There are moments in life that call for straightforward answers rather than long explanations. If you or someone you love is facing a terminal illness, this page is written with that in mind — clearly, honestly, and with care for the difficulty of the situation you’re navigating.
Pennsylvania includes terminal illness as a qualifying condition for medical marijuana specifically because of what cannabis can offer at the end of life: relief from pain, help with nausea and appetite, better sleep, and something harder to measure but just as real — a sense of control over one’s own comfort during a time when so much else is beyond control.
Does Terminal Illness Qualify for Medical Marijuana in Pennsylvania?
Yes. Terminal illness with a medical prognosis of life expectancy of approximately one year or less if the illness runs its normal course is an explicitly named qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016).
A few important things this means:
Any terminal diagnosis qualifies — not just cancer. Advanced heart failure, end-stage COPD, end-stage renal disease, end-stage liver disease, advanced neurological conditions with a terminal prognosis, and any other serious illness where the expected trajectory is death within approximately a year all qualify under this provision.
“Approximately one year” is not a rigid cutoff. The language uses “approximately,” which gives certifying physicians flexibility to certify patients whose prognosis may be somewhat longer than 12 months but who clearly have a life-limiting terminal condition.
Patients with other qualifying diagnoses can certify under those conditions instead. Cancer has its own qualifying condition entry. So do ALS, HIV/AIDS, Parkinson’s disease, and neurodegenerative diseases. If your terminal illness is one of those named conditions, your certifying physician may choose to use that specific entry — or the terminal illness pathway — or both simultaneously. There is no functional difference in what you can access.
There is no requirement that you be on hospice. You do not need to have enrolled in a hospice program, stopped curative treatment, or met any other palliative care criteria to qualify. A terminal diagnosis with an approximate prognosis is sufficient.
- Source: Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Source: 28 Pa. Code Appendix A – Serious Medical Conditions
Why Cannabis at End of Life
When someone has a terminal illness, the goals of care shift. Instead of trying to cure a disease, the focus becomes comfort, quality of life, and the ability to be present — for your own experience, for the people who love you, for whatever time remains.
The symptom burden at end of life can be overwhelming. Pain that escalates as disease progresses. Nausea from medications or the illness itself. An appetite that disappears, making every meal a small battle. Nights that don’t bring rest. Anxiety about what’s coming. The deep sadness and sometimes fear that can settle in as life narrows.
Cannabis doesn’t fix any of that. But it can soften it — in ways that matter.
A palliative care physician, Dr. B.J. Miller — former director of the Zen Hospice Project and author of A Beginner’s Guide to the End — describes something that often gets missed in discussions of end-of-life cannabis: agency. At a time when illness takes so much out of a person’s hands, having a tool they chose, that they manage, that helps them feel more like themselves rather than more sedated — that matters. “Another important issue in palliative care is treating a person’s sense of agency,” he says, “and giving them as much freedom and control as possible.”
That dimension of comfort — not just the absence of symptoms, but the preservation of self — is part of what cannabis can offer.
What the Research Shows
Pain — The Most Common Reason Patients Seek Cannabis
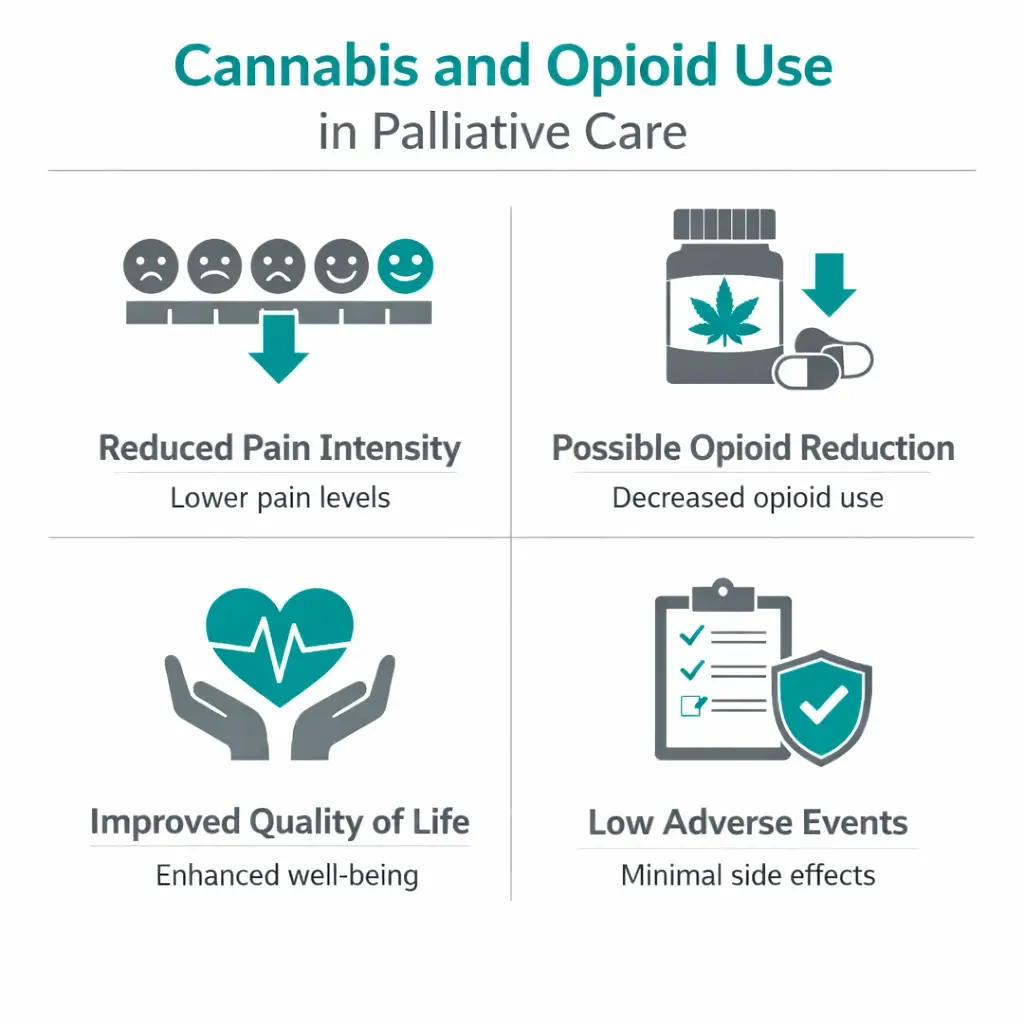
Pain affects roughly half of all people with cancer at some point, and a much higher proportion in advanced or terminal stages. For many patients, opioids are essential — and this page isn’t suggesting otherwise. What the research shows is that cannabis and opioids can work together in ways that benefit patients.
A 2024 study published in the American Journal of Hospice and Palliative Care — conducted at the Connecticut Hospice, affiliated with Yale School of Medicine — enrolled 66 hospice inpatients already on scheduled opioids for pain. They added standardized oral medical cannabis products (low-dose CBD/THC formulations) alongside the existing opioids. Over 996 treatment days, the combination produced a statistically significant reduction in pain intensity compared to baseline. A trend toward lower opioid doses was seen but did not reach statistical significance. Only 4.5% of patients had minor, reversible side effects. No serious adverse events occurred.
This “opioid-sparing” potential — the possibility of achieving equivalent or better pain control at lower opioid doses — is one of the most meaningful practical benefits for terminal patients. Opioids at high doses cause sedation, constipation, and cognitive fog. Anything that maintains pain control while potentially reducing those side effects preserves a patient’s ability to be present with their family.
A large observational study of over 2,970 cancer patients in Israel who used cannabis for palliative care found that among those who responded at 6 months, 36% had stopped using opioids entirely, while the number of patients reporting good quality of life rose from 18.7% before cannabis treatment to 69.5% at six months. These figures are observational — not controlled — but they reflect what real-world patients and families experience when cannabis is integrated into end-of-life care.
- Source: PubMed – Medical Marijuana for Pain Management in Hospice Care as Complementary Approach to Scheduled Opioids (Zanker et al., American Journal of Hospice and Palliative Care, 2024)
- Source: Annals of Palliative Medicine – Cannabis in Palliative Care: Current Challenges and Practical Recommendations (Cyr et al.)
Nausea — A Constant Companion at End of Life
Nausea in terminal illness comes from many directions at once — from the disease itself, from medications, from constipation, from the body’s shifting chemistry. For many terminal patients, nausea is the symptom that makes eating impossible and turns every day into an endurance test.
THC is among the most effective antiemetics in medicine. It works through CB1 receptors in the brainstem’s vomiting center — the same mechanism that made dronabinol (synthetic THC) an FDA-approved antiemetic in 1985. For patients whose nausea is not well-controlled by standard medications, or for those who want to reduce medication burden, cannabis offers a meaningful option.
Appetite and Weight — Eating Again
Appetite loss is nearly universal in advanced terminal illness. It’s one of the most distressing symptoms for families to witness — watching someone they love stop eating, knowing the body is slowly withdrawing. Cannabis’s appetite-stimulating effects, mediated by CB1 receptors in the hypothalamus, are well-documented. For a patient in the middle stages of a terminal illness who still has weeks or months to live, maintaining nutritional intake preserves strength, reduces fatigue, and supports the ability to spend meaningful time with people they love.
Sleep — The Night Becomes Hard
Disrupted sleep is nearly universal in terminal illness — from pain that wakes patients, from anxiety that arrives in the quiet hours, from the physical changes of the dying body. Most sleep medications in this setting come with sedation that carries into the day. For patients who still want to be awake and present in their waking hours, the balance is delicate.
Low-to-moderate THC doses taken before sleep, particularly through oral formulations that last longer than inhaled products, can improve sleep onset and continuity without the hangover effects of many conventional sleep aids.
Anxiety and Emotional Distress — The Weight of What’s Coming
Facing death is not like facing anything else. The anxiety of a terminal diagnosis is existential, not situational — it doesn’t respond to relaxation techniques the same way ordinary worry does. For some patients, there is genuine fear; for others, a sadness so pervasive it becomes its own kind of suffering.
Research in the palliative care literature suggests cannabis may help with this dimension of end-of-life suffering — not by eliminating the grief, but by allowing the nervous system to relax enough to be present rather than bracing. Some palliative care physicians note that low doses of THC produce what’s sometimes called a “psycholytic” effect — a gentle softening of the rigid defenses that can make it hard for a dying person to connect with what matters most to them.
In a large observational study of advanced cancer patients, 74.1% reported improvement in anxiety and depression after starting cannabis treatment, a figure that reflects the real-world experience of patients using cannabis not just for physical symptoms but for the full weight of what they’re carrying.
Honest About What Cannabis Cannot Do
Cannabis cannot reverse a terminal illness. It cannot extend life in any documented way. It cannot substitute for comprehensive palliative care, including access to pain specialists, social workers, chaplains, and the full team that good hospice and palliative programs provide.
There are also individual differences in how people respond. Some patients find cannabis deeply helpful for pain, nausea, or sleep. Others get limited benefit. A small number find the psychoactive effects uncomfortable, particularly those with anxiety who are sensitive to THC.
The principle that matters most at this stage of life is: start low, adjust gently, and stay in communication with your care team. The goal is more comfort, more presence, more of what makes life worth living in the time that remains. Cannabis is a tool in service of that goal — not a miracle, and not a substitute for the full support a person deserves at the end of life.
If You or Your Loved One Cannot Manage the Process
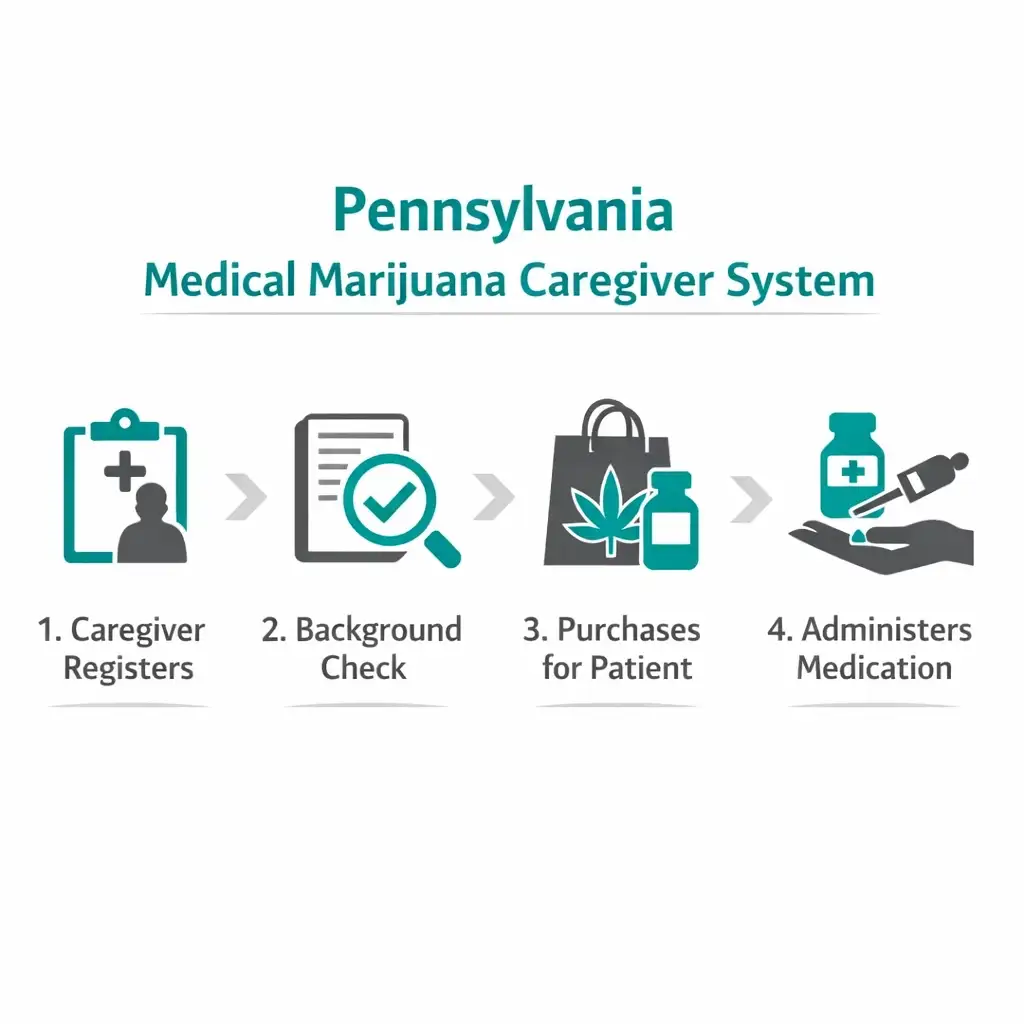
Pennsylvania’s caregiver pathway is essential for this population. Many terminal patients — particularly in later stages of illness — cannot drive to dispensaries, navigate websites, or physically manage the certification process. The PA MMJ program accommodates this.
A designated caregiver can be a spouse, adult child, partner, friend, or any trusted adult who is willing to register, pass a background check, and pick up medications from the dispensary on the patient’s behalf. The caregiver can do everything — register the patient, make dispensary visits, and administer the medication at home.
For patients who are homebound, too ill to attend even a telehealth appointment independently, or who need help completing paperwork, the certifying physician and caregiver can work together through the telehealth process with the caregiver present and actively participating.
Caregiver requirements:
- Must be 21 or older
- Must be a PA resident with valid PA driver’s license or state-issued ID
- Must have no drug-related criminal convictions in the past five years
- Must register with PA DOH and pass a background check
- $50 registration fee (waived for patients on Medicaid, SNAP, WIC, CHIP, PACE, PACENET)
- One patient can designate up to two caregivers
- Caregivers may purchase up to a 90-day supply at a time
A Note About Hospice Facilities and Care Settings
If your loved one is receiving care at an inpatient hospice facility, skilled nursing facility, or other care setting, it is worth knowing that individual facilities have their own policies about cannabis on-site, which may differ from Pennsylvania state law.
Pennsylvania law protects registered patients. But a specific facility may restrict cannabis use on their premises, require that it be administered only by registered caregivers rather than staff, or prohibit it altogether in their internal policies.
Before beginning cannabis, have a brief conversation with the facility’s director of nursing or medical director. Ask specifically: “What is your policy on patients using medical marijuana?” Knowing the answer in advance means no surprises at an already difficult time.
For patients receiving care at home, there are no facility restrictions. A registered caregiver can administer cannabis products in a home setting without limitation.
Practical Guidance: Products That Work at End of Life
For terminal patients — especially those who are elderly, frail, or already taking multiple medications — simplicity and low doses are most important.
Oral tinctures and oils are the best starting point. They can be added to food or drink, held under the tongue, or placed in the cheek pouch. They provide longer-lasting, more consistent relief than inhaled products and allow for accurate, small dosing. They are easy to administer by a caregiver.
Capsules are another option for patients who prefer a familiar pill format and can swallow without difficulty.
Vaporized products are available in Pennsylvania (vaporizing dry leaf or cartridges) but are harder to control for dose and require more ability to actively inhale — which may not be realistic for patients with respiratory limitations or who are very weak. They are better suited for patients who are still relatively active and want faster onset.
Start with the smallest dose available — 2.5mg THC equivalent or less — and observe for 24–48 hours before considering any increase. At end of life, less is almost always more. The goal is relief, not sedation.
Watch especially for dizziness and falls — cannabis can cause a temporary drop in blood pressure, particularly when standing. For any patient who is still mobile, this deserves attention.
Tell every care team member what cannabis products are being used and in what amounts, the same way you would disclose any other medication. This includes hospice nurses, the prescribing physician, and any emergency providers who may be involved.
How to Get a PA MMJ Card When Time Is Short
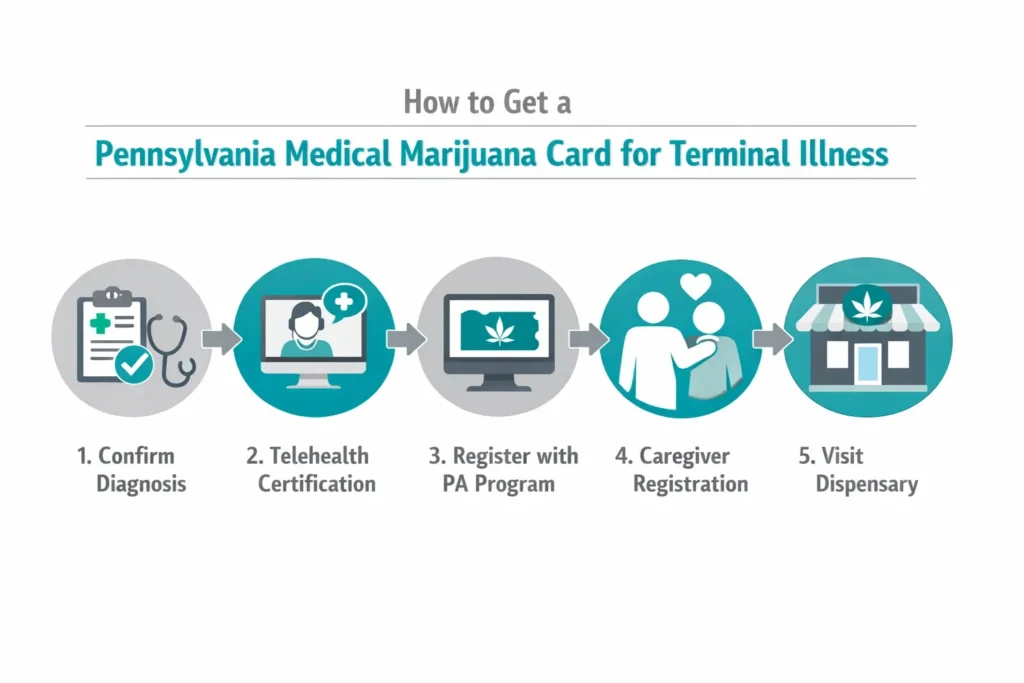
The process can move quickly when needed. A telehealth appointment typically takes 10–15 minutes. Cards are mailed within 7–14 days after the state registration fee is paid. For patients who may not have weeks to spare, the process can be prioritized.
Step 1 — Schedule the certification
Book a telehealth appointment with a PA DOH-registered medical marijuana physician. The patient’s caregiver or family member should be present. The certifying physician needs confirmation of the terminal diagnosis — a copy of recent medical records, a letter from the treating physician, or a hospice enrollment documentation all work.
Step 2 — Register with the PA DOH
After certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com). If the patient cannot do this themselves, the caregiver registers on their behalf using the “Caregiver Registering for a New Patient” option. The $50 registration fee applies; fee waivers are available for qualifying programs.
Step 3 — Caregiver background check
The caregiver completes a background check through the PA DOH portal. This typically takes 2–4 weeks. For patients with very limited time, it may be worth prioritizing this process as early as possible — even while other arrangements are still being made.
Step 4 — Dispensary visit
With caregiver card in hand, visit any PA dispensary. Tell the pharmacist clearly: “I’m picking up for a hospice patient. I need low-dose oral products for pain, nausea, and sleep.” A good dispensary pharmacist will guide you to appropriate products and doses.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Dyskinetic and spastic movement disorders
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
Frequently Asked Questions
Q: My loved one is in hospice. Does hospice enrollment affect eligibility?
Q: Does cannabis interact with morphine or other hospice medications?
Q: What if my family member can no longer make decisions for themselves?
Q: Is there a fast-track option for patients who are very ill?
Q: Can cannabis be used in a nursing home or long-term care facility?
Support for Families
If you are caring for someone at the end of life, please know that this is one of the most demanding things a person can do — and you deserve support too.
VSPA – Volunteer Services for Pennsylvania and the Pennsylvania Hospice Network can connect families with hospice and palliative care resources throughout the state.
Hospice Foundation of America (hospicefoundation.org) provides free caregiver resources, grief support, and end-of-life planning guidance at no cost.
Caring.com and CaringBridge (caringbridge.org) are practical platforms for organizing caregiver support and keeping family informed during illness.
NAMI Pennsylvania (nami.org/your-local-nami/nami-pennsylvania) offers mental health support for family members experiencing the emotional burden of caregiving and anticipatory grief.
Facing a terminal illness — your own or someone you love — is among the most profound things life asks of us. Pennsylvania’s medical marijuana program was designed with patients like this in mind: people carrying a burden that deserves every possible tool for relief.
NOTE: The PA MMJ card opens the door to cannabis products that may reduce pain, soften nausea, restore some appetite, bring better sleep, and ease the anxiety of the hours that feel heaviest. It doesn’t change what’s coming. But it can change how it feels to live through it — with more comfort, more presence, and more of the dignity that every person deserves in their final chapter.