
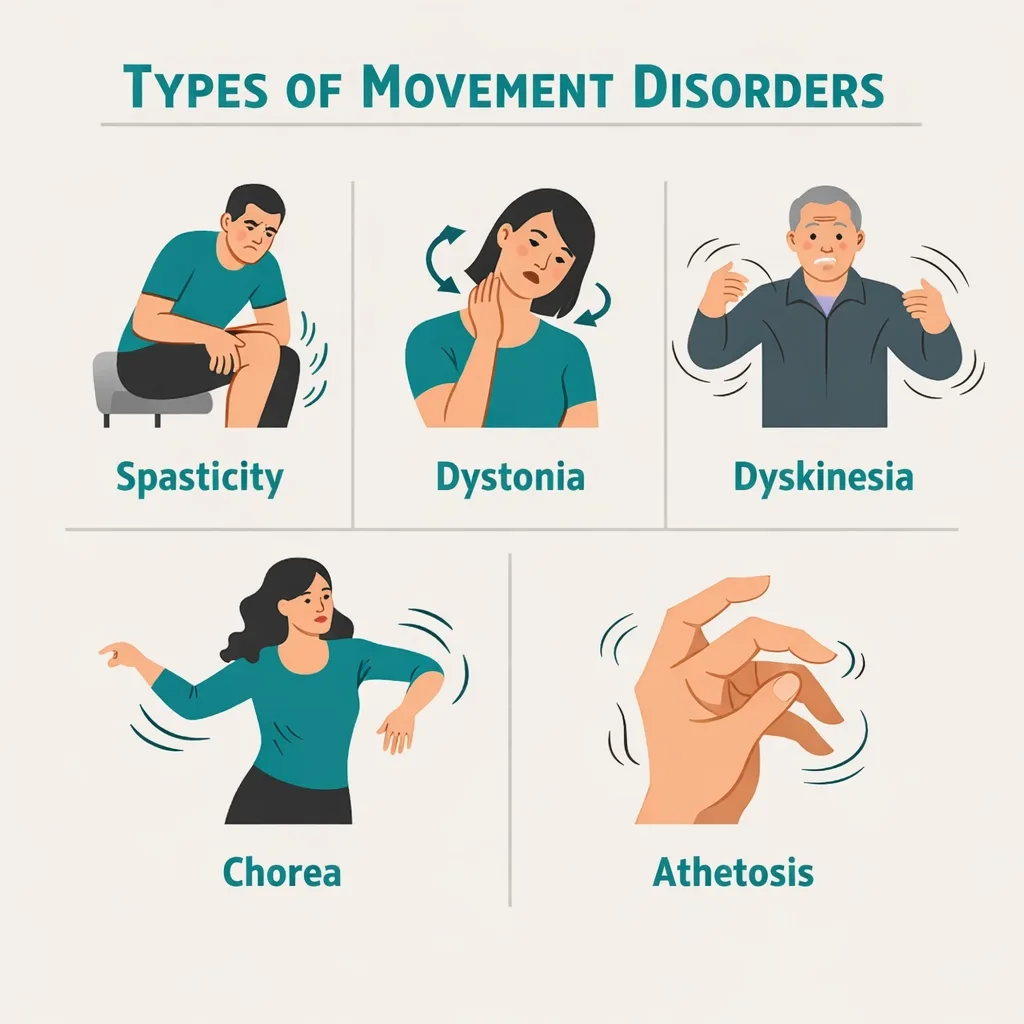
Living with a movement disorder means your body moves in ways you didn’t choose — and often can’t stop. Whether it’s the stiffness and painful muscle tightening of spasticity, the twisting involuntary postures of dystonia, the unpredictable writhing movements of chorea, or the medication-related jerks of dyskinesia, these conditions affect every part of daily life: getting dressed, eating, sleeping, holding a conversation, and simply sitting comfortably.
Pennsylvania includes dyskinetic and spastic movement disorders as a qualifying condition for its medical marijuana program — one of the most broadly written categories on the state’s list. If you have a diagnosis that involves abnormal, involuntary, or uncontrolled movements, there is a good chance it qualifies.
This page explains what conditions fall under this umbrella, what the evidence shows for different types of movement disorders (and where it’s honest about limitations), and how to get your PA MMJ card.
Does My Condition Qualify?
Pennsylvania’s Medical Marijuana Act lists “dyskinetic and spastic movement disorders” as an explicit qualifying condition. The state’s official list also includes a separate entry for multiple sclerosis, a separate entry for Parkinson’s disease, and a separate entry for damage to the central nervous system with intractable spasticity — so patients with those specific diagnoses have multiple pathways.
For the dyskinetic and spastic movement disorders category specifically, qualifying diagnoses include:
Spastic conditions — where muscles are stiff, tight, and resist movement:
- Spastic cerebral palsy (all types — diplegia, hemiplegia, quadriplegia, and mixed spastic/dyskinetic)
- Spasticity from spinal cord injury
- Spasticity from traumatic brain injury (TBI)
- Spasticity from stroke
- Hereditary spastic paraplegia (HSP)
- Primary lateral sclerosis (PLS)
Dyskinetic conditions — where muscles produce unwanted, involuntary movements:
- Dyskinetic cerebral palsy (including dystonic CP, choreoathetoid CP, athetoid CP)
- Dystonia (primary dystonia, cervical dystonia/torticollis, blepharospasm, Meige syndrome, generalized dystonia, DYT-gene dystonia disorders)
- Levodopa-induced dyskinesia (LID) — involuntary movements caused by long-term Parkinson’s medications
- Tardive dyskinesia (TD) — involuntary movements caused by long-term antipsychotic or anti-nausea medications
- Chorea not covered under other conditions (including drug-induced chorea)
- Athetosis (slow, writhing movements, often in cerebral palsy)
- Hemiballismus (large, flinging movements, usually following stroke or brain injury)
Mixed conditions — spasticity and dyskinesia together:
- Mixed cerebral palsy (the most common form — most people with CP have features of both)
- Conditions following brain injury or stroke with both spastic and dyskinetic components
If your diagnosis isn’t on this list but involves abnormal muscle tone, involuntary movements, or movement control problems, ask a certifying physician whether it falls within this qualifying category. The language is broad enough to accommodate many diagnoses not explicitly named above.
Note on overlap with other qualifying conditions: If your movement disorder is caused by multiple sclerosis, Parkinson’s disease, Huntington’s disease, or CNS tissue damage, those conditions have their own separate qualifying entries in Pennsylvania’s program. Your certifying physician may certify you under this condition, under the underlying diagnosis, or under both — all result in the same PA MMJ card.
- Source: Pennsylvania DOH – Medical Marijuana Patients: Qualifying Conditions
- Source: 28 Pa. Code Appendix A – Serious Medical Conditions
Why Cannabis and Movement Disorders: The Biology
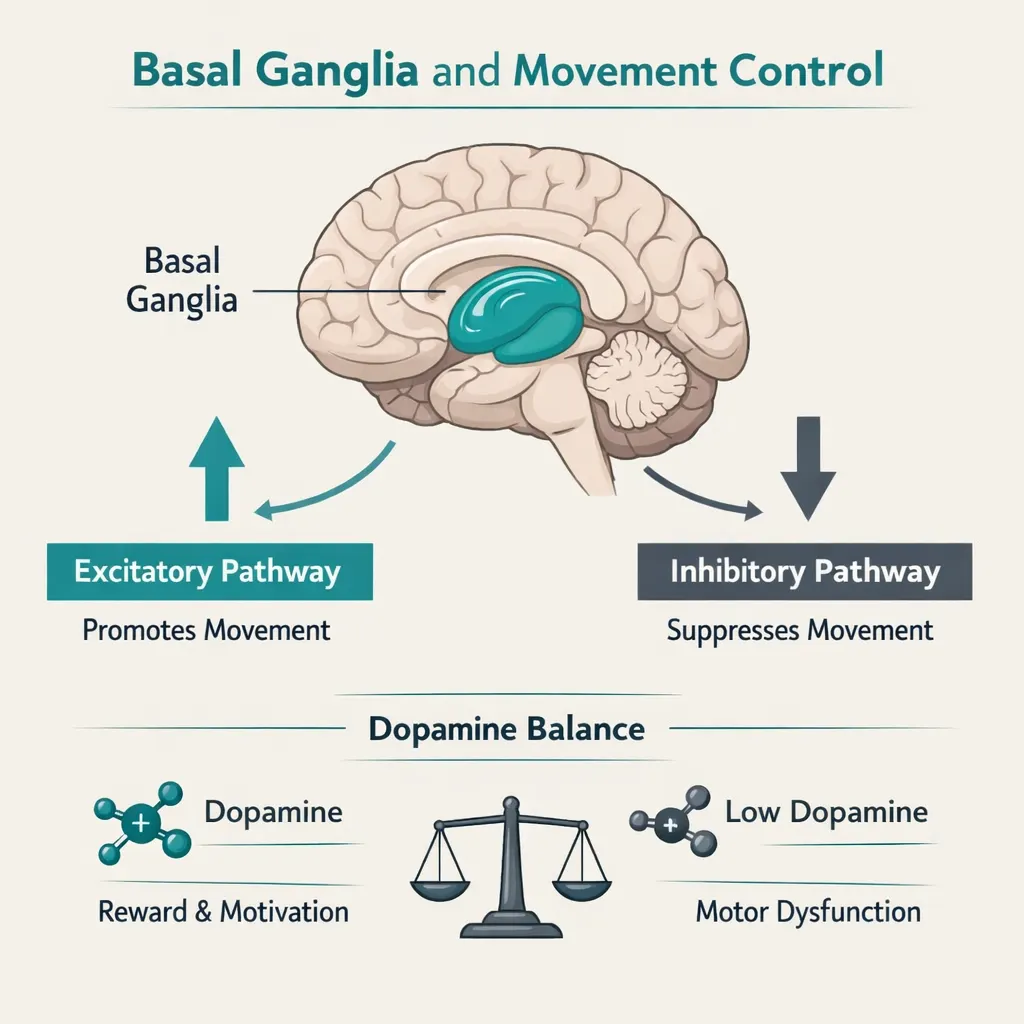
Cannabinoid receptors — particularly CB1 receptors — are concentrated in the basal ganglia, the deep brain structures that coordinate and regulate movement. The basal ganglia are the exact circuits that malfunction in most movement disorders. This is not a coincidence — it’s why researchers have been interested in cannabinoids for movement disorders for decades.
When the basal ganglia’s normal balance between movement-promoting and movement-suppressing signals breaks down, the result is either too much movement (dyskinesias, dystonia, chorea) or too little controlled movement (rigidity, spasticity). Endocannabinoids naturally help regulate this balance.
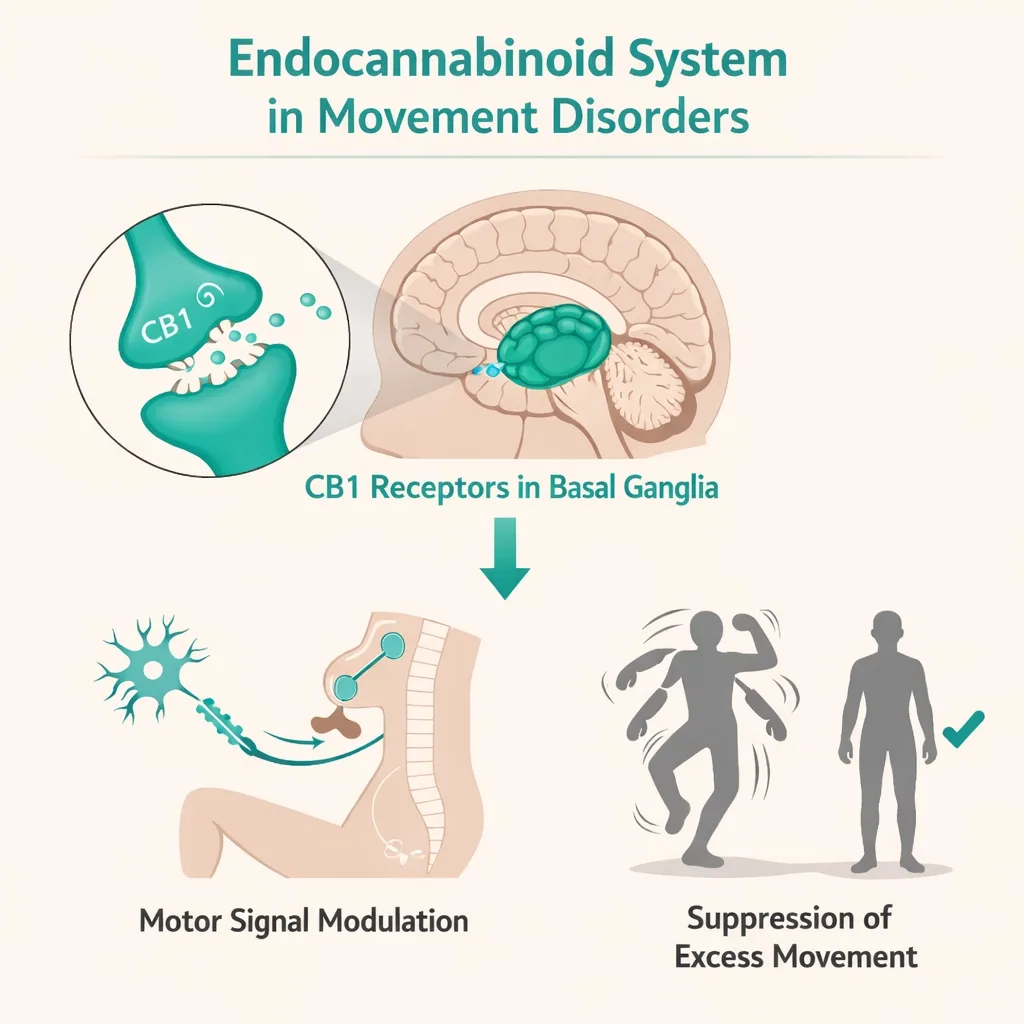
THC acts as a partial agonist at CB1 receptors throughout the basal ganglia. In states of excess movement, CB1 activation generally suppresses motor activity — which is why cannabis has potential in hyperkinetic (too-much-movement) disorders. For spasticity, CB1 activation in the spinal cord and brain reduces the exaggerated stretch reflexes that cause muscles to lock up.
This biology explains both the promise and the variability of cannabis in movement disorders: the circuit being targeted is right, but the specific condition, the stage of disease, and the patient’s individual cannabinoid receptor expression all affect how well it works.
What the Research Shows — Condition by Condition
Spasticity — The Strongest Evidence in Movement Disorders
Spasticity is the area where cannabinoids have their best-documented effectiveness across movement disorders. The American Academy of Neurology (AAN) Guideline Development Subcommittee reviewed all available clinical evidence and concluded:
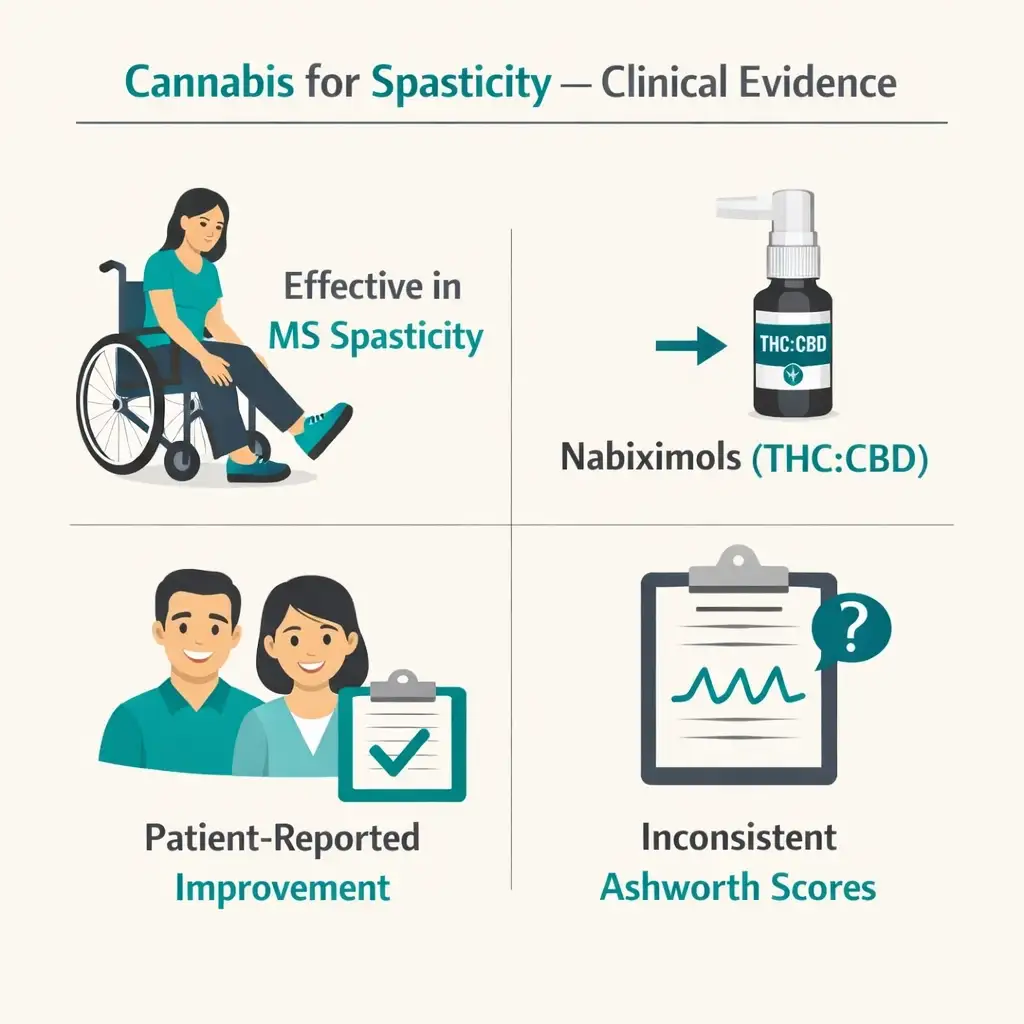
- Oral cannabis extract is effective for reducing patient-reported spasticity in multiple sclerosis
- Nabiximols (Sativex, the 1:1 THC:CBD oromucosal spray) and oral THC are probably effective for MS-related spasticity and painful spasms
- These effects are consistently found on patient-reported outcome measures, though clinical measurements on the modified Ashworth Scale (a doctor’s physical exam rating of muscle tone) show inconsistent improvement
Why the gap between what patients report and what doctors measure? This question runs through the spasticity literature. The current understanding is that cannabis may be reducing the subjective experience of spasticity — the pain, the discomfort, the sense of tightness — in ways that don’t fully reflect on a neurological exam score. For patients, this still matters enormously.
Nabiximols has been approved for MS-related spasticity in more than 30 countries outside the United States. In the UK, Canada, and across Europe, it is an accepted treatment for moderate-to-severe spasticity that doesn’t respond adequately to other medications.
For spasticity from causes other than MS — spinal cord injury, traumatic brain injury, stroke — the controlled clinical trial evidence is thinner, but patient surveys and real-world data consistently report benefit, and the mechanism supports its use.
- Source: PMC – AAN Systematic Review: Efficacy and Safety of Medical Marijuana in Selected Neurologic Disorders
- Source: PMC – Symptomatic Therapy in Multiple Sclerosis: The Role of Cannabinoids in Treating Spasticity
Cerebral Palsy — A Mixed but Encouraging Picture
Cerebral palsy is the most common movement disorder of childhood, and the research on cannabis in CP is growing — but not yet conclusive.
The encouraging data
A study from Israel (published in the Journal of Child Neurology) administered low-THC, high-CBD cannabis products to 25 patients with complex movement disorders including cerebral palsy over five months. Researchers noted significant improvement in spasticity and dystonia, sleep difficulties, pain severity, and quality of life in the total cohort. The majority of participants continued treatment after the study ended. A second Israeli study at Wolfson Medical Center focused specifically on dyskinetic CP with similarly promising results.
The tempering data
A more recent rigorous trial — a double-blind, placebo-controlled study published in 2024, conducted at the University Medical Centre Ljubljana in Slovenia — enrolled 53 children and adolescents with spastic CP (grades IV and V, the most severely affected). The treatment was a 10:1 CBD:THC full-spectrum cannabis oil added to existing therapy for six weeks. The primary outcome — change in spasticity measured by the modified Ashworth Scale — showed no statistically significant improvement over placebo. The product was well-tolerated, with no severe side effects. Quality of life parameters also did not significantly improve.
How to hold both findings
These studies used different products (Israeli: varied low-THC/high-CBD formulations; Slovenian: standardized 10:1 CBD:THC oil), different severities, different measurement tools, and different durations. The honest reading is that cannabis may help some CP patients — particularly with pain, sleep, and subjective experience of spasticity — while not consistently improving objective clinical scores. For families managing CP, this may still represent meaningful real-world benefit, even if it doesn’t show up on a standardized scale.
- Source: PMC – Efficacy and Safety of Medical Cannabinoids in Children with Cerebral Palsy: A Systematic Review (2023)
- Source: ScienceDirect – Plant-Derived Cannabinoids for Treatment of Spasticity in Children and Adolescents with Severe Cerebral Palsy: Double-Blind, Placebo-Controlled Trial (2024)
Levodopa-Induced Dyskinesia in Parkinson’s — An Honest Finding
This is one of the most important honest disclosures in this entire qualifying category, and the one no competing PA MMJ page bothers to make.
Levodopa-induced dyskinesia (LID) — the involuntary writhing or jerking movements that develop after years of Parkinson’s treatment with levodopa — seems like a natural target for cannabinoids, because the basal ganglia biology points that way. And some early animal models were encouraging.
But the clinical trial evidence in humans is not supportive. The AAN’s systematic review concluded that oral cannabis extract is probably ineffective for treating levodopa-induced dyskinesias in Parkinson’s disease. This is based on a Class I randomized controlled trial of 19 Parkinson’s patients, which found no objective or subjective improvement in dyskinesias. A more recent 2024 review in the Journal of Parkinson’s Disease (Fox and Freitas) confirmed: “For levodopa-induced dyskinesia the evidence is that cannabinoids do not significantly reduce symptoms.”
This doesn’t mean cannabis has nothing to offer Parkinson’s patients. For the separate symptoms of pain, sleep disruption, anxiety, and general quality of life in PD, the picture is more positive. But for LID specifically — the involuntary movements — the controlled evidence says it probably doesn’t work, and patients and prescribers deserve to know that.
Patients with Parkinson’s disease who want to use cannabis for LID should have an honest conversation with their neurologist before proceeding, and should not reduce or stop levodopa based on any perceived cannabis effect.
- Source: PMC – AAN Systematic Review: Efficacy and Safety of Medical Marijuana in Selected Neurologic Disorders
- Source: Sage Journals – Advice to People with Parkinson’s in My Clinic: Cannabis (Fox and Freitas, Journal of Parkinson’s Disease, 2024)
Tardive Dyskinesia — An Emerging Option
Tardive dyskinesia (TD) is caused by long-term use of medications that block dopamine — primarily antipsychotics and some anti-nausea drugs. It produces involuntary movements, typically affecting the face (repetitive mouth movements, tongue protrusion, lip smacking), trunk, and limbs that often persist even after the offending medication is stopped.
Current FDA-approved treatments for TD (valbenazine/Ingrezza and deutetrabenazine/Austedo) are effective but expensive and not universally accessible. Cannabis represents an off-label option that some patients have found helpful, though controlled trial evidence in TD specifically is limited. The endocannabinoid mechanism — modulating dopamine signaling in the basal ganglia — is biologically plausible. Case reports and patient surveys show a range of responses. For PA patients with TD who have not found adequate relief with approved treatments, the PA MMJ card gives access to a low-risk adjunctive option worth discussing with the prescribing physician.
Dystonia — Early Signals, More Research Needed
Dystonia — where muscles contract involuntarily into twisting, repetitive movements or abnormal postures — has a biologically compelling cannabinoid target: CB1 receptors in the basal ganglia are directly involved in the circuits that go wrong in dystonia.
Clinical evidence is limited. Several small case series and surveys have shown benefit from oral CBD and oral cannabis extracts in patients with generalized dystonia, cervical dystonia, and secondary dystonia in conditions like Wilson’s disease. However, the two small randomized controlled trials specifically targeting dystonia showed no statistically significant benefit. The gap between anecdotal reports and trial results likely reflects the small sample sizes, heterogeneity of dystonia types, and the challenge of measuring a condition that varies so much from patient to patient.
For PA patients with dystonia whose symptoms are not adequately controlled by conventional therapies (injections of botulinum toxin, oral baclofen, trihexyphenidyl, or deep brain stimulation where indicated), cannabis is a reasonable adjunctive option with a favorable safety profile.
What Cannabis Can Help With (Beyond Just Movement)

Even in cases where the direct movement-reducing effect of cannabis is uncertain, there are secondary symptoms of movement disorders where cannabis has stronger and more consistent evidence:
Pain: Most forms of spasticity are painful — the constant muscle tension, the spasms that wake you at night, the joint compression from dystonic postures. Cannabis is one of the most consistently effective pain relievers for musculoskeletal and neuropathic pain, and movement disorder pain is a legitimate primary target regardless of whether the movement itself improves.
Sleep: People with spasticity and dystonia frequently have severely disrupted sleep — muscle spasms wake them, posturing makes comfortable sleep impossible, and the overall physical burden of the condition carries into the night. Cannabis’s sleep-promoting effects are well-documented and represent one of the most realistic quality-of-life benefits for this population.
Anxiety and psychological distress: Living with a movement disorder that affects how you appear in public, how you can communicate, and how much you can independently do creates real and significant anxiety. For patients whose anxiety compounds their movement disorder symptoms (anxiety typically worsens dystonia and spasticity), cannabis addressing the anxiety can have meaningful indirect effects on the movement symptoms as well.
Appetite and nutrition: People with severe cerebral palsy, dystonia, or spasticity may have difficulty eating due to the physical demands of chewing and swallowing, and may have elevated caloric needs from constant muscle activity. Cannabis’s appetite-stimulating properties directly address this.
PA Dispensary Guidance: What to Look For
For spasticity
THC-dominant or balanced THC:CBD oral products are the most evidence-supported formulations. Oral tinctures or capsules taken before periods of anticipated spasm (e.g., before physical therapy, before sleep) allow for planned relief. Start at 2.5–5mg THC equivalent and titrate slowly. Vaporized forms act faster but shorter, which suits breakthrough spasms when immediate relief is more important than duration.
For pain from spasticity or dystonia
The same THC-dominant approach applies for pain. CBD-dominant products at higher doses (20–40mg CBD) are appropriate for patients who want to avoid psychoactive effects or who are using cannabis primarily for background pain management.
For sleep disruption
Moderate oral THC doses (5–10mg) 1–2 hours before sleep work better than doses taken at bedtime, as oral onset is slower. Drowsiness the following morning is a common side effect at higher doses — start low.
For levodopa-induced dyskinesia specifically
Based on the clinical evidence reviewed above, patients should have realistic expectations. If you wish to try cannabis for LID, discuss it with your neurologist, start very low, and treat any perceived benefit as preliminary pending your own experience.
Tell the dispensary pharmacist your specific movement disorder. “I have spastic CP” and “I have tardive dyskinesia from antipsychotics” and “I have LID from Parkinson’s” will lead to different product recommendations. Be specific.
How to Get Your PA MMJ Card
Step 1 — Confirm your diagnosis
Have documentation of your movement disorder diagnosis available for the certifying appointment. This can be a letter from your neurologist, recent medical records, or prior prescription records for movement disorder medications.
Step 2 — Schedule a telehealth certification
Book an appointment with a PA DOH-registered medical marijuana physician. The telehealth consultation typically takes 10–15 minutes. The certifying physician confirms your qualifying diagnosis and discusses your symptoms and goals.
Step 3 — Register with the PA DOH
After certification, register at the PA Medical Marijuana Program Patient Registry (patientportal.mmapinc.com) with your certification, a valid PA driver’s license or state-issued ID, and the $50 annual fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 4 — Caregiver pathway if needed
Patients with severe movement disorders who cannot drive, cannot navigate websites independently, or who need assistance at the dispensary can designate a caregiver. The caregiver registers separately, completes a background check ($50 fee), and can purchase and administer cannabis on the patient’s behalf. See the caregiver registration page for full details.
Step 5 — First dispensary visit
Tell the dispensary pharmacist your specific movement disorder, the symptoms you’re targeting (spasticity, pain, sleep, dyskinesias), and any other medications you take. Ask specifically about starting doses for your situation.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Tourettes
- Chronic Hepatitis C
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions
- Anxiety Disorder
Frequently Asked Questions
Q: I have cerebral palsy with both spasticity and dyskinesia (mixed CP). Which qualifying condition do I use?
Q: I have tardive dyskinesia from antipsychotic medication. My psychiatrist manages my mental health treatment. How do I navigate this?
Q: My child has severe spastic quadriplegia. Can they get a PA MMJ card?
Q: Will cannabis help my involuntary movements directly, or just the pain and other symptoms?
Q: Can I use cannabis alongside baclofen or other spasticity medications?
Support Resources
United Cerebral Palsy of Pennsylvania (ucppa.org) provides advocacy, education, and support services for people with cerebral palsy and their families across the Commonwealth.
Dystonia Medical Research Foundation (dystonia-foundation.org) offers patient education, support group connections, and research updates for all forms of dystonia.
Parkinson’s Foundation (parkinson.org) maintains an extensive knowledge base on levodopa-induced dyskinesia, treatment options, and the current state of cannabis research in Parkinson’s disease.
National Organization for Rare Disorders (NORD) (rarediseases.org) provides condition-specific information for less common movement disorders including hereditary spastic paraplegia, Wilson’s disease, and other rare dystonias.
NAMI Pennsylvania (nami.org/your-local-nami/nami-pennsylvania) for patients with tardive dyskinesia whose movement disorder developed in the context of mental health treatment.
NOTE: Movement disorders are among the most physically demanding conditions in medicine — they take over the body, exhaust muscles that never get to rest, and demand constant adaptation from patients and their families. Cannabis doesn’t solve any of that, and this page has been honest about where the evidence is weaker than hope would have it be.
But for the pain that never goes away, the sleep that never comes easily, the anxiety that compounds every symptom, and the spasticity that makes every movement a negotiation — cannabis has real, documented, and increasingly well-understood effects. Pennsylvania’s program is the legal pathway to access those effects. The qualifying category is broad, the evidence base for spasticity is solid, and the caregiver pathway ensures access even for those with the most severe forms of these conditions.