Chronic pain does not look the same from the outside. To everyone else, you appear fine. You get up, you show up, you manage — because you have learned to manage, because there is no other choice. But inside, there is the constant companion that never fully leaves. The burning in your feet. The ache that wakes you at 3am. The nerve pain that shoots down your leg for no reason at all. The days when the medication that worked last month has stopped working as well, and you are back at square one, trying something new, hoping this time it will be different.
Chronic pain — especially when it comes from nerve damage — is one of the most difficult conditions to treat in all of medicine. Standard medications help some patients meaningfully. For others, they provide only partial relief, come with side effects that become their own burden, or stop working over time. If that is your experience, Pennsylvania’s medical marijuana program exists, in part, for you.
Severe chronic and intractable pain is one of the most commonly used qualifying pathways for a PA MMJ card — and this page covers what actually qualifies, what the research honestly shows, and how to use a PA MMJ card in a way that is both safe and realistic.
Does Chronic or Intractable Pain Qualify for a PA MMJ Card?
Yes. The full qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016) is: “Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain in which conventional therapeutic intervention and opiate therapy is contraindicated or ineffective.”
This is one of the broadest qualifying conditions on Pennsylvania’s list — and intentionally so. It covers two overlapping situations:
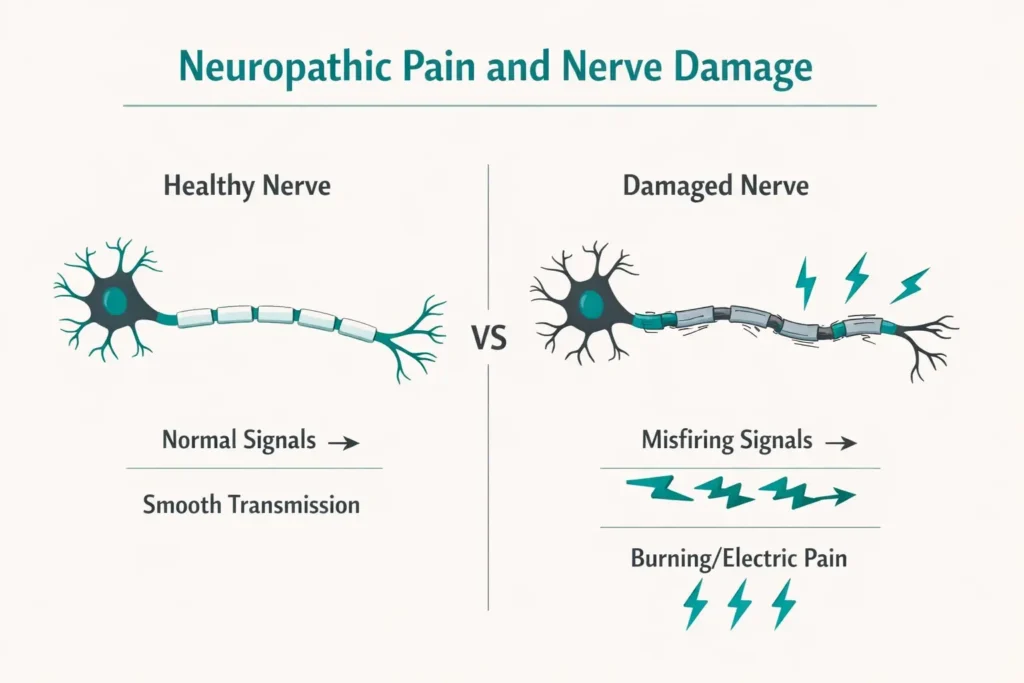
The first is pain of neuropathic origin — pain that comes from damaged, malfunctioning, or diseased nerves. This includes diabetic neuropathy, postherpetic neuralgia (shingles-related nerve pain), complex regional pain syndrome (CRPS), chemotherapy-induced peripheral neuropathy, HIV-associated neuropathy, radicular pain from disc disease, and many others.
The second is any severe chronic or intractable pain where conventional treatment and opioid therapy are either contraindicated (not medically appropriate for you) or have not worked adequately. This means patients with severe chronic pain from conditions like fibromyalgia, osteoarthritis, failed back surgery syndrome, chronic migraines, and more can qualify under this pathway — even if their condition is not separately named elsewhere on Pennsylvania’s qualifying list.
In practical terms: if you have severe, persistent pain that has not responded adequately to standard treatments, and a licensed physician confirms that — you qualify.
Sources:
- Pennsylvania Department of Health – Medical Marijuana Qualifying Conditions
- 28 Pa. Code Appendix A – Serious Medical Conditions
What Conditions This Pathway Covers
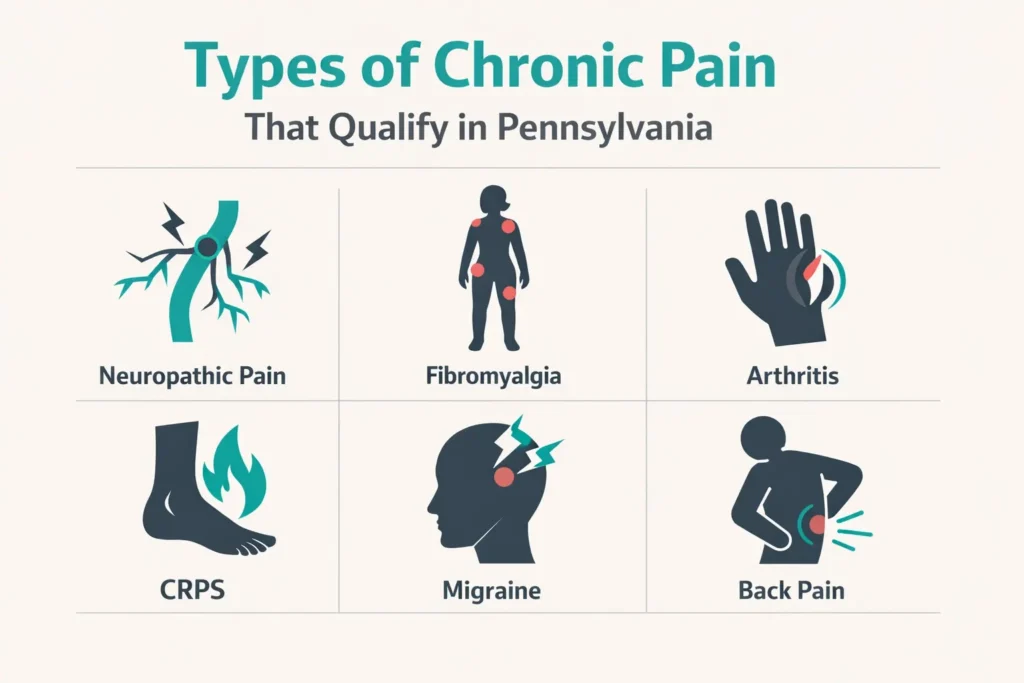
Because this qualifying condition is broad, it is worth listing the types of pain it commonly covers — because many patients do not realise their condition qualifies.
Neuropathic pain conditions that commonly qualify include diabetic peripheral neuropathy, postherpetic neuralgia, CRPS (complex regional pain syndrome), chemotherapy-induced peripheral neuropathy, HIV-associated neuropathic pain, spinal cord injury pain, central sensitisation pain, and chronic radiculopathy (nerve root pain from the spine).
Other severe chronic pain conditions that qualify through the “conventional treatment contraindicated or ineffective” pathway include fibromyalgia, severe osteoarthritis where surgery is not appropriate or has not resolved pain, failed back surgery syndrome, chronic migraine, degenerative disc disease with persistent pain, endometriosis-related chronic pelvic pain, and interstitial cystitis.
If your pain is severe, persistent, and has not been adequately controlled by conventional approaches — whatever the underlying cause — talk to a certifying physician about whether this pathway applies to you.
What the Research Honestly Shows
Chronic pain is by far the most common qualifying condition cited by medical cannabis patients across the United States. That means more research exists for pain than almost any other condition. It also means the research picture is complex — and honesty here matters more than enthusiasm.
The Overall Finding: Small But Real Benefit for Neuropathic Pain
The most rigorous and up-to-date review of the evidence is the Agency for Healthcare Research and Quality (AHRQ) living systematic review on cannabis for chronic pain, updated through 2025 with 29 randomised controlled trials and 15 observational studies. The vast majority of trial participants had neuropathic pain.
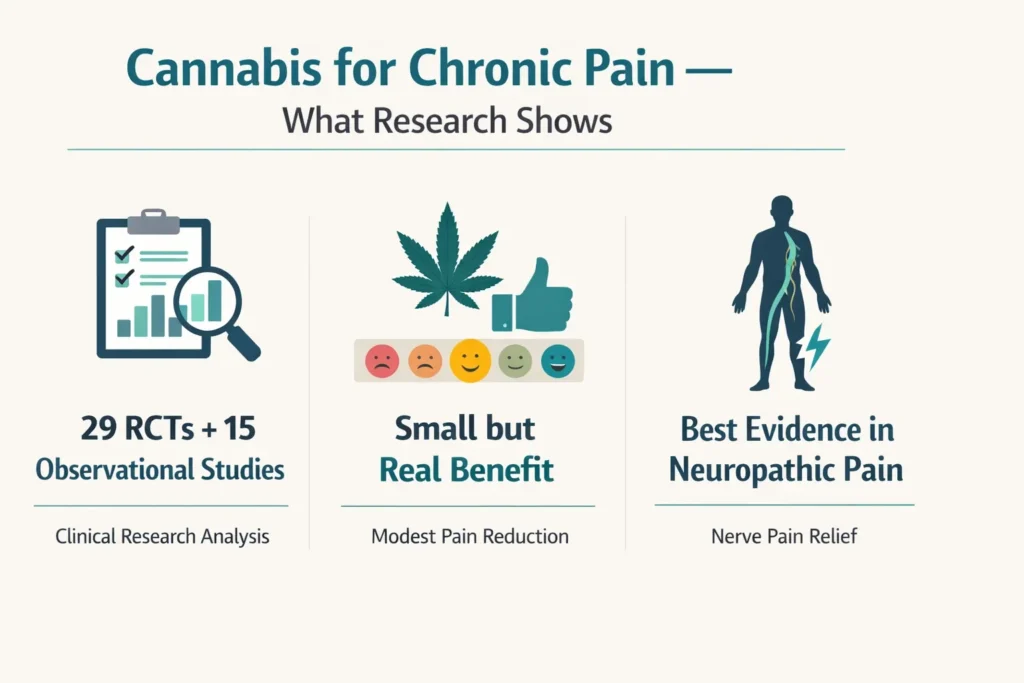
The key findings from this review — and from the most recent Annals of Internal Medicine update published in 2026 — are consistent: oromucosal extracted cannabis products with a comparable THC:CBD ratio probably produce small improvements in pain severity versus placebo, with a pooled difference of approximately 0.54 points on a 0–10 scale. THC-only products may show slightly more benefit (0.78 points reduction) but with more adverse effects. CBD-only (low THC) products may not improve pain outcomes versus placebo at all.
A 2024 systematic review of 14 randomised trials for peripheral neuropathy specifically found that 13 of 14 studies (93%) observed a statistically significant decrease in neuropathic pain score following cannabinoid treatment, with a mean difference of −0.67 points on a 0–10 scale compared with placebo. Secondary outcomes including sleep, sensory symptoms, and quality of life also improved.
A 2025 comprehensive systematic review covering studies from 2003 to 2024 found significant pain reductions in 15 studies across MS, spinal cord injuries, diabetic neuropathy, postherpetic neuralgia, HIV-associated neuropathy, CRPS, and peripheral neuropathy of the lower extremities.
What does “small but real” mean in practical terms? A reduction of 0.5–1.0 points on a 10-point pain scale may not sound dramatic. But for a person who has lived at a 7 out of 10 for years, moving to 6 or even 6.5 — combined with better sleep, less anxiety about pain, and improved daily functioning — can make a meaningful difference in quality of life. The research measures average effects across heterogeneous populations. Individual responses vary considerably, and some patients report much more substantial relief.
Sources:
- AHRQ – Living Systematic Review on Cannabis for Chronic Pain: 2025 Update
- PubMed – Cannabis-Based Products for Chronic Pain: Updated Systematic Review, Annals of Internal Medicine (2026)
- PubMed – Use of Cannabinoids in Treatment of Peripheral Neuropathy: Systematic Review (2024)
- PMC – Are Cannabis-Based Medicines a Useful Treatment for Neuropathic Pain? Systematic Review (2025)
What Cannabis Does Well for Chronic Pain — Beyond Pain Scores
The research focus on numerical pain score reductions misses much of what chronic pain patients actually value. Beyond the pain itself, the most consistent and meaningful benefits observed across studies include:
Sleep
Chronic pain and sleep disruption are inseparable companions. Cannabis, particularly THC-containing products at low to moderate doses taken before bed, consistently improves sleep onset and sleep quality in chronic pain patients. For patients who lie awake because of pain, this alone has real quality-of-life impact.
Anxiety about pain
The fear and anticipatory anxiety that build around chronic pain — will it be bad today? Can I make it through work? What if I cannot manage? — are dimensions of pain that cannabis addresses through CBD’s anxiolytic effects and THC’s mood-modulating effects. Reducing pain-related anxiety often improves functional capacity even when the raw pain score does not change much.
Daily functioning
Many clinical trials report improvements in overall functioning and quality of life even in studies where pain score reductions are modest. Being able to do more, rest better, and engage with life more fully is a real outcome that matters to real people.
Reduced reliance on other medications
Many chronic pain patients report being able to reduce doses of other pain medications when using cannabis. The formal research on “opioid sparing” is mixed — randomised trials have not consistently confirmed this effect, while observational studies frequently show it. The disconnect likely reflects the difference between controlled trial conditions (where opioid doses are held steady) and real-world use (where patients naturally adjust). What can be said honestly: some patients find cannabis allows them to use less of other medications; others do not. This should not be assumed, but it is a real outcome for a meaningful subset of patients.
What the Research Does Not Show
Cannabis is not a cure for chronic pain. It does not repair damaged nerves, reverse diabetic neuropathy, fix failed back surgery, or address the underlying cause of any pain condition. The evidence for pure CBD products (no meaningful THC) relieving pain is weak — CBD alone at typical dispensary doses does not have strong evidence for analgesic effect. Very high-THC products are not necessary for pain relief and bring more side effects. And the evidence is clearest for neuropathic pain — for some other chronic pain types, the benefit is more uncertain.
Managing realistic expectations is not pessimism. It is what allows you to use cannabis effectively as part of a broader pain management strategy, rather than as a replacement for everything else.
THC, CBD, and the Right Ratio for Pain
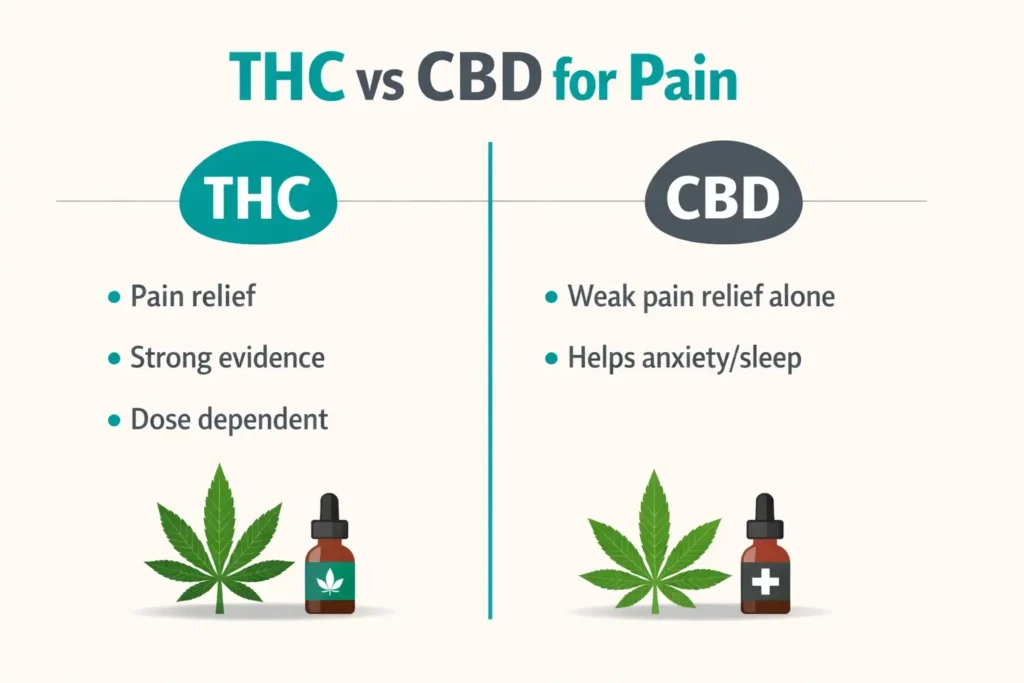
For chronic and neuropathic pain specifically, the evidence points clearly toward products with meaningful THC content alongside CBD — not CBD-only products. The AHRQ review found that low THC:CBD ratio products (predominantly CBD) may not improve pain outcomes at all. The signal is in the THC, modulated and made more tolerable by the presence of CBD.
Comparable THC:CBD ratio products (roughly 1:1) have the strongest evidence base for pain — they appear to offer pain relief while keeping the psychoactive and side-effect burden manageable compared to high-THC products alone.
Mild THC-dominant products with CBD present are appropriate for patients who need more pain relief and have established they tolerate THC well.
CBD-dominant or CBD-only products for pain specifically are not well-supported by the controlled trial evidence. They may help with anxiety, sleep, and inflammation-related discomfort, but as direct analgesics the evidence is weak.
The practical starting point for most PA chronic pain patients: a balanced 1:1 or 2:1 (THC:CBD) oral tincture or capsule, starting at a very low dose and increasing slowly over weeks.
PA Dispensary Product Guidance for Chronic Pain

Oral Tinctures and Oils
The most appropriate first format for most chronic pain patients. Sublingual tinctures (absorbed under the tongue) work faster — 15–45 minutes — making them useful for breakthrough pain or acute flares. Swallowed oil or capsules have slower but longer-lasting effects (2–5 hours), better suited to sustained daily pain management.
Take oral cannabis products with a small amount of fat — a spoonful of peanut butter, a small piece of cheese — to significantly improve absorption and consistency.
Capsules
Capsules provide the most consistent, predictable dosing for daily use. They are slower to work (60–90 minutes) but deliver sustained relief without the variability of sublingual absorption. For patients managing around-the-clock pain, a consistent daily capsule dose provides a reliable baseline.
Topicals
Topical cannabis products — creams, balms, and patches — are appropriate for localised pain: joint pain, muscle pain, peripheral neuropathy in specific areas (feet, hands). They deliver cannabinoids locally without significant systemic absorption, meaning no psychoactive effect. They will not address central or widespread pain, but for localised neuropathic pain in the hands or feet, a quality topical can be a useful addition with minimal side effects.
Vaporised Cannabis
Vaporised flower has faster onset than oral products (minutes rather than hours), making it suitable for acute breakthrough pain that needs quick relief. The tradeoff is shorter duration (1–2 hours versus 3–5 for oral) and more variable dosing. It is a reasonable option for experienced patients managing acute pain episodes but not the best starting point for someone new to cannabis.
What to Avoid
Very high-THC products (above 20% THC with minimal CBD) carry the highest side-effect burden — dizziness, sedation, cognitive impairment — without proportionally greater pain relief. CBD-only tinctures are unlikely to provide meaningful pain relief based on current evidence. Edibles from dispensaries (capsules and oils specifically, not food-based edibles) are fine; food-based edibles from unlicensed sources should be avoided entirely.
Starting Dose
Start with 2.5–5 mg THC equivalent in a balanced product. Wait at least 90 minutes before assessing oral products, since onset is slow and new users often re-dose too early and overshoot their comfort level. Increase by 2.5 mg increments every few days, not every few hours. The goal is the lowest dose that provides meaningful relief with manageable side effects.
Drug Interactions: Common Pain Medications and Cannabis
Most chronic pain patients are already on one or more medications. The most important interactions to know:
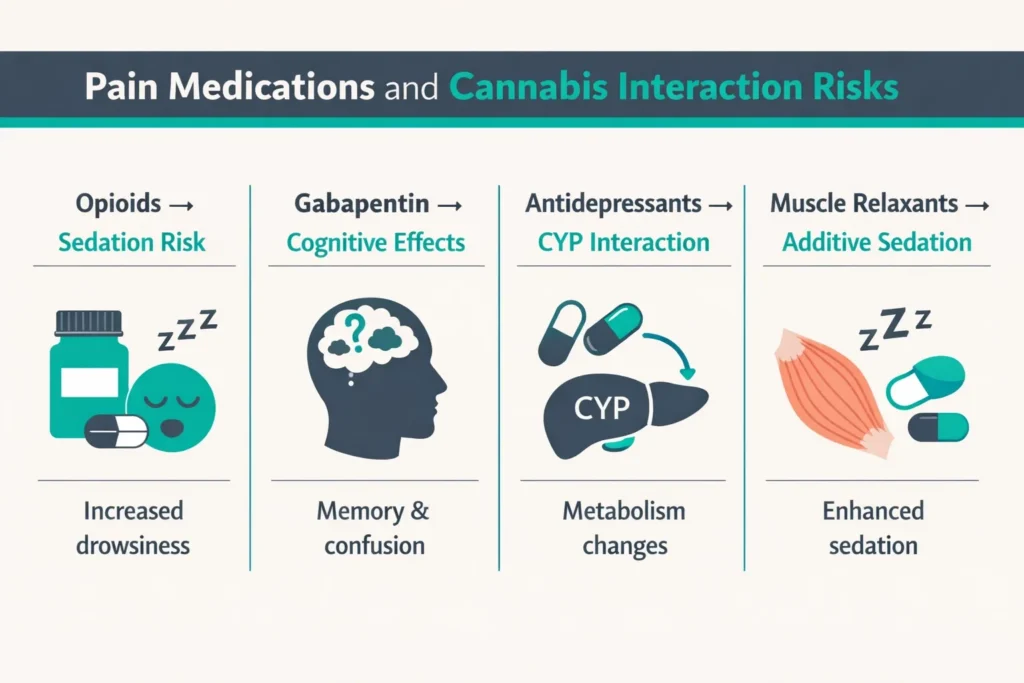
Opioids (oxycodone, hydrocodone, morphine, buprenorphine) — Both opioids and THC cause central nervous system depression, sedation, and cognitive effects. Combined, these can be amplified. This does not mean the combination is forbidden — many patients use both — but starting cannabis at a low dose while on opioids is important to avoid excessive sedation. Do not abruptly reduce opioids based on feeling better from cannabis without physician guidance, as opioid dependence requires managed tapering.
Gabapentin and pregabalin (Neurontin, Lyrica) — Commonly used for neuropathic pain. Both cause sedation and cognitive effects that can compound with THC. Start cannabis low and monitor for increased drowsiness or cognitive fog.
NSAIDs (ibuprofen, naproxen, celecoxib) — Low interaction risk from a pharmacokinetic standpoint. These are not significantly metabolised through CYP450 pathways that cannabis substantially affects. No major interaction concern.
Antidepressants used for pain (duloxetine, amitriptyline) — CBD can inhibit CYP2D6, which metabolises some tricyclic antidepressants, potentially increasing their levels. Duloxetine interactions are less established. Tell your prescriber you are adding cannabis.
Muscle relaxants (baclofen, cyclobenzaprine, methocarbamol) — Additive sedation with THC is the key concern. Start low and avoid daytime high-THC doses if muscle relaxants are causing sedation already.
The overarching principle: tell your pain management physician or primary care doctor before starting cannabis. The interactions are manageable but require awareness, particularly around opioids and sedating medications.
How to Get Your PA MMJ Card for Chronic Pain
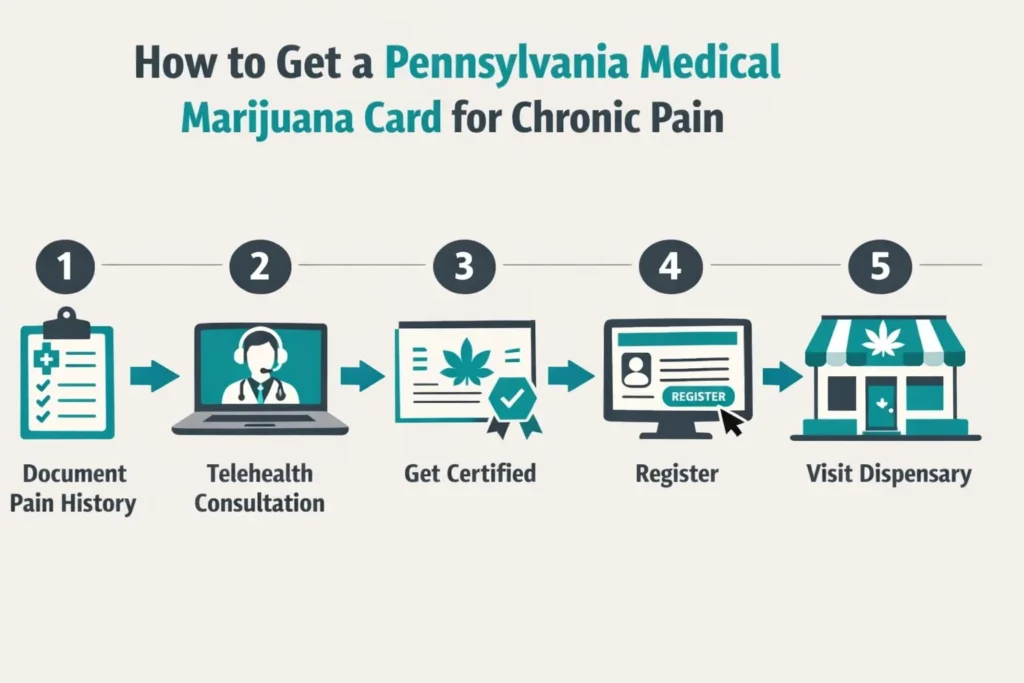
Step 1 — Document your pain history.
Pull together any records that document your pain diagnosis, the treatments you have tried, and why they have not been adequate — physician notes, specialist reports, medication history. The certifying physician needs to understand your pain is severe, chronic or intractable, and has not responded sufficiently to conventional approaches.
Step 2 — Tell your pain management doctor or primary care physician.
They need to know you are using cannabis — particularly because of the interactions with opioids, gabapentin, and sedating medications. You do not need their permission, but keeping them informed is both a safety requirement and clinically sensible.
Step 3 — Book a telehealth certification appointment.
A PA DOH-registered certifying physician evaluates you via telehealth from home. Appointments take 10–15 minutes. Bring your pain history and medication list. The physician submits your certification electronically to the Pennsylvania Department of Health.
Step 4 — Register with the PA MMJ Program.
Go to the PA Medical Marijuana Program Patient Registry at patientportal.mmapinc.com. Provide your PA driver’s licence or state-issued ID and the $50 annual fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 5 — Visit a Pennsylvania dispensary.
Tell the pharmacist you have chronic or neuropathic pain and describe where your pain is and what you are already taking. Ask for balanced THC:CBD products — a 1:1 ratio tincture or capsule as a starting point. Start at the lowest available dose, take it consistently for at least two weeks before evaluating, and increase slowly.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
- Chronic Hepatitis C
Frequently Asked Questions
Q: My pain is from fibromyalgia, which is not listed separately. Can I still qualify?
Q: I have chronic back pain but no formal nerve damage diagnosis. Do I qualify?
Q: I am already on opioids. Can I still get a PA MMJ card?
Q: Will cannabis definitely reduce my pain?
Q: CBD alone is cheaper at health food stores. Why should I get a PA MMJ card for CBD products?
Q: Will cannabis interact badly with my gabapentin?
Pennsylvania Chronic Pain Support Resources
American Chronic Pain Association (ACPA) — theacpa.org The leading patient organisation for chronic pain in the United States, with condition-specific resources, peer support group listings by state, and evidence-based pain management education. Pennsylvania patients can find local support through the ACPA’s group directory.
Penn Medicine Pain Management — pennmedicine.org Academic pain management services in Philadelphia and southeastern Pennsylvania, including interventional pain, neuropathic pain, and integrative pain management approaches.
UPMC Pain Medicine — upmc.com/pain Western Pennsylvania’s major academic pain management programme, covering neuropathic pain, chronic pain rehabilitation, and interdisciplinary approaches.
National Institute of Neurological Disorders and Stroke – Chronic Pain — ninds.nih.gov Authoritative patient-facing information on neuropathic and chronic pain conditions, treatment options, and current research.
NOTE: Chronic pain does not care about your plans or your schedule or your relationships. It just keeps showing up. And the treatments that are supposed to help do not always help enough, or come with a cost of their own that you have to weigh every single day.
Pennsylvania’s medical marijuana program will not fix what medicine has not been able to fix. But for better nights, less daily suffering, and a tool that addresses pain through pathways that conventional medications do not reach — a PA MMJ card is a real and legally supported option, backed by real evidence, available to you through a process that starts at home.