If someone you love has Alzheimer’s disease, dementia, or another condition that affects the brain over time, you know how hard the difficult days can be. The restlessness that starts at sundown. The sleepless nights. The sudden distress that comes from nowhere and is nearly impossible to calm. The gradual loss of appetite and weight.
These symptoms — not just the memory loss, but all of the behavioral and physical challenges that come with it — are exactly what medical marijuana has been studied for in people with neurodegenerative diseases. And in Pennsylvania, neurodegenerative diseases are an official qualifying condition for the state’s medical marijuana program.
This page is written for families and caregivers as much as it is for patients themselves. It explains what qualifies, what the research says in plain language, how to navigate the process when your loved one can no longer manage their own care, and what realistic expectations look like.
Does Alzheimer’s Disease (and Other Neurodegenerative Conditions) Qualify in Pennsylvania?
Yes. Pennsylvania’s Medical Marijuana Act specifically lists “neurodegenerative diseases (i.e., Alzheimer’s Disease)” as a qualifying condition — and the parenthetical is just an example, not the full list. Many brain conditions that involve progressive nerve cell damage qualify under this umbrella.
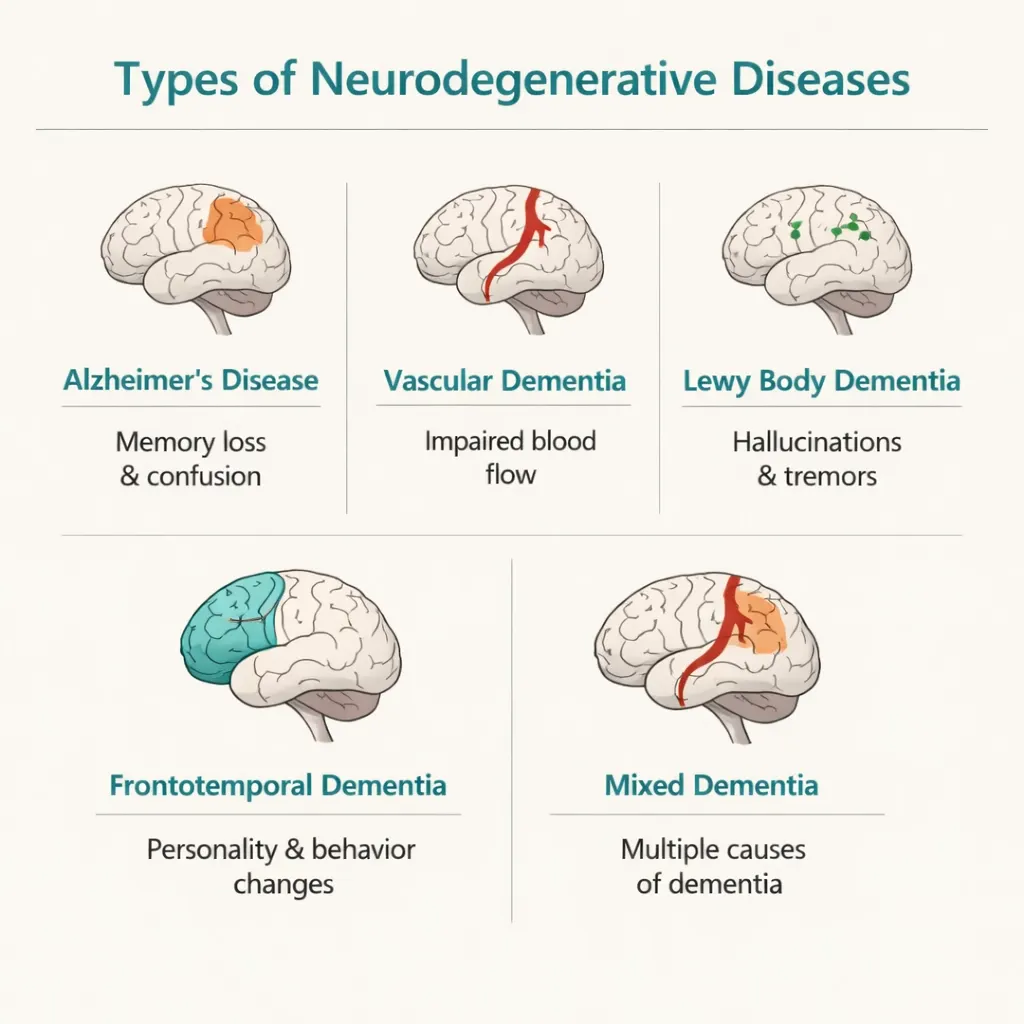
Here are the diagnoses that fall under this qualifying condition:
- Alzheimer’s disease — the most common form of dementia
- Vascular dementia — caused by reduced blood flow to the brain
- Lewy body dementia — related to abnormal protein deposits in brain cells
- Frontotemporal dementia (FTD) — affects personality, behavior, and language
- Mixed dementia — a combination of two or more types
- Multiple system atrophy, progressive supranuclear palsy, corticobasal degeneration — rarer conditions causing movement and cognitive changes
- Prion diseases (such as Creutzfeldt-Jakob disease)
- Huntington’s disease and other hereditary neurodegenerative conditions
If your loved one’s neurologist has diagnosed them with any condition described as progressive, neurodegenerative, or involving long-term deterioration of brain cells, it is worth asking a PA MMJ certifying physician whether the diagnosis qualifies.
Note: Parkinson’s disease and ALS each have their own separate qualifying condition entry in Pennsylvania’s program. Patients with those diagnoses can certify under either their specific condition or under the neurodegenerative diseases category — ask your certifying physician which makes most sense.
- Source: Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Source: 28 Pa. Code Appendix A – Serious Medical Conditions
The Most Important Thing to Understand Upfront
Medical marijuana will not stop or reverse Alzheimer’s disease or any other neurodegenerative condition. No treatment currently available can do that — including the newer Alzheimer’s medications like lecanemab and donanemab, which only modestly slow progression in very early disease.
What medical marijuana can do is help with the behavioral and physical symptoms that make life so much harder for both the person with dementia and the people who care for them. Things like:
- Agitation, restlessness, and aggression
- Disturbed sleep and nighttime waking
- Loss of appetite and unintended weight loss
- Anxiety and emotional distress
These are the symptoms that often drive emergency room visits, early entry into memory care facilities, and caregiver burnout. They are also the symptoms where the research on cannabis is most promising — and where families report the most meaningful real-world relief.
What Does the Research Show? (In Plain Language)
Agitation — The Symptom That Changes Everything
Agitation is one of the hardest parts of living with or caring for someone with advanced dementia. It shows up as pacing that never stops, repeated questions or cries of distress, sudden aggression toward caregivers, or an inability to settle. Nearly half of all people with moderate-to-severe Alzheimer’s experience significant agitation, and it often gets worse in the late afternoon and evening — a pattern families call “sundowning.”
The problem with current medications for agitation in dementia is serious. Antipsychotic drugs like quetiapine (Seroquel), risperidone (Risperdal), and olanzapine (Zyprexa) are commonly used off-label for agitation in dementia, but they carry an FDA Black Box Warning: these medications increase the risk of stroke-like events and death in elderly patients with dementia. They also cause sedation, falls, and metabolic changes. Families and doctors are often caught between inadequate behavioral interventions and medications with genuinely dangerous side effects.
This is exactly why the research on THC in dementia agitation matters so much.
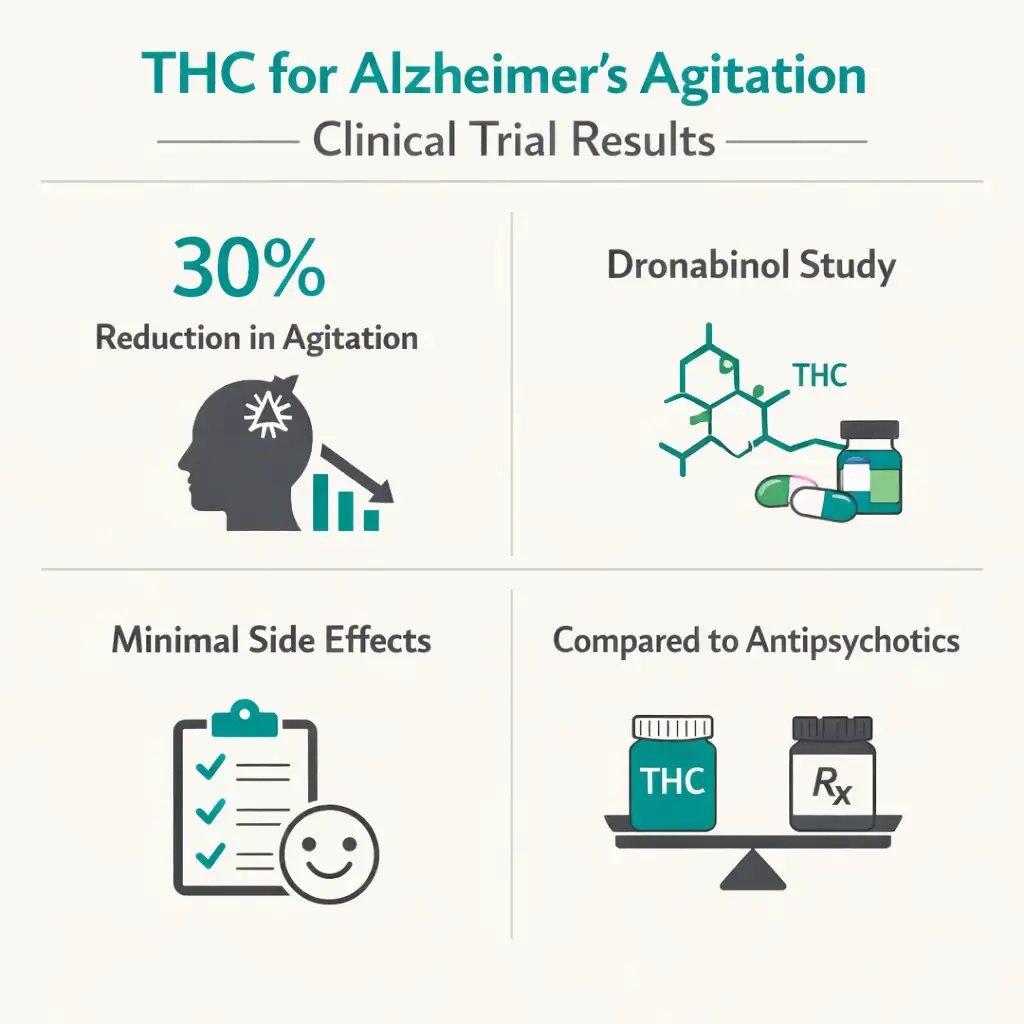
The Johns Hopkins and Tufts University clinical trial (2024): After eight years of work, researchers at two of the country’s top academic medical centers completed a randomized, double-blind, placebo-controlled trial — the gold standard of medical research — testing dronabinol (a synthetic form of THC) for severe Alzheimer’s agitation. Seventy-five patients with confirmed Alzheimer’s and significant agitation participated. Those taking dronabinol showed about a 30% reduction in agitation compared to the placebo group. Side effects were minimal. The investigators concluded that dronabinol performed as well as or better than the only other FDA-approved medication for dementia agitation currently on the market — without the dangerous cardiovascular risks of antipsychotics.
“It is the agitation, not the memory loss, that often drives individuals with dementia to the emergency department and long-term care facilities,” said Dr. Brent Forester, co-principal investigator and psychiatry chairman at Tufts Medical Center. “Dronabinol has the potential to both reduce health care costs and make an important, positive impact on caregivers’ mental and physical health.”
The University of Chicago real-world study (2023): A study published in the Journal of Clinical Psychiatry looked at what happened when clinicians at a major U.S. academic medical center actually recommended dispensary-obtained THC to 50 patients with dementia-related behavioral symptoms — real products, from real dispensaries, as caregivers would actually obtain them in states like Pennsylvania. The results were striking:
- 79% of patients who took THC showed caregiver-reported improvement in agitation, aggression, irritability, lability, anxiety, and sleep
- Among the 20 patients who were on antipsychotics when they started THC, more than half were able to decrease or discontinue their antipsychotic after adding THC
- THC was found to be 100% effective in patients with late-onset Alzheimer’s dementia in this dataset
This is particularly meaningful for families who have a loved one on antipsychotics and are worried about the risks — the possibility of potentially reducing that medication while maintaining behavioral control is a genuine quality-of-life improvement for both patient and family.
Sleep — The Gift for the Whole Family
When someone with dementia can’t sleep, nobody in the household sleeps. Disturbed sleep in dementia can mean waking at 2am confused and frightened, pacing through the night, or cycles of daytime sleeping that completely reverse the normal rhythm of the day.
Multiple studies have found improvements in sleep for dementia patients using cannabis. A 2023 study of 30 patients (ages 65–90) using THC oil sublingually found meaningful improvements in nighttime sleep patterns reported by family caregivers, with patients settling more consistently and requiring fewer late-night interventions.
The Penn Memory Center at the University of Pennsylvania reviewed the available evidence in 2025, noting that a study using CBD-rich oil showed over 94% of dementia patients had at least a 30% reduction in agitation, and that caregiver distress decreased alongside patient improvement — because the two are inseparably linked.
Better sleep for the person with dementia often means better sleep for the whole household. For a family caregiver, that is not a small thing.
Appetite and Weight Loss
Refusing food is common in advanced dementia — sometimes because agitation or distress makes sitting at the table impossible, sometimes because the pleasure of eating has simply faded. Unintended weight loss in dementia is associated with faster decline and more medical complications.
THC has well-documented appetite-stimulating properties. It works by activating receptors in the brain’s appetite centers, and this effect has been studied in dementia patients specifically. Low-dose THC taken before meals can improve willingness to eat and increase caloric intake, helping to maintain weight and nutritional status without the side effects of pharmaceutical appetite stimulants.
Could Cannabis Actually Help the Brain? Emerging Research
A 2025 Phase 2 clinical trial — the longest controlled study of cannabinoids in Alzheimer’s disease to date at 26 weeks — tested a low-dose balanced THC/CBD extract in patients with Alzheimer’s-associated dementia. At the end of the trial, patients in the cannabis group had significantly higher scores on the Mini-Mental State Exam (MMSE) than those in the placebo group — a meaningful finding, even though cognitive outcomes were listed as secondary endpoints.
This is early evidence. It does not mean cannabis reverses Alzheimer’s disease or slows its progression definitively. But it adds to a growing body of preclinical research suggesting that cannabinoids may have neuroprotective properties — potentially reducing brain inflammation and protecting neurons from some of the damage processes involved in Alzheimer’s. Researchers at the Penn Memory Center note that multiple ongoing trials are investigating cannabinoid therapy as a gentler alternative to antipsychotics for end-of-life dementia care.
- Source: PubMed – A Randomized Clinical Trial of Low-Dose Cannabis Extract in Alzheimer’s Disease (2025)
Being Honest About What We Don’t Know
Research on cannabis in neurodegenerative diseases is still growing. Most studies have been small. Not everyone responds the same way — in the University of Chicago study, 10% of patients had adverse reactions (dizziness, worsening agitation, or increased paranoia), and a small number had to stop THC. Cannabis can cause sedation, dizziness, and an increased fall risk in older adults, which matters enormously for someone who already has balance or mobility challenges. High doses of THC are not appropriate for elderly or frail patients.
The goal for this population is almost always low-dose, slow-start, monitored use — with an informed caregiver involved at every step.
This Is a Journey for the Whole Family — The Caregiver Pathway
Here is something many families don’t realize until they’re deep in the process: Pennsylvania has a specific caregiver registration pathway for patients who cannot manage their own medical marijuana care. This is one of the most important practical features of the PA MMJ program for anyone dealing with dementia.
When someone has significant cognitive impairment — whether from Alzheimer’s, vascular dementia, Lewy body disease, or another condition — they may not be able to navigate the physician certification process, register on the state website, or travel to a dispensary. The caregiver pathway solves this.
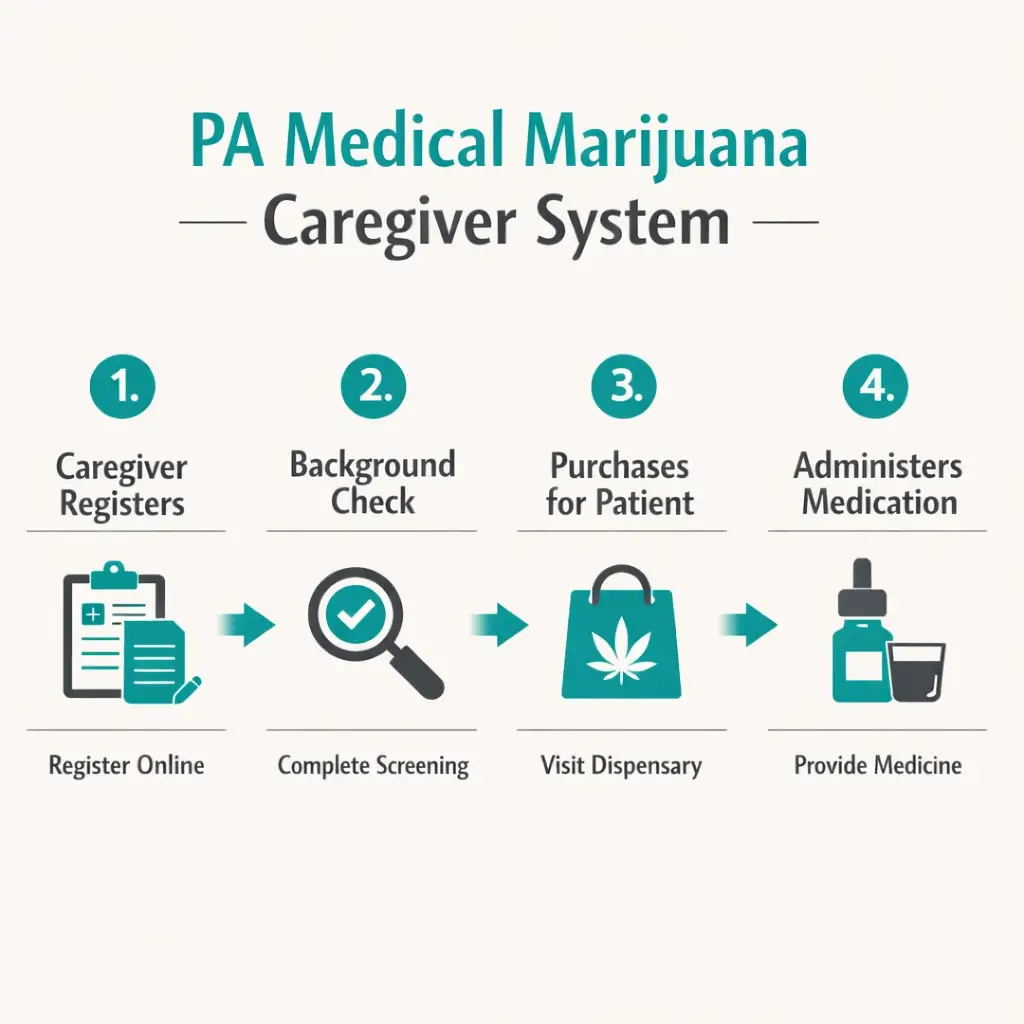
How the caregiver pathway works:
A designated caregiver in Pennsylvania is a family member, spouse, partner, or other trusted adult who is authorized by the PA Department of Health to purchase and administer medical marijuana on behalf of a patient. The caregiver registers with the state, passes a background check, and gets their own caregiver ID card. They then visit the dispensary and bring the medication home.
For a patient with dementia who cannot visit a dispensary independently, the caregiver does everything — the patient only needs to have their qualifying diagnosis confirmed by a certifying physician (often via telehealth, with the caregiver present).
Caregiver requirements in Pennsylvania:
- Must be 21 years old or older
- Must be a Pennsylvania resident with a valid PA driver’s license or state-issued ID
- Must have no criminal convictions related to drug possession or sale within the past five years
- Must register with the PA DOH and pass a criminal background check
- $50 annual registration fee (fee waivers available for patients on Medicaid, SNAP, WIC, CHIP, PACE/PACENET)
- One patient can designate up to two caregivers
- Each caregiver can serve up to five patients
- Caregivers may purchase up to a 90-day supply at a time
The caregiver pathway is particularly important because many dementia patients are in the moderate-to-severe stages of disease, where they no longer have full decision-making capacity. Pennsylvania’s program accommodates this through the “Caregiver Registering for a New Patient” option on the state portal — the caregiver registers on behalf of the patient, who does not receive their own ID card and does not visit the dispensary.
- Source: PA DOH – Medical Marijuana Patients and Caregivers
- Source: PA DOH – Register for the Medical Marijuana Program
A Note on Decision-Making and Capacity
For families navigating dementia care, the question of who makes medical decisions — and when — is already a familiar one. Medical marijuana is no different. If your loved one still has the capacity to participate in the decision to try cannabis, involve them. If they no longer have that capacity, the same person who holds their healthcare power of attorney or acts as their healthcare proxy in other medical decisions can make this decision on their behalf.
It is worth discussing this with both the certifying MMJ physician and the patient’s existing neurologist or primary care physician. Not because permission is required from multiple doctors — it isn’t — but because having everyone informed produces the best and safest care.
Choosing the Right Products: What Families Should Know
For elderly patients with neurodegenerative diseases, less is almost always more when it comes to cannabis. Here is simple, practical guidance:
Start lower than you think necessary. Products designed for a healthy 40-year-old are often far too strong for a 78-year-old with dementia. Ask specifically at the dispensary for the lowest-dose products available.
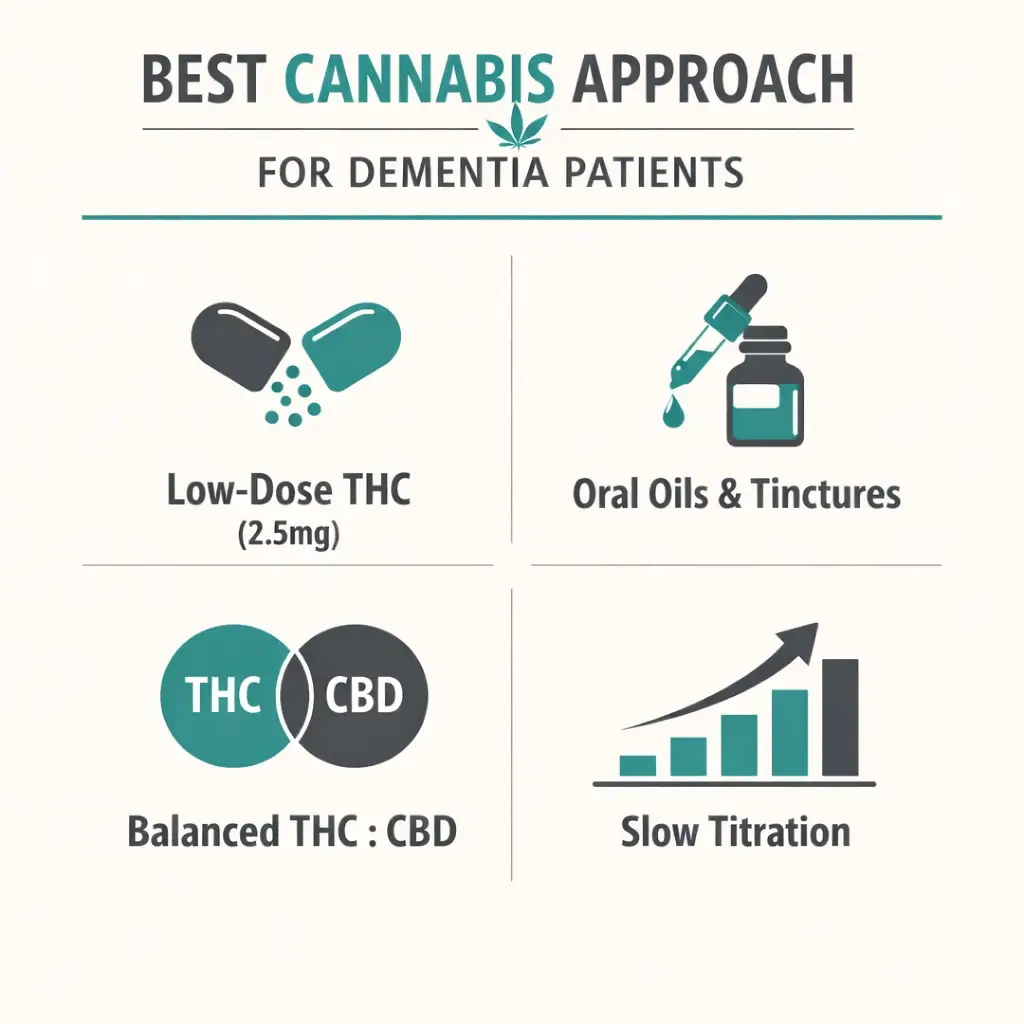
Oral formats work best for most dementia patients. Oils and tinctures placed under the tongue (sublingual) or added to food or drink are the easiest to administer consistently and allow for accurate, small doses. Capsules are also an option. Vaporized products are harder to dose consistently and present inhalation challenges for elderly patients.
THC-dominant products — particularly at low doses (starting around 2.5mg THC) — are the most studied for the symptoms that matter most in dementia: agitation, sleep, and appetite. The research is centered on THC, not CBD alone.
Balanced THC:CBD products may be gentler for patients who seem sensitive to THC’s effects. The anti-anxiety properties of CBD can complement THC for patients whose agitation has an anxious quality.
Timing matters. For agitation, a dose given an hour or two before the typical agitation window (often late afternoon/sundowning time) may be most effective. For sleep, a dose given 1–2 hours before the intended bedtime tends to work better than one given at bedtime itself.
Watch for side effects. The two most common concerns in this population are increased dizziness (which raises fall risk) and sedation that is too deep. Start with the smallest dose, observe for 24–48 hours before increasing, and keep a simple log of what you give, when, and what you observe. Bring that log to follow-up appointments.
Tell the dispensary pharmacist everything. Let them know your loved one’s age, weight, other medications, and what specific symptoms you are hoping to address. A good dispensary pharmacist is a resource — use them.
Step by Step: How to Get a PA MMJ Card for Your Loved One
Step 1 — Talk to the existing physician first (optional but helpful)
Let your loved one’s neurologist, geriatric psychiatrist, or primary care doctor know you are considering medical marijuana. They don’t have to agree or participate — but keeping them in the loop means they can flag any medication concerns and can monitor whether behavioral symptoms are improving or changing. If your loved one is on antipsychotics, the potential to eventually reduce or discontinue those with physician guidance is a conversation worth having.
Step 2 — Schedule the MMJ physician certification
Book a telehealth appointment with a PA DOH-registered medical marijuana physician. Caregivers can and should be present for this appointment to provide the patient’s history, medication list, and symptom description. The certifying physician will confirm the qualifying diagnosis and issue the certification. For patients with cognitive impairment, the caregiver’s presence is often essential to the appointment.
Step 3 — Decide on the registration pathway
If your loved one can still register themselves and visit a dispensary (even with help), they register as a standard adult patient and designate you as their caregiver simultaneously.
If your loved one can no longer manage their own care and will not be visiting the dispensary independently, you register as “Caregiver Registering for a New Patient” at the PA DOH portal. You become the registered caregiver; the patient does not get their own ID card.
Step 4 — Register and pay the fee
Register at the PA Medical Marijuana Program Patient Registry. The fee is $50 — for the patient’s card and/or the caregiver’s card. If your loved one is on Medicaid, SNAP, WIC, CHIP, PACE, or PACENET, the fee is waived.
Step 5 — Complete the background check (caregivers only)
Caregivers must pass a state criminal background check. This process typically takes 2–4 weeks. You’ll be notified by email.
Step 6 — Receive your card and visit a dispensary
Caregiver cards are mailed after approval. Bring the card to any PA dispensary. Tell the staff you are picking up for a patient with dementia and what you are trying to address (agitation, sleep, appetite). They can help you choose the right product.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Terminal illness
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
- Chronic Hepatitis C
Frequently Asked Questions
Q: Can my parent with Alzheimer’s get a PA MMJ card even if they can’t make decisions for themselves?
Q: What conditions besides Alzheimer’s qualify under “neurodegenerative diseases” in Pennsylvania?
Q: My dad is on Seroquel (quetiapine) for his agitation. Can cannabis help us reduce that?
Q: Will cannabis make my loved one more confused?
Q: Is there a risk of falls?
Q: What if my loved one is in memory care or a nursing facility?
Support Resources for Families in Pennsylvania
Alzheimer’s Association Delaware Valley Chapter serves southeastern Pennsylvania including Philadelphia. Their 24/7 helpline (800-272-3900) connects families with local resources, support groups, and clinical care navigation. Their website at alz.org has a large library of caregiver tools.
Alzheimer’s Association Greater Pennsylvania Chapter serves the western and central regions of the state. Same 24/7 helpline: 800-272-3900.
Penn Memory Center at the University of Pennsylvania (pennmemorycenter.org) is one of the leading dementia research and clinical care centers in the state. They publish patient-facing summaries of emerging research including their 2025 overview of cannabis and cognition cited on this page.
UPMC Alzheimer’s Disease Research Center in Pittsburgh provides both clinical care and research participation opportunities for families dealing with neurodegenerative diseases in western Pennsylvania.
Alzheimer’s Foundation of America (alzfdn.org) operates a free national care consultation service (866-232-8484) staffed by licensed social workers who can help families navigate care planning decisions including complementary therapies.
NOTE: Living with a neurodegenerative disease — or loving someone who does — is one of the most exhausting and heartbreaking experiences a family can face. There are no simple answers and no cure on the horizon. But for many families, medical marijuana has offered something real and meaningful: fewer nights of acute agitation, a little more sleep, a better appetite at mealtime, and a reduction in the dangerous antipsychotic medications that had become a last resort.
Pennsylvania’s program makes this accessible through the caregiver pathway — so even when a person with dementia cannot manage the process themselves, the family can. The card, the caregiver card, the dispensary visit — all of it can be done by the people who are already showing up every day for their loved one.
If this sounds like something worth exploring, the first step is simply a telehealth appointment with a PA-registered physician. Bring the diagnosis, bring the medication list, and bring your questions.