
If you live with sickle cell disease, you know what it means to have your pain questioned. You have sat in emergency rooms explaining yourself to providers who look at you with suspicion instead of compassion. You have heard the word “drug-seeking” used about people who are in genuine, severe, medically documented pain. You have managed crises at home alone because the alternative — another ER visit where you wait in agony while your chart is scrutinised — sometimes feels worse than suffering through it yourself.
The pain of sickle cell disease is not exaggerated. It is not a character failure. It is one of the most severe and complex pain syndromes in medicine. And the patients who experience it — predominantly Black Americans — have faced decades of systemic under-treatment, bias, and stigma that make managing this disease harder than it already is.
Pennsylvania included sickle cell anemia as a qualifying condition under its Medical Marijuana Act from the very beginning. This page covers everything you need to know: what qualifies, what the research shows, what cannabis can and cannot do for sickle cell, and how to get your PA MMJ card.
Does Sickle Cell Anemia Qualify for a PA MMJ Card?
Yes. Sickle cell anemia is one of the original qualifying conditions listed in the Pennsylvania Medical Marijuana Act (Act 16 of 2016), recognised by the Pennsylvania Department of Health from the program’s launch.
All forms of sickle cell disease qualify — not just the HbSS (classic sickle cell anemia) genotype. This includes sickle-hemoglobin C disease (HbSC), sickle beta-thalassemia (HbSβ0 and HbSβ+), and other sickle cell variants. If you have any confirmed sickle cell disease diagnosis, you qualify.
There is no severity requirement, no minimum number of pain crises per year, and no requirement to have failed specific medications. A confirmed diagnosis is the threshold.
Sources:
- Pennsylvania Department of Health – Medical Marijuana Qualifying Conditions
- 28 Pa. Code Appendix A – Serious Medical Conditions
What Sickle Cell Disease Actually Does — The Reality Behind the Diagnosis
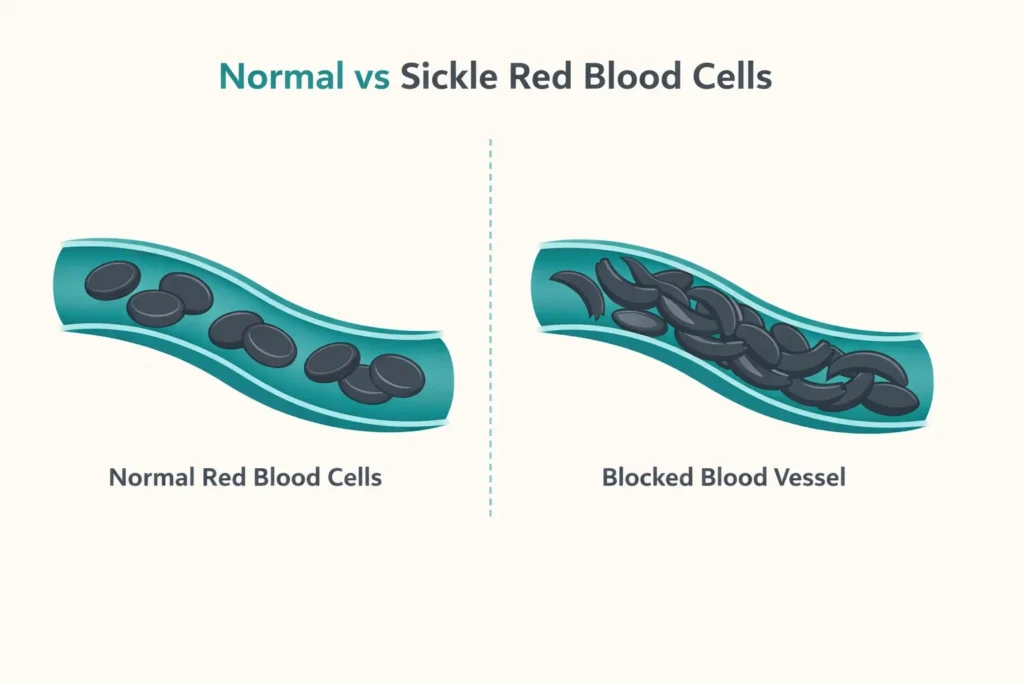
Sickle cell disease is a group of inherited blood disorders caused by a mutation that produces abnormal hemoglobin — the protein in red blood cells that carries oxygen. Normal red blood cells are flexible discs that move easily through blood vessels. Sickle cells are rigid and crescent-shaped. They stick to vessel walls, clump together, and block blood flow.
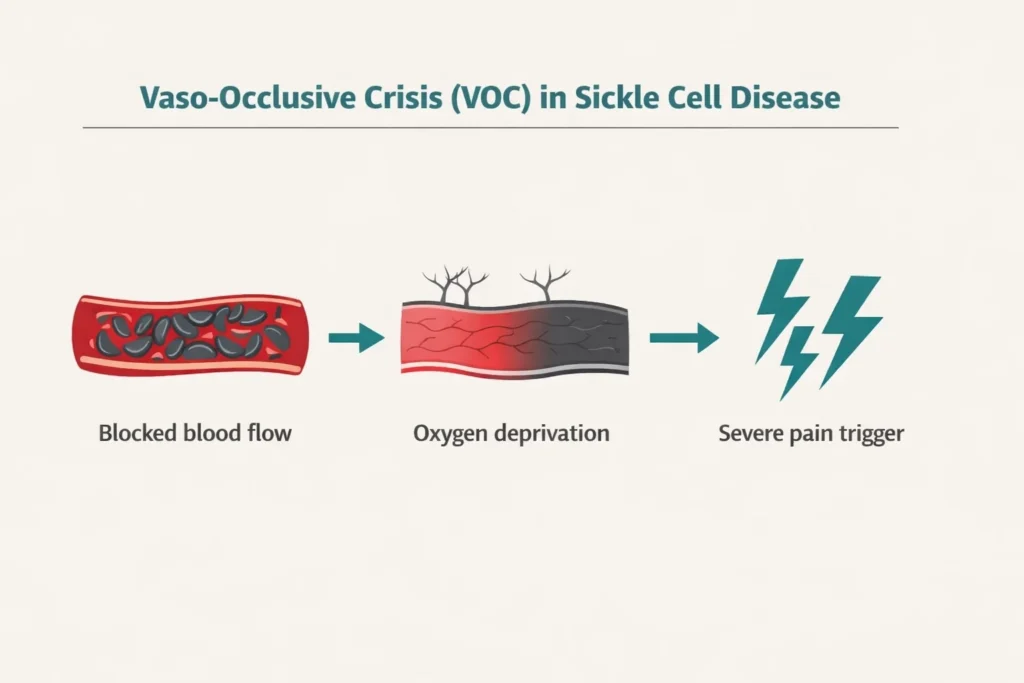
When blood flow stops — even briefly — the tissue downstream is deprived of oxygen. That is a vaso-occlusive crisis (VOC). It produces severe, sudden, often excruciating pain that can hit any part of the body: the bones, chest, abdomen, joints. Sixty percent of SCD patients will experience a vaso-occlusive crisis in any given year. These crises are the leading reason for hospitalisation and emergency visits. They are unpredictable. They can be triggered by dehydration, cold, stress, illness, or nothing identifiable at all.
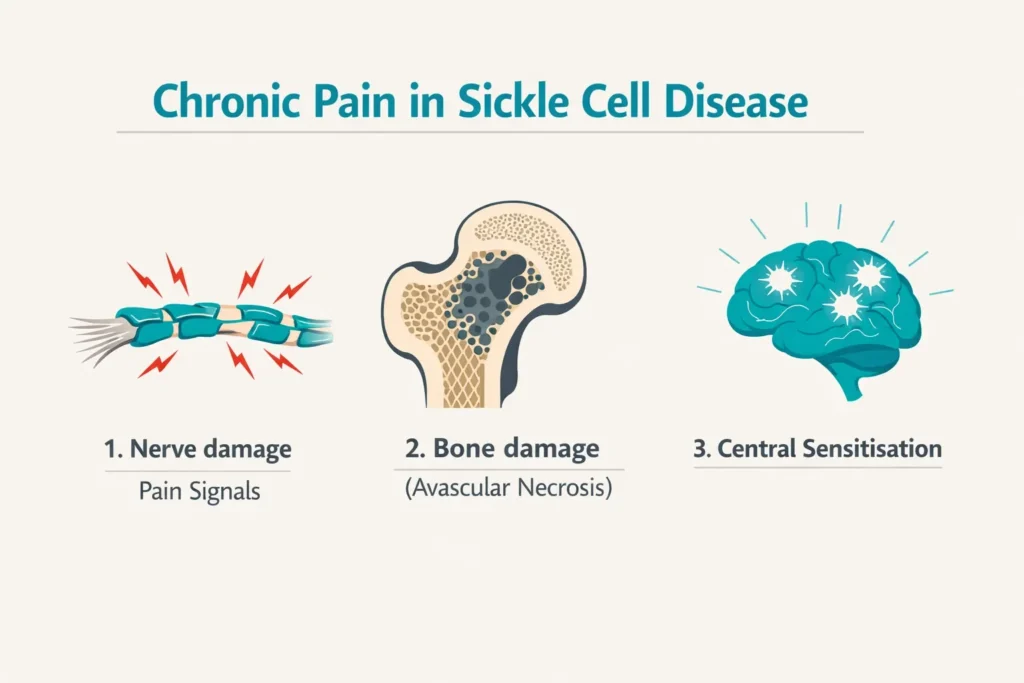
Beyond the crises, sickle cell disease causes relentless chronic pain that builds over years. Up to 40% of SCD patients live with chronic pain between crises. This chronic pain has both nociceptive and neuropathic components — nerve damage, bone damage from avascular necrosis, and central sensitisation that makes the nervous system increasingly reactive to pain signals over time.
The full picture of SCD also includes anaemia and crushing fatigue, heightened risk of stroke and infection, lung complications like acute chest syndrome, kidney damage, and for many patients, a significantly shortened life expectancy. The median life expectancy in the United States for people with SCD is 43 years.
And layered over all of this is the healthcare experience that far too many SCD patients describe: pain that is real and documented and severe, met with scepticism, under-treatment, and labels that follow them from one ER visit to the next.
The Healthcare Bias Problem — And Why a PA MMJ Card Matters Beyond Medicine
This is not a tangential point. It is central to why access to medical cannabis matters so much for people with sickle cell disease in Pennsylvania specifically.
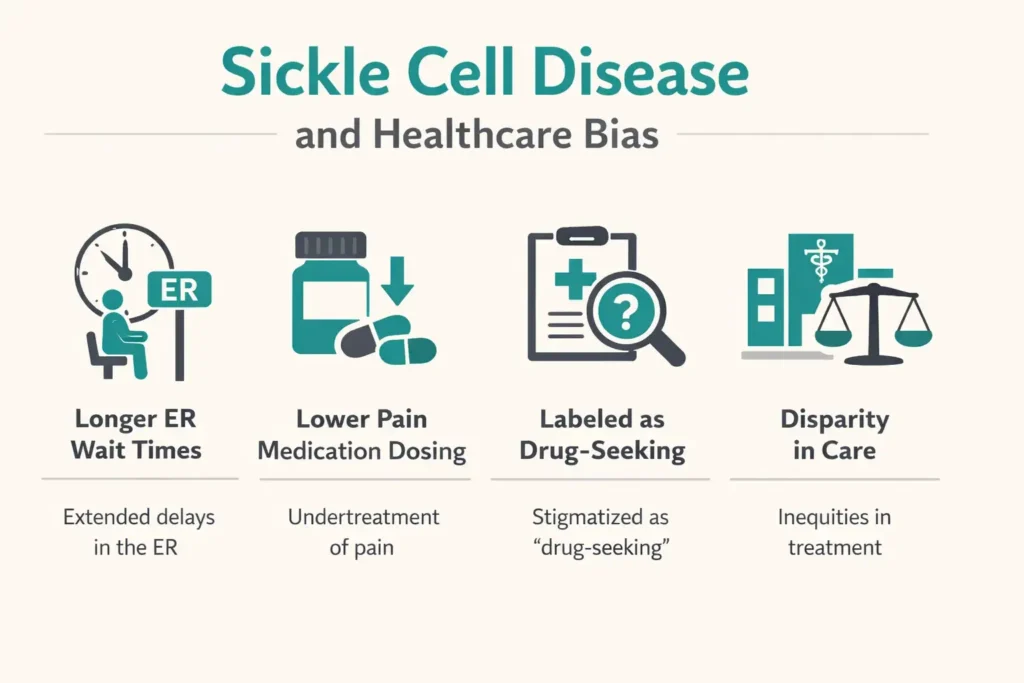
Research published in peer-reviewed medical journals — including the New England Journal of Medicine and multiple systematic reviews — documents that Black patients with SCD are consistently undertreated for pain, face longer wait times in emergency departments, receive lower doses of analgesic medications, and are more likely to be labelled as drug-seeking than white patients presenting with comparable pain. This happens despite clear evidence that SCD pain is biologically severe and despite CDC data showing prescription opioid overdose deaths are highest among non-Hispanic white patients.
The current opioid prescribing environment — with increased scrutiny and restrictions on controlled substances — has paradoxically made this worse for SCD patients, who have legitimate chronic pain needs that may require high-dose opioids during crises and who are disproportionately Black.
A PA MMJ card does not fix this systemic problem. But it does something important: it gives SCD patients in Pennsylvania a state-protected, legal, non-opioid tool for pain and symptom management that they can access without an emergency room, without a provider’s discretionary decision about whether their pain is “real enough,” and without the label that follows too many SCD patients through the healthcare system.
That is not a small thing.
Sources:
- NEJM – Treating Chronic Pain in Sickle Cell Disease: The Need for a Biopsychosocial Model
- ScienceDirect – Implicit Bias in Pain Management: The Intersection of Stigma, Race, and Chronic Disease in Sickle Cell Disease (2026)
What the Research Shows: Cannabis and Sickle Cell Disease
The Landmark Clinical Trial
The most important study in cannabis and sickle cell disease was published in JAMA Network Open in 2020. This was the first double-blind, placebo-controlled, randomised trial to use gold-standard methods to assess cannabis for pain in SCD patients — a landmark achievement given how difficult these trials have historically been to conduct due to federal restrictions.
Twenty-three adults with SCD-related chronic pain completed the trial at UC San Francisco, inhaling vaporised cannabis or vaporised placebo during two five-day inpatient sessions. The cannabis used contained equal parts THC and CBD (obtained from the National Institute on Drug Abuse).
The results showed that vaporised cannabis was generally safe and well-tolerated. Pain improvement did not reach statistical significance as the primary endpoint, but the trial was designed primarily as a safety and feasibility study — it was not powered to definitively establish efficacy. Importantly, there was measurable improvement in mood and no significant adverse events, and the researchers concluded that vaporised cannabis appears to be a safe option and warranted further investigation.
The lead researcher, Professor Kalpna Gupta of UC Irvine, stated that the results suggest SCD patients may be able to mitigate their pain with cannabis and that cannabis might help address the opioid crisis. She called the trial the doorway to testing different forms of medical cannabis for SCD chronic pain.
What Patient Surveys and Observational Studies Show
Between 25% and 50% of adult SCD patients report using cannabis to manage their pain. Survey data across multiple studies paints a consistent picture of what patients themselves report:
A questionnaire study of SCD patients in the UK found that cannabis users reported improvement in mood (35%), reduced use of painkillers (42%), improvement in anxiety and depression (52%), and improvement in sleep (61%). Importantly, no patients reported worsening of their SCD symptoms, and 58% expressed interest in participating in clinical trials studying cannabis for SCD.
A 2025 scoping review covering all available evidence on cannabis for chronic pain in SCD — published in the journal Pain Management Nursing — found mixed but generally positive evidence, with no studies showing exacerbation of SCD symptoms. The review noted that cannabinoids may help manage SCD pain in select patients, while emphasising the need for larger, more standardised trials.
Real-world clinical observations have also suggested that daily cannabis users may have fewer admissions and emergency visits — potentially because cannabis increases pain tolerance and allows patients to manage some crises at home. This observational finding is not definitive, but it is consistent with what many SCD patients report.
Sources:
- Pain Management Nursing – Cannabis Use for Chronic Pain in Sickle Cell Disease: A Scoping Review (2025)
- PMC – Considerations for Cannabis Use to Treat Pain in Sickle Cell Disease
Preclinical Evidence: The Biology Is Compelling
In animal models of sickle cell disease, cannabinoid receptor agonists consistently reduce both chronic and acute hyperalgesia. CB1 and CB2 receptors are present throughout the pain pathways most relevant to SCD — the spinal cord, the brain’s pain processing centres, and the peripheral nervous system. A 2023 study published in Blood found that CBD specifically attenuates hyperalgesia in a mouse model of SCD.
The endocannabinoid system’s role in modulating the inflammatory and vascular components of SCD pathology is an active area of preclinical investigation. While this basic science has not yet been translated into definitive human clinical outcomes, it provides the biological rationale for why cannabis-based approaches are being studied specifically in this population.
What Cannabis Cannot Do
Cannabis does not reverse the sickling of red blood cells. It does not treat the underlying haemoglobin mutation. It does not prevent vaso-occlusive crises. It does not replace disease-modifying treatments like hydroxyurea or, for eligible patients, bone marrow transplant or the newer gene therapy approaches.
What cannabis may do — based on the available evidence — is reduce the pain severity, improve sleep, reduce anxiety, support mood, and potentially reduce reliance on opioids during periods of chronic pain management between crises. These are meaningful, real-world benefits for people living with a lifelong, painful, complex disease.
PA Dispensary Product Guidance for Sickle Cell Disease
For Chronic Background Pain
The JAMA trial used a balanced 1:1 THC:CBD vaporised product and found it safe. For PA dispensary use, a balanced 1:1 THC:CBD tincture or oil taken orally is the most appropriate starting format for ongoing chronic pain management. Oral products provide longer-lasting relief (3–5 hours) versus inhalation (1–2 hours), making them better suited to daily baseline pain management.
Start low — 2.5–5 mg THC equivalent — and increase slowly over weeks. Take with a small amount of fat to improve absorption. Capsules are a good option for consistent daily dosing.
For Acute Pain Flares at Home
For breakthrough pain episodes managed at home, a faster-onset format is more appropriate. Sublingual tinctures (absorbed under the tongue) work in 15–45 minutes. For patients comfortable with inhalation, vaporised cannabis has the fastest onset of any format — minutes rather than hours — which is relevant when pain comes on suddenly.
The evidence from the JAMA trial specifically used vaporised cannabis, and the researchers noted that vaporisation may be safer than other forms because lower amounts reach the body’s circulation. Pennsylvania dispensaries carry vaporisable flower and oil cartridges for pen-style vaporisers. Vaporisation is permitted under Pennsylvania law; smoking is not.
For Anxiety, Depression, and Sleep
The patient survey data consistently shows improvements in anxiety, depression, and sleep alongside pain relief in SCD patients using cannabis. CBD-dominant products (20:1 or higher CBD:THC ratio) are appropriate for daytime anxiety management without significant psychoactive effect. Balanced products taken at night are appropriate for sleep.
Important: Product Standardisation
The research on cannabis in SCD consistently emphasises that product quality, consistency, and known cannabinoid content matter. Pennsylvania’s licensed dispensaries are required to test and label their products accurately — this matters for SCD patients in a way it does not for casual users. Ask the dispensary pharmacist for products with a verified, consistent cannabinoid profile. Do not rely on unlicensed or unverified products.
Drug Interactions: SCD Medications and Cannabis
Most SCD patients are on one or more medications. The key interactions to know:
Hydroxyurea — The most widely used disease-modifying treatment in SCD. Hydroxyurea is not significantly metabolised through CYP450 pathways that cannabinoids substantially affect. The direct pharmacokinetic interaction risk between cannabis and hydroxyurea is low. Continue hydroxyurea exactly as prescribed — cannabis does not replace it.
Opioids (morphine, hydromorphone, oxycodone) — Both THC and opioids cause central nervous system depression, sedation, and respiratory depression. Combined, these effects can be amplified. For patients using opioids for crisis management or chronic pain, adding cannabis requires starting at a low THC dose and monitoring carefully. Do not abruptly reduce prescribed opioids based on cannabis use — taper under physician supervision if opioid reduction is a goal.
L-glutamine — Used to reduce pain crises in SCD. No significant known cannabis interaction. Continue as prescribed.
Voxelotor (Oxbryta) and crizanlizumab (Adakveo) — Newer disease-modifying agents. These are metabolised through CYP3A4 pathways. CBD is a CYP3A4 inhibitor and could theoretically increase levels of these medications. The interaction is not well-characterised in clinical data for SCD specifically, but it warrants disclosure to your haematologist when adding cannabis to your regimen.
NSAIDs (ibuprofen, naproxen, ketorolac) — Low pharmacokinetic interaction risk. These are not primarily metabolised through CYP450 pathways cannabis affects significantly.
The overall message is the same as for every condition: tell your haematologist and pain management physician before starting cannabis. Your haematologist needs to know because of the newer disease-modifying agents, and your pain management physician needs to know because of the opioid interactions.
How to Get Your PA MMJ Card for Sickle Cell Disease
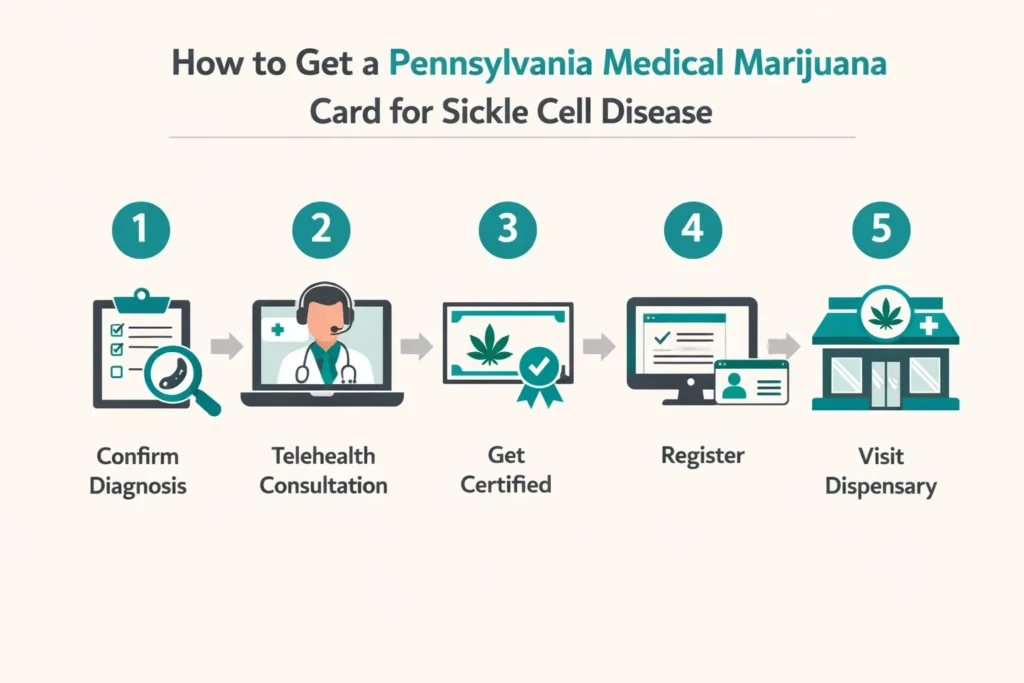
Step 1 — Document your diagnosis.
Your haematologist’s records confirming your SCD diagnosis and genotype are all you need. Any physician documentation of your diagnosis is sufficient. You do not need recent hospitalization records, though bringing your current medication list is helpful.
Step 2 — Tell your haematologist.
Your haematologist should know you are using cannabis — particularly because of the potential interactions with newer disease-modifying agents like voxelotor and crizanlizumab. You do not need their permission. But keeping them informed is important for your medical care.
Step 3 — Book a telehealth certification appointment.
Find a PA DOH-registered medical marijuana certifying physician and complete the evaluation from home via telehealth. It takes 10–15 minutes. Bring your SCD diagnosis records and medication list.
Step 4 — Register with the PA MMJ Program.
After your certification, go to the PA Medical Marijuana Program Patient Registry at patientportal.mmapinc.com. You need your PA driver’s licence or state-issued ID and the $50 annual registration fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 5 — Visit a Pennsylvania dispensary.
Tell the pharmacist you have sickle cell disease. Describe whether you are primarily managing chronic background pain, acute flares at home, or both. Ask for a balanced THC:CBD product with verified cannabinoid content. Start at the lowest available dose.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
Frequently Asked Questions
Q: I have HbSC disease, not HbSS. Do I still qualify?
Q: Will cannabis stop my vaso-occlusive crises?
Q: I am already on hydroxyurea. Can I use cannabis too?
Q: I am concerned about being seen as drug-seeking. Will getting a PA MMJ card affect how my pain is treated in the ER?
Q: Can I use cannabis instead of opioids for my pain?
Q: My child has sickle cell disease. Can they get a PA MMJ card?
Pennsylvania Sickle Cell Support Resources
Sickle Cell Disease Association of America (SCDAA) — sicklecelldisease.org The national patient advocacy organisation for sickle cell disease. Provides patient education, physician referrals, research updates, and advocacy resources. Their Find a Doctor tool can connect Pennsylvania patients with SCD specialists.
Children’s Hospital of Philadelphia (CHOP) – Sickle Cell Center — One of the leading paediatric sickle cell programmes in the United States, serving Pennsylvania families.
UPMC Children’s Hospital of Pittsburgh – Sickle Cell Disease Program — Specialist sickle cell care for western Pennsylvania patients, including transition programmes for adolescents moving to adult care.
Penn Medicine – Division of Hematology/Oncology — Adult sickle cell specialist care in Philadelphia and southeastern Pennsylvania.
National Heart, Lung, and Blood Institute – Sickle Cell Disease Information — nhlbi.nih.gov/sickle-cell-disease Authoritative, patient-facing information on SCD management, current treatments, and ongoing clinical trials.
Sickle Cell Disease News — sicklecellanemianews.com Patient-focused news and research updates on sickle cell disease, including coverage of cannabis research.
NOTE: Living with sickle cell disease means living with pain that is real, severe, and documented — and has still too often been met with doubt. Pennsylvania’s medical marijuana program offers a state-protected, legally accessible, non-opioid tool for pain and symptom management that does not require anyone’s approval of how much your pain deserves to be treated.
The evidence for cannabis in SCD is promising and growing. The biology is compelling. The patient experience consistently points toward meaningful help with pain, sleep, anxiety, and mood. And accessing it no longer requires a trip to the emergency room, an argument with a sceptical provider, or a label that has no place in the care of someone managing one of the most painful conditions in medicine.