarily to dissociate from everything is a different pattern worth monitoring honestly.
A Note for Veterans
Veterans are disproportionately represented in the PTSD population, and many Pennsylvania veterans have found that standard VA medications — SSRIs, prazosin — provided only partial relief or side effects they could not tolerate. The VA’s official position remains cautious on cannabis because the evidence base is not yet large enough for a formal recommendation. That is the VA’s position. It is not the same as saying cannabis does not help.
You can have a VA provider and a PA MMJ card simultaneously. Using medical cannabis does not disqualify you from VA care or VA mental health services. You do not need your VA provider’s permission to get a PA MMJ card — though telling your VA mental health provider you are using cannabis is important so they can monitor interactions with any prescribed medications.
Pennsylvania has over 100 dispensaries statewide. Access is not a barrier. The process is straightforward and can be completed entirely from home.
Drug Interactions: PTSD Medications and Cannabis
Most PTSD patients are on one or more medications. Here is what you need to know.
SSRIs and SNRIs (sertraline, paroxetine, venlafaxine) — These are the FDA-approved first-line pharmacotherapies for PTSD. CBD inhibits certain CYP450 enzymes involved in SSRI metabolism, which can theoretically increase SSRI blood levels. The interaction is generally mild at dispensary doses but worth mentioning to your prescribing physician. Do not stop your SSRI to use cannabis — they can work together.
Prazosin (used for PTSD nightmares) — Alpha-1 blocker with its own evidence for nightmare reduction. Cannabis and prazosin have overlapping goals for nighttime use. Both can cause blood pressure changes. The combination is not contraindicated but starting cannabis at low doses while monitoring for dizziness or lightheadedness is sensible. Tell your prescriber.
Benzodiazepines (Xanax, Klonopin, Valium) — Both benzodiazepines and THC cause central nervous system depression and sedation. Combined, the sedative and cognitive effects can be significantly amplified. This is the most important interaction caution for PTSD patients. If you are on a benzodiazepine, start cannabis at a very low dose, use it carefully at night rather than during the day, and tell your prescribing physician. Do not add high-THC cannabis to a benzodiazepine regimen without medical supervision.
Antipsychotics (quetiapine, risperidone) — Sometimes used off-label for PTSD. These have their own sedative and cognitive effects. Additive sedation is a concern. Discuss with your prescriber.
How to Get Your PA MMJ Card for PTSD
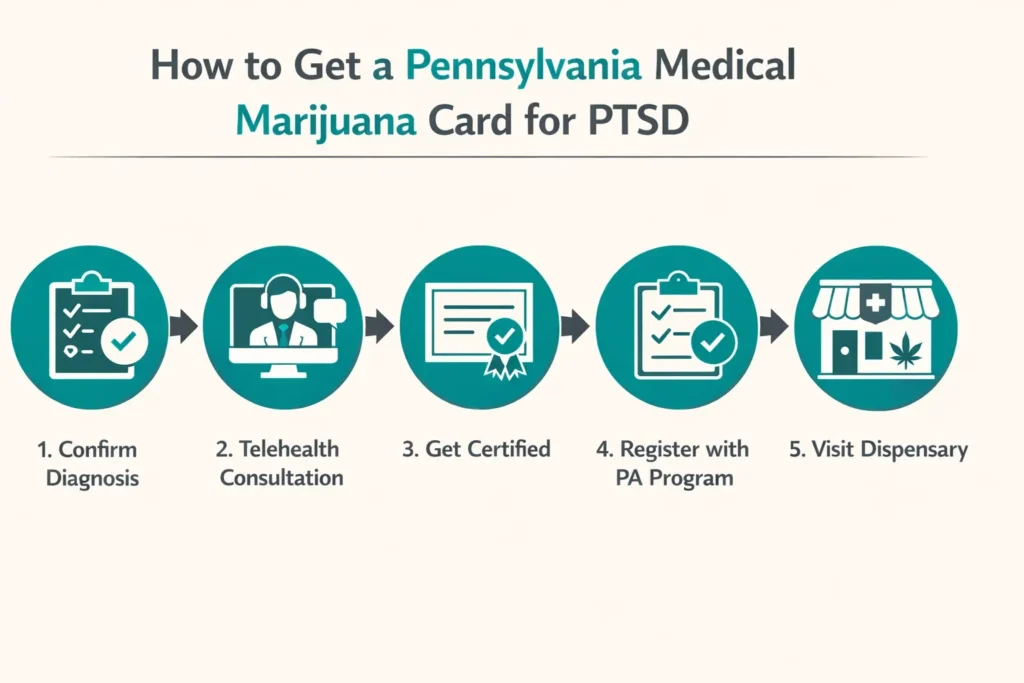
Step 1 — Get your diagnosis documented.
You need documentation of a PTSD diagnosis from a licensed mental health professional or physician — a psychiatrist, therapist’s records, or primary care physician notes that reference the diagnosis are all useful. You do not need extensive records; the certifying physician simply needs confirmation of the diagnosis.
Step 2 — Tell your mental health provider.
If you are in therapy or working with a psychiatrist, tell them before starting cannabis. Not because you need their permission — but because your therapist should know what you are using, and because interactions with SSRIs, prazosin, or benzodiazepines are real considerations that require awareness.
Step 3 — Book a telehealth certification appointment.
Find a PA DOH-registered medical marijuana certifying physician and complete the telehealth appointment from home. It takes 10–15 minutes. Bring your diagnosis documentation and medication list.
Step 4 — Register with the PA MMJ Program.
After certification, register at patientportal.mmapinc.com with your PA driver’s licence or state-issued ID and the $50 annual fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 5 — Visit a Pennsylvania dispensary.
Tell the dispensary pharmacist you have PTSD and describe your priority symptoms — nightmares and sleep, hyperarousal, daytime anxiety, or a combination. Ask for balanced THC:CBD products for nighttime and higher-CBD products for daytime if needed. Start at the lowest available dose.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
Frequently Asked Questions
Q: I am already in therapy for PTSD. Should I still get a PA MMJ card?
Q: I am a veteran. Will getting a PA MMJ card affect my VA benefits?
Q: I take Xanax for panic attacks related to my PTSD. Is it safe to use cannabis too?
Q: Cannabis makes me feel anxious sometimes. Does that mean it won’t work for my PTSD?
Q: Will cannabis replace my SSRIs?
Q: Is PTSD from something other than combat or military service still qualifying?
Pennsylvania PTSD Support Resources
Pennsylvania Coalition Against Rape (PCAR) — pcar.org Statewide advocacy and support organisation for survivors of sexual violence in Pennsylvania, including trauma-informed referrals to mental health providers.
Veterans Crisis Line — Call 988, then press 1. Text 838255. Available 24/7. Immediate support for veterans and service members in crisis. Confidential.
Pennsylvania Department of Military and Veterans Affairs – PTSD Resources — dmva.pa.gov Pennsylvania-specific veteran mental health programmes and referral resources.
National Center for PTSD — ptsd.va.gov The most comprehensive evidence-based resource on PTSD treatment, research, and self-help tools available anywhere. Invaluable reading regardless of whether you are a veteran.
PTSD Alliance — ptsdalliance.org Patient-facing education and support resources for all trauma survivors, not just veterans.
Crisis Text Line — Text HOME to 741741 for free, confidential support 24/7.
NOTE: PTSD does not go away because you want it to. The nights keep coming, the hypervigilance keeps humming, the memories keep arriving without invitation. The work of healing is real and it is slow and it does not always follow a straight line.
A PA MMJ card is not a cure. But for better sleep, quieter nights, a nervous system that is slightly less locked in fight-or-flight — it is a real option, backed by real evidence, available to you right now through a straightforward process from your own home. You have been carrying this long enough to deserve every tool that might help.