
Recovery is not a straight line. Anyone who has lived it — or loved someone through it — already knows that. There are medications that help and don’t work for everyone. There are treatment programmes with waiting lists. There are days when everything that is supposed to help feels like it is almost enough, but not quite. And there are the cravings that arrive without warning — triggered by a smell, a street, a song — and have to be managed without a playbook.
If you have opioid use disorder and conventional treatments have not been enough, or you are looking for something to support the treatment you are already in, Pennsylvania has opened a specific, legal door for you.
Opioid use disorder is an explicitly named qualifying condition under Pennsylvania’s Medical Marijuana Act. It is one of the most forward-thinking inclusions on the entire qualifying list — and this page explains what it means, who qualifies, what the research honestly shows, and how to use a PA MMJ card as part of a recovery approach that actually works for your life.
Does Opioid Use Disorder Qualify for a PA MMJ Card?
Yes. The full qualifying condition under the Pennsylvania Medical Marijuana Act (Act 16 of 2016) is:
“Opioid use disorder for which conventional therapeutic interventions are contraindicated or ineffective, or for which adjunctive therapy is indicated in combination with primary therapeutic interventions.”

This carefully worded language covers three distinct situations:
Conventional treatments are contraindicated — meaning standard medications for opioid use disorder (buprenorphine, methadone, naltrexone) are medically not appropriate for you. This might be due to a specific medical condition, a documented adverse reaction, or a drug interaction that makes those medications unsafe.
Conventional treatments are ineffective — meaning you have tried standard medications for opioid use disorder and they have not provided adequate benefit. You have engaged with the available treatments and they are not working well enough.
Adjunctive therapy alongside primary treatment — meaning you are currently in treatment with buprenorphine, methadone, naltrexone, or another primary intervention, and you want to use cannabis as a complementary tool alongside it.
The third pathway is the most commonly applicable. It means you do not need to have failed treatment or be unable to tolerate standard medications. If you are currently in medication-assisted treatment and want to explore cannabis as a supplementary tool — for cravings, anxiety, sleep, pain, or other factors that affect your recovery — you may qualify.
Sources:
- Pennsylvania Department of Health – Medical Marijuana Qualifying Conditions
- 28 Pa. Code Appendix A – Serious Medical Conditions
The Pennsylvania Context: Why This Qualifying Condition Exists
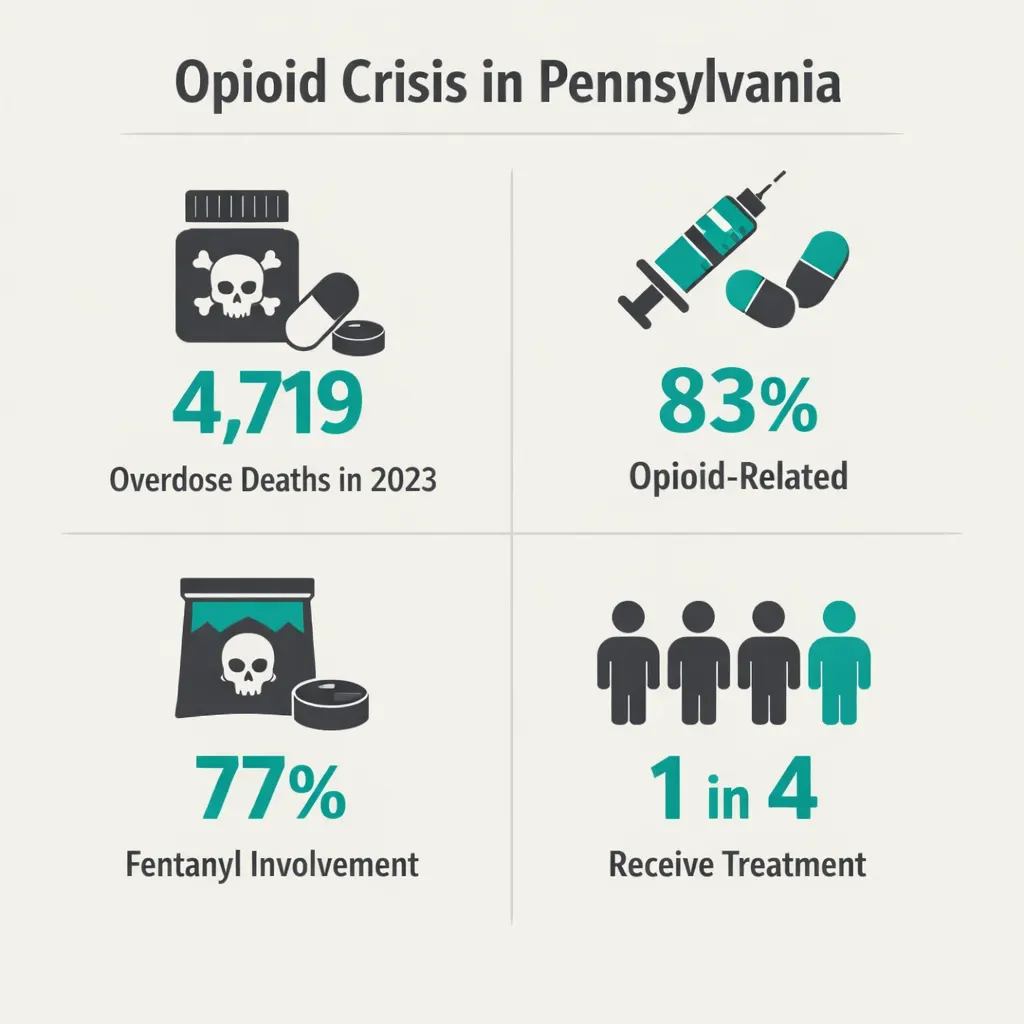
Pennsylvania has been one of the hardest-hit states in the opioid epidemic. In 2023 alone, 4,719 Pennsylvanians died from drug overdoses — approximately one person every two hours. Of those deaths, 83% were opioid-related and nearly 77% involved fentanyl.
Despite those numbers, treatment remains inaccessible for too many people. Only about one in four Pennsylvanians who needed treatment for opioid use disorder were receiving it. Buprenorphine access has improved significantly since federal X-waiver requirements were eliminated in 2023, but barriers remain — stigma from providers and pharmacies, geographic access in rural areas, cost, and the practical reality that no single treatment works for everyone.
Pennsylvania recognised this reality when it wrote opioid use disorder into its medical marijuana qualifying conditions. The state was not endorsing cannabis over buprenorphine or methadone — the gold-standard medications for OUD, which remain the first-line evidence-based treatments. It was acknowledging that for a subset of patients, conventional options are not enough, not tolerated, or not accessible — and that a broader toolkit serves people better.
Sources:
- Pennsylvania Department of Health – Opioid Crisis Data
- NIDA – To Address the Fentanyl Crisis, Greater Access to Methadone Is Needed (2024)
Before Anything Else: The Most Important Thing to Say
Buprenorphine (Suboxone) and methadone are the most effective treatments for opioid use disorder that currently exist. They reduce overdose deaths, reduce illicit opioid use, improve social functioning, and save lives. If you are not currently on one of these medications and have opioid use disorder, please talk to a doctor or addiction specialist about them before anything else.
Cannabis is not a replacement for buprenorphine or methadone. The evidence for CBD and cannabis in OUD is real and growing — but it does not yet compare to the evidence base for these medications. If you are in medication-assisted treatment (MAT) and it is working, do not stop it in favour of cannabis.
This is not a formality — it is clinically important. And it is possible to hold it alongside everything else this page says.
With that said — not everyone responds to standard treatments. Not everyone can access them. Not everyone can tolerate them. For those people, and for those already in treatment who want a complementary tool, the evidence for cannabis in OUD is worth understanding honestly.
What the Research Shows
CBD and Heroin Cravings: The Landmark Study
The most important clinical trial in cannabis and OUD was published in the American Journal of Psychiatry in 2019 by researchers at the Icahn School of Medicine at Mount Sinai, led by addiction neuroscientist Dr. Yasmin Hurd.
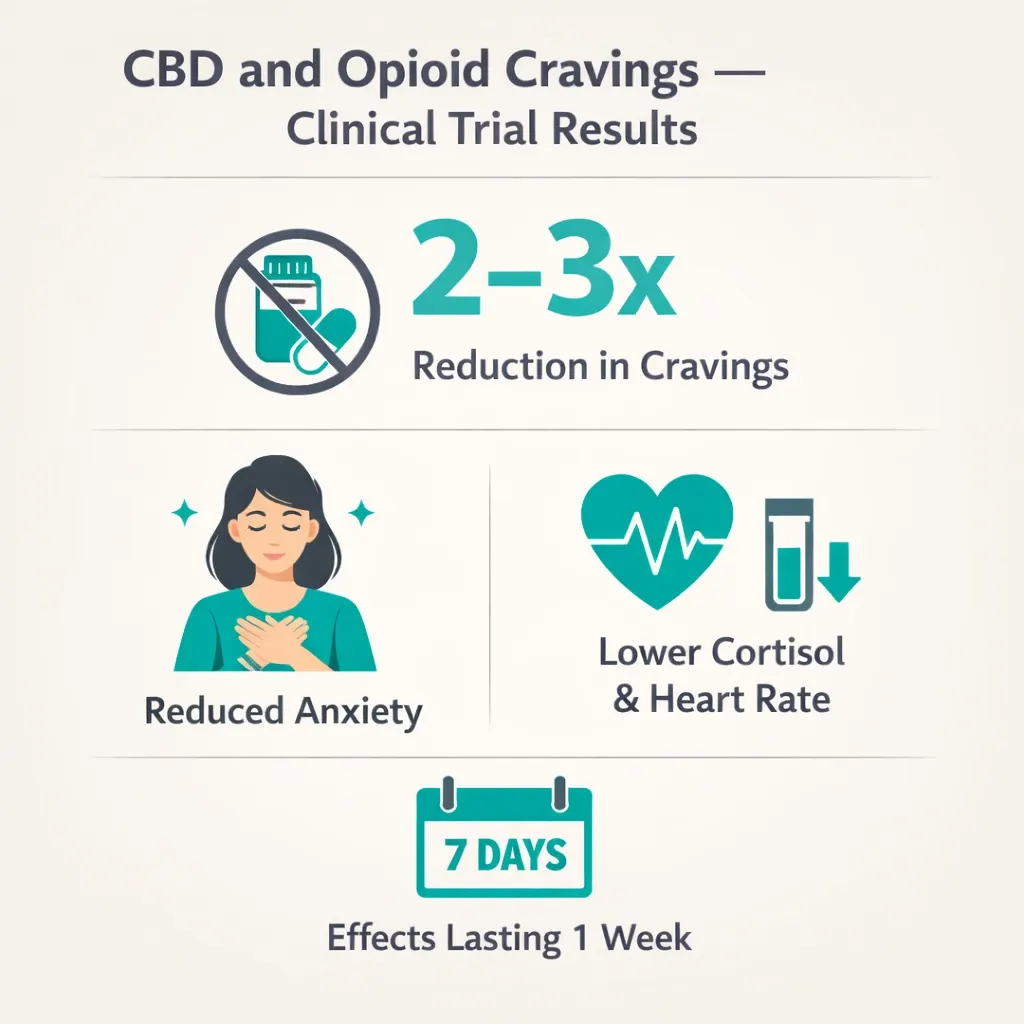
This was a double-blind, randomised, placebo-controlled trial — the gold standard study design — involving 42 drug-abstinent individuals with heroin use disorder. Participants received either 400 mg CBD, 800 mg CBD, or placebo once daily for three consecutive days and were then exposed to neutral cues and drug-related cues (videos of drug use and heroin paraphernalia) to trigger cravings.
The results were striking. Compared to placebo, CBD significantly reduced both craving and anxiety induced by the drug cues — with effects persisting one week after the final dose, when little CBD would be expected to remain in the body. Those who received CBD had a two to three times reduction in cravings compared to the placebo group at the seven-day follow-up. The researchers also measured physiological stress responses — heart rate and cortisol levels — and found that CBD objectively reduced both, confirming the effect was not simply self-reported.
Dr. Hurd described the significance: “The intense craving is what drives the drug use. If we can have medications that dampen that, that can greatly reduce the chance of relapse and overdose risk.” She explicitly called for this as the basis for further investigation of CBD as an OUD treatment option — which the NIH HEAL Initiative subsequently funded.
What This Means in Plain Terms
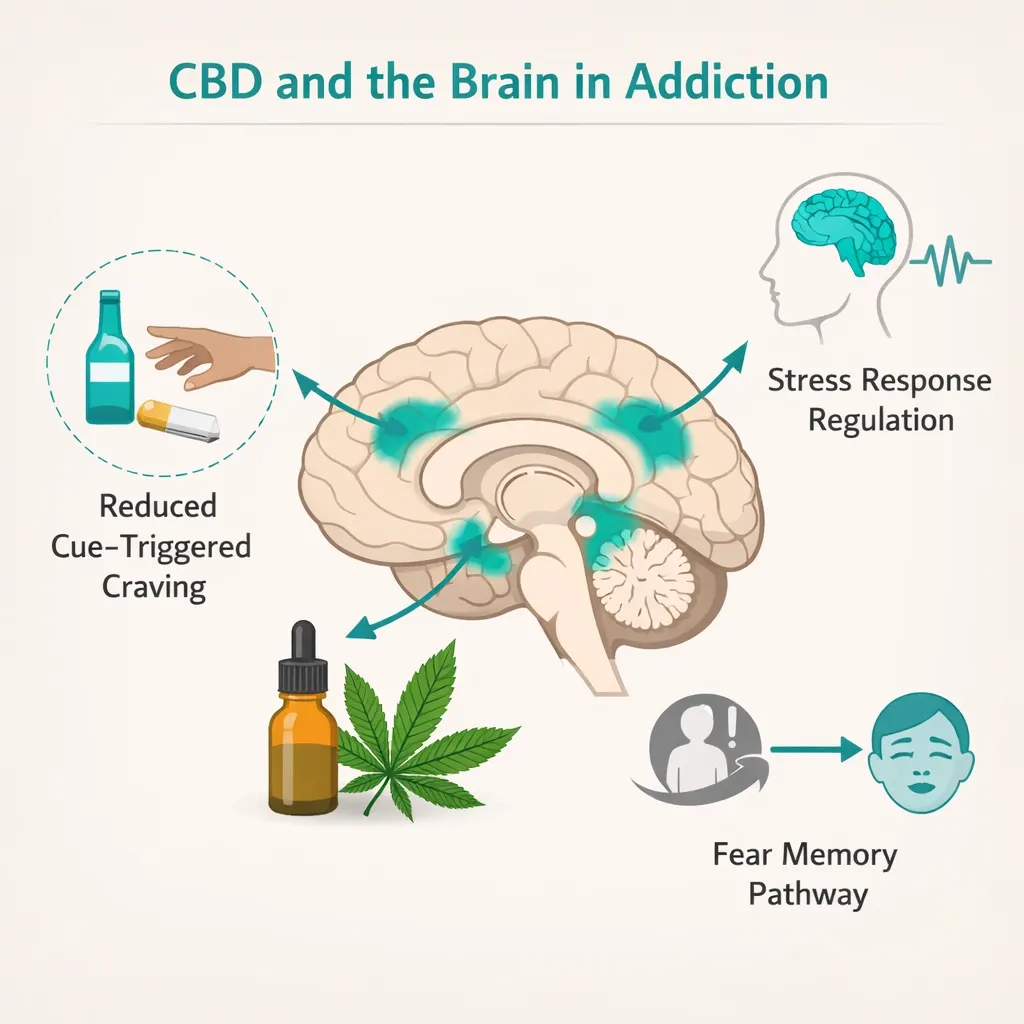
The craving triggered by environmental cues — seeing a place where you used to use, a person you used with, an object associated with using — is one of the most powerful drivers of relapse. It is not a choice or a failure. It is a neurological response. CBD, in this study, reduced that neurological response both subjectively (what participants reported feeling) and objectively (what their bodies measured).
The effects lasting a week after the last dose is particularly significant. It suggests CBD may do something in the brain — changing the way the fear and craving circuitry responds to cues — rather than simply providing temporary relief during the moment of use.
Broader Evidence on Cannabis and Opioid Use Disorder
Beyond the CBD craving trial, several other evidence threads are relevant for Pennsylvania patients:
A 2024 systematic review published in Pain and Therapy synthesised the available evidence on medicinal cannabis for OUD, concluding that both preclinical and observational data support cannabis-based products as a potential emerging therapy for managing opioid addiction. Studies have found cannabis may reduce opioid cravings and withdrawal effects and may be considered as an adjunct or standalone option alongside current medications for opioid use disorder. The review emphasised the need for more rigorous randomised trials — which are ongoing.
A 12-month qualitative study published in Harm Reduction Journal (2025) interviewed OUD patients with chronic pain who were on buprenorphine and using medical cannabis as an adjunct. Key themes at 12 months included meaningful improvements in pain management, reductions in anxiety and mood disturbance, improvements in sleep quality and duration, and reductions in cravings for illicit drugs. Patients described medical cannabis as enabling them to better manage the combination of OUD and chronic pain — two conditions that are frequently co-occurring and mutually reinforcing.
An important 2023 Canadian study analysed data from a 24-week trial of 272 patients with OUD on buprenorphine/naloxone or methadone. It found that recent cannabis use was not associated with worse opioid use, craving, or withdrawal in people receiving medication for OUD. This is relevant because it directly addresses the concern that cannabis use might undermine buprenorphine or methadone treatment — this study found it did not.
Sources:
- PMC – The Role of Medicinal Cannabis as an Emerging Therapy for Opioid Use Disorder (2024)
- Harm Reduction Journal – Motivation and Experiences of OUD and Chronic Pain Patients Using Medical Cannabis for 12 Months (2025)
- NCBI – Cannabis for Opioid Use Disorder: Review of Evidence
Cannabis for Pain in OUD — A Critical Overlap
Chronic pain is one of the most common co-occurring conditions in opioid use disorder. Many people develop OUD because they were prescribed opioids for legitimate pain and dependency followed. Others developed OUD independently and also have chronic pain. Either way, unmanaged pain is one of the biggest drivers of relapse — because opioids provide the pain relief that nothing else has.
Cannabis has meaningful evidence for pain relief — particularly neuropathic and chronic pain — which is directly relevant for OUD patients whose opioid use was driven by pain. Managing pain through a non-opioid alternative that does not drive the same neurological dependency cycle is one of the most clinically coherent reasons to integrate cannabis into an OUD treatment plan.
What Honest Uncertainty Looks Like Here
The evidence for cannabis in OUD is promising but not settled. The CBD craving trial involved 42 participants. The observational studies have methodological limitations. There are not yet large, long-term RCTs of cannabis or CBD as an adjunct to standard OUD treatment in real-world conditions.
This does not mean the evidence does not exist or does not matter — the CBD craving trial is a properly designed RCT with meaningful results, and the preclinical, observational, and early clinical evidence all points in a consistent direction. It means that anyone managing OUD should be doing so with their treatment team — doctor, addiction specialist, therapist — and cannabis should be one tool in a broader approach, not the whole approach.
THC, CBD, and OUD — Which Matters Most?
For the specific OUD applications — craving reduction, anxiety management, sleep — the evidence points in different directions for THC and CBD.
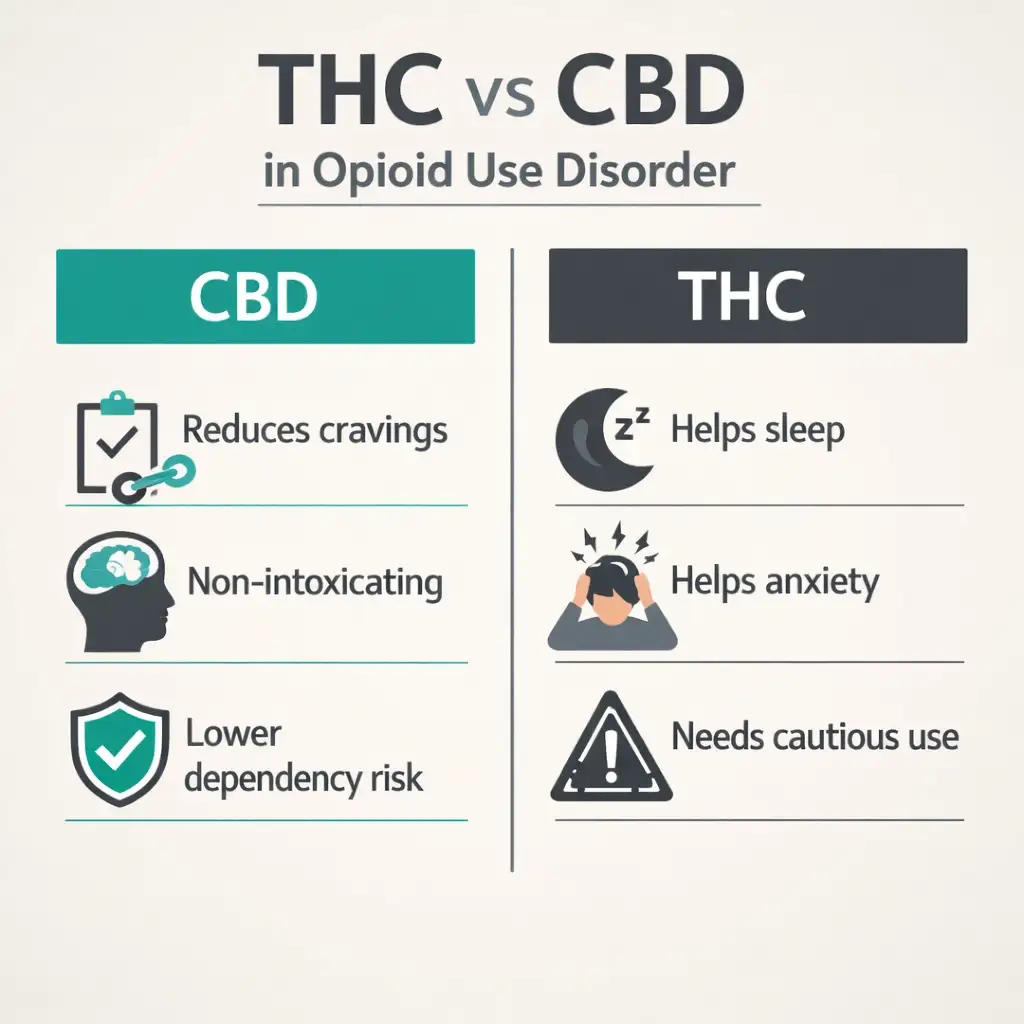
CBD is the primary compound of interest for craving reduction. The landmark Mount Sinai trial used CBD specifically. CBD is non-intoxicating, does not activate the opioid reward pathway, and does not carry the same dependency risk as THC. For patients in recovery who want to avoid any psychoactive effect — including for reasons of personal recovery philosophy or 12-step programme participation — CBD-dominant products are the most appropriate choice.
THC plays a supporting role for anxiety, sleep, and pain management. For OUD patients whose craving triggers are deeply connected to anxiety, or who struggle with sleep disruption that increases relapse risk, the combination of CBD with modest amounts of THC may be more effective than CBD alone. Balanced 1:1 products are appropriate for this.
High-THC products carry specific caution in OUD. There is evidence that heavy THC use can impair the effects of buprenorphine and may have complex interactions with the dopamine and reward systems involved in addiction. Very high-THC dispensary products used heavily are not the appropriate choice for this qualifying condition. Moderate doses, CBD-dominant or balanced ratios, and consistent use patterns under physician awareness are the appropriate approach.
PA Dispensary Product Guidance for Opioid Use Disorder
For Craving Management
CBD-dominant tinctures or capsules at meaningful doses (20–40 mg CBD equivalent) are the most evidence-aligned choice for craving management between episodes. Based on the Mount Sinai trial, CBD’s anti-craving effects appear to persist beyond the dosing period, suggesting regular daily use rather than only crisis-time use may be more effective.
For acute cue-induced craving moments, sublingual CBD tinctures have a faster onset (15–30 minutes) than capsules and can serve as a rapid intervention when environmental triggers are encountered.
For Anxiety and Sleep
Anxiety and sleep disruption are among the most common factors that drive relapse. Balanced 1:1 THC:CBD products in low to moderate doses taken in the evening are appropriate for patients managing anxiety and sleep issues alongside OUD recovery. Start with 2.5–5 mg THC equivalent. Keep doses modest and consistent.
For Chronic Pain Co-Occurring with OUD
For patients where chronic pain is a significant factor in their OUD, balanced products with meaningful CBD and modest THC addressing the pain directly are appropriate — following the same guidance as the chronic pain qualifying condition page. The goal is adequate pain management through a non-opioid mechanism that supports rather than undermines recovery.
What to Avoid
Avoid high-THC products used heavily. Avoid using cannabis as a crisis replacement for emergency naloxone — cannabis does not reverse overdose. Avoid stopping buprenorphine or methadone to substitute cannabis — this is clinically dangerous and not supported by evidence.
What Your Recovery Programme or Sponsor Might Think
This is a real consideration for many people in recovery, especially those participating in 12-step programmes like Narcotics Anonymous (NA) or Alcoholics Anonymous (AA). These programmes traditionally take a complete abstinence position, including from cannabis. Some members and sponsors will view a PA MMJ card as inconsistent with sobriety.
This is a genuinely personal decision that only you can make, in conversation with your treatment team and with awareness of your own recovery history and what it requires. Some people in buprenorphine-assisted recovery also navigate this tension with 12-step programmes. There are also SMART Recovery and other non-abstinence-based frameworks that do not take the same position.
What medicine says and what a recovery fellowship says are not always the same thing. Both perspectives matter for different reasons. A PA MMJ card is a medical choice, not a declaration about your recovery values. How you integrate it — with your doctor, with your support network, with honesty about what helps and what hinders — is your own.
Drug Interactions: Cannabis and OUD Medications
Buprenorphine/naloxone (Suboxone) — The 2023 Canadian study found no adverse interaction between recent cannabis use and buprenorphine/naloxone treatment. No pharmacokinetic interaction that meaningfully alters buprenorphine levels has been identified. However, both buprenorphine and THC can cause sedation — monitor for additive drowsiness, particularly with higher-THC products.
Methadone — Both methadone and THC are metabolised through CYP3A4. CBD is a CYP3A4 inhibitor and could theoretically increase methadone plasma levels. This interaction is not well-characterised clinically for typical dispensary CBD doses but warrants awareness. Tell your methadone clinic prescriber before adding any cannabis product — they need to know, both for safety monitoring and because some programmes have policies on cannabis use.
Naltrexone (Vivitrol) — Naltrexone blocks opioid receptors and does not interact with the endocannabinoid system directly. Cannabis and naltrexone can generally be co-used without pharmacokinetic concern. Cannabis may support sleep, anxiety, and wellbeing that complements naltrexone’s receptor-blocking mechanism.
Antidepressants and anxiolytics — Many OUD patients manage co-occurring depression and anxiety. CBD inhibits CYP2D6, which metabolises some antidepressants. Discuss with your prescribing physician before adding CBD.
How to Get Your PA MMJ Card for Opioid Use Disorder
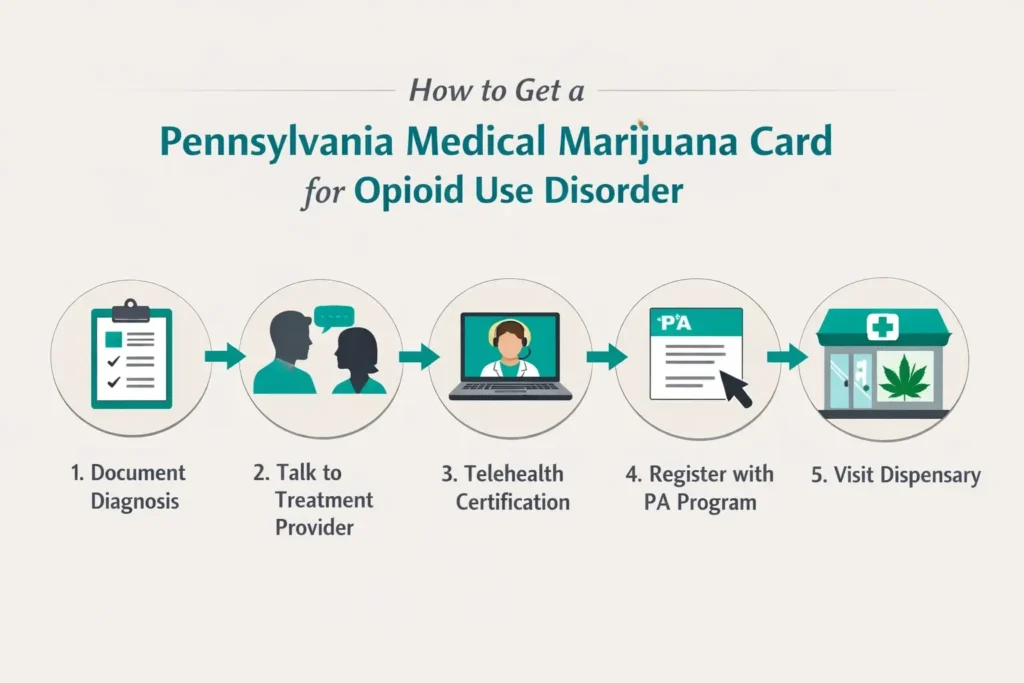
Step 1 — Document your OUD history and treatment.
You need documentation of an opioid use disorder diagnosis from a physician, addiction specialist, or mental health provider. This might be records from a treatment programme, a prescribing physician’s notes, or documentation from a substance use clinic. If you are currently in medication-assisted treatment, your prescribing physician’s records are the clearest documentation.
Step 2 — Tell your OUD treatment provider.
If you are currently on buprenorphine, methadone, or naltrexone — tell the provider managing that treatment before adding cannabis. Some methadone clinics in Pennsylvania have policies on cannabis use that you should understand. Your treatment provider needs to know what you are using for safety monitoring and to support you effectively.
Step 3 — Book a telehealth certification appointment.
Find a PA DOH-registered medical marijuana certifying physician and complete the evaluation from home. The appointment takes 10–15 minutes. Bring your OUD diagnosis documentation and medication list. The certifying physician submits your certification to the Pennsylvania Department of Health.
Step 4 — Register with the PA MMJ Program.
After certification, register at the PA Medical Marijuana Program Patient Registry at patientportal.mmapinc.com. You need your PA driver’s licence or state-issued ID and the $50 annual fee. Fee waivers are available for patients enrolled in Medicaid, PACE/PACENET, CHIP, SNAP, or WIC.
Step 5 — Visit a Pennsylvania dispensary.
Tell the pharmacist you have opioid use disorder and describe your specific goals — craving management, anxiety, sleep, or pain. Ask for CBD-dominant or balanced products. Start at the lowest available dose. Maintain transparency with your treatment team.
Other Qualifying Conditions
- Amyotrophic Lateral Sclerosis (ALS)
- Autism
- Cancer, including remission therapy
- Crohn’s Disease
- Damage to the nervous tissue of the central nervous system (brain-spinal cord) with objective neurological indication of intractable spasticity, and other associated neuropathies
- Epilepsy
- Glaucoma
- Positive status for Human Immunodeficiency Virus or Acquired Immune Deficiency Syndrome (HIV/AIDS)
- Huntington’s Disease
- Inflammatory Bowel Disease (IBD)
- Intractable Seizures
- Multiple Sclerosis
- Neuropathies
- Parkinson’s Disease
- Post-traumatic Stress Disorder (PTSD)
- Severe chronic or intractable pain of neuropathic origin or severe chronic or intractable pain
- Sickle Cell Anemia
- Neurodegenerative diseases (i.e., Alzheimer’s Disease)
- Terminal illness
- Dyskinetic and spastic movement disorders
- Anxiety Disorder
- Chronic Hepatitis C
- Tourettes
Frequently Asked Questions
Q: I am on Suboxone. Can I still get a PA MMJ card?
Q: I am at a methadone clinic. Will they know? Will it affect my treatment?
Q: Will cannabis help me stop using opioids entirely?
Q: My NA sponsor says I cannot use cannabis and stay in the programme. What do I do?
Q: I previously had OUD but I am now in long-term recovery. Do I still qualify?
Q: Does cannabis risk making my OUD worse — by trading one addiction for another?
Pennsylvania OUD and Recovery Support Resources
Pennsylvania Department of Health – Get Help Now — pa.gov/opioids Pennsylvania’s official resource page for OUD treatment, including the PA Get Help Now hotline: 1-800-662-HELP (4357), available 24/7, connecting callers with treatment resources across the state.
SAMHSA National Helpline — 1-800-662-4357 (free, confidential, 24/7) The Substance Abuse and Mental Health Services Administration’s free treatment referral service. Can help locate medication-assisted treatment providers in Pennsylvania.
SAMHSA Treatment Locator — findtreatment.gov Find buprenorphine providers, methadone clinics, and other OUD treatment resources in Pennsylvania by zip code.
Pennsylvania Recovery Organizations Alliance (PRO-A) — pro-a.org Pennsylvania’s statewide recovery community organisation, providing peer support, recovery coaching, and resources for people at every stage of recovery.
Narcotic Recovery Association of Greater New York – SMART Recovery — smartrecovery.org Evidence-based, non-12-step recovery support with Pennsylvania meetings and online options. SMART Recovery takes a harm-reduction-compatible approach and is more openly compatible with medication-assisted treatment and cannabis use.
NOTE: Naloxone (Narcan) is available without a prescription at any Pennsylvania pharmacy. If you or someone you know uses opioids, having naloxone on hand saves lives. It is free or low-cost under Pennsylvania’s standing order and does not require a doctor’s visit.
Recovery looks different for different people, and medicine increasingly recognises that. Pennsylvania’s decision to include opioid use disorder as a qualifying condition for medical marijuana reflects that reality — that a single pathway does not work for everyone, and that more tools, used wisely and under medical supervision, serve people better than fewer.
The evidence for CBD’s effect on opioid cravings is real. The evidence that cannabis does not interfere with buprenorphine treatment is encouraging. And the evidence that chronic pain — so often the thread that runs through OUD — responds to cannabis is meaningful.