Is anxiety a neurological disorder? It’s a question that sounds simple but the honest answer reveals something genuinely fascinating about how the brain works, and why the line between “neurological” and “psychiatric” is far blurrier than most people assume.
The short answer: Anxiety is not classified as a neurological disorder in the traditional sense. It is officially classified as a psychiatric or mental health condition. But that classification doesn’t tell the whole story. Decades of neuroscience research have shown that anxiety disorders involve real, measurable changes in brain structure, brain chemistry, and nervous system function. What happens during anxiety is deeply neurological, even if the official label isn’t.
Understanding this distinction matters, not just academically, but practically. It affects how you think about your condition, what kind of help you seek, and which treatment options are available to you.
The Difference Between Neurological and Psychiatric Disorders
To answer whether anxiety is neurological, we first need to understand what that word actually means in medicine.
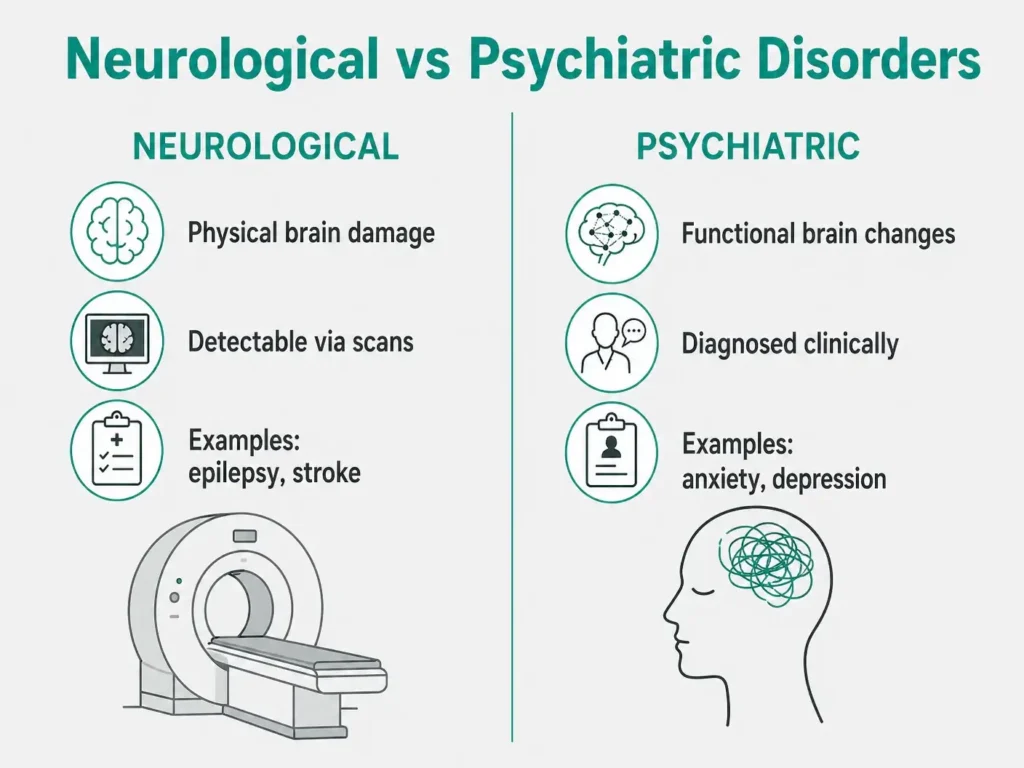
Neurological disorders: involve damage to or malfunction of the nervous system – the brain, spinal cord, and peripheral nerves. Classic examples include epilepsy (abnormal electrical activity in the brain), Parkinson’s disease (degeneration of dopamine-producing neurons), multiple sclerosis (damage to the myelin sheath of nerve cells), and stroke (disruption of blood flow causing brain tissue death). These conditions are detectable through physical examination, neurological testing, and brain imaging.
Psychiatric disorders: also called mental disorders — are traditionally defined by disturbances in thinking, emotion, and behavior that cause significant distress or functional impairment. They include conditions like schizophrenia, major depression, bipolar disorder, and anxiety disorders. The diagnosis is made through clinical interview and standardized criteria, not through a blood test or brain scan.
The British Journal of Psychiatry published a landmark study examining this distinction empirically and found that while neurological and psychiatric conditions do show different patterns of brain abnormalities, the boundary between them is far from clean. As the researchers concluded: “Psychiatric disorders are not just ‘mental’ but physical too.”
The traditional rule is: If a disorder is reliably associated with a recognizable pathological process in the central nervous system, it’s neurological. By that rule, anxiety is psychiatric because it doesn’t arise from a single, identifiable physical lesion or clearly visible structural damage.
But here’s where it gets interesting.
So Where Does Anxiety Actually Fall?
Anxiety is officially classified as a psychiatric/mental health condition under both the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition) and the ICD-11 (International Classification of Diseases), which groups anxiety under “anxiety and fear-related disorders.”
However, decades of neuroscience research have revealed that anxiety disorders involve:
- Measurable structural differences in the brain – including larger amygdala volume and altered white matter connectivity
- Functional differences visible on fMRI and PET scans – particularly in how the amygdala, prefrontal cortex, and hippocampus communicate
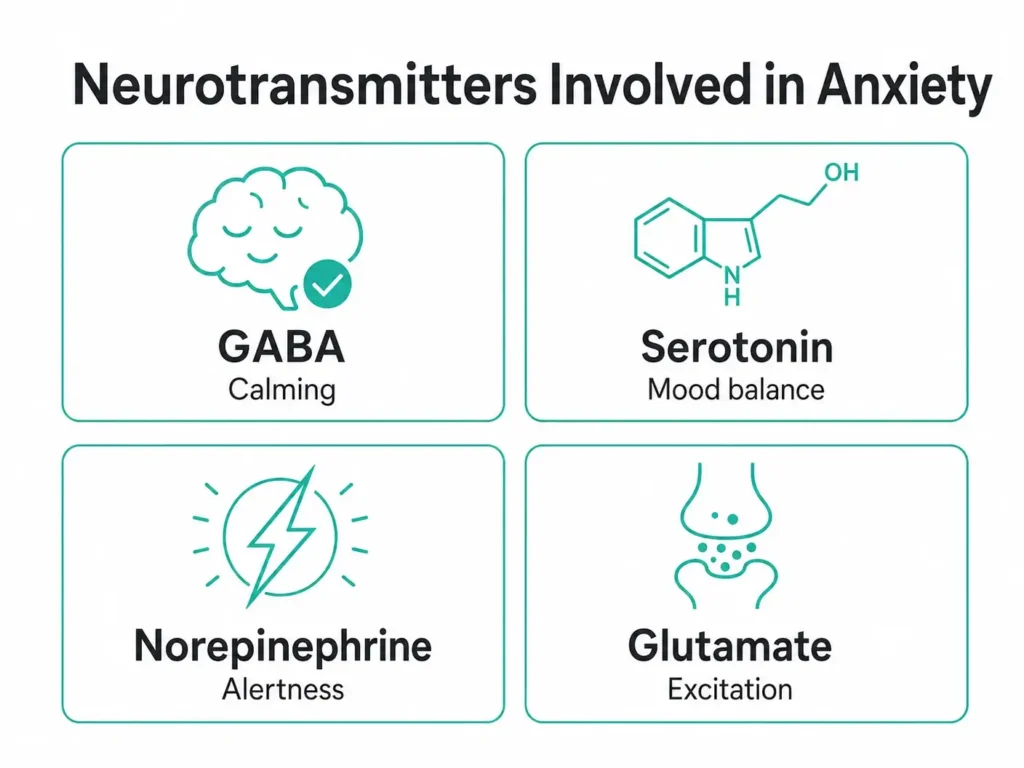
- Dysregulation of specific neurotransmitter systems – GABA, serotonin, norepinephrine, and glutamate
- Disruption of the autonomic nervous system – producing physical symptoms from racing heart to digestive problems
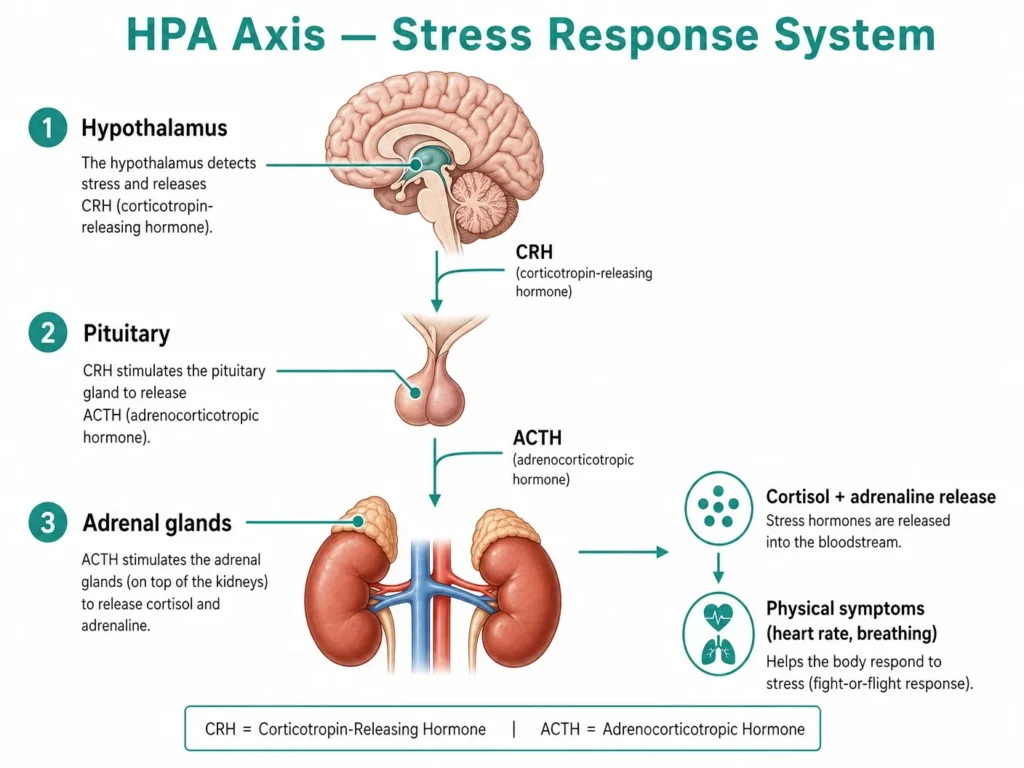
- Activation of the HPA (hypothalamic-pituitary-adrenal) axis – the brain-body stress response system
A 2025 review published in Nature Reviews Neuroscience noted that “recent advances in functional neuroimaging have provided new insights into the neural circuits implicated in pathological anxiety, revealing dysfunctions that cut across traditional diagnostic boundaries.”
In other words: Anxiety is categorized as psychiatric but it is neurobiological through and through. The brain changes are real. The nervous system involvement is real. The “mental” label is increasingly understood as a limitation of how medicine has historically divided itself, not a reflection of where the biology actually sits.
According to NIMH, an estimated 19.1% of U.S. adults roughly 1 in 5 had an anxiety disorder in the past year. Across a lifetime, 31.1% of adults will experience an anxiety disorder at some point. These numbers represent tens of millions of people whose brains are doing something measurably different, which is why this question matters far beyond semantics.
What Is Happening in Your Brain During Anxiety? In Plain English
Imagine your brain as a very sophisticated alarm system. It was designed to protect you, to scan your environment constantly for threats and trigger a rapid response when it detects danger.
That alarm system works beautifully when the threat is real, a car swerving toward you, a confrontation, a physical danger. Your brain fires, your body mobilizes, you respond. The threat passes. The alarm resets.
In anxiety disorders, something goes wrong with the alarm. The threat-detection system becomes oversensitive, it fires too easily, too intensely, or refuses to reset even when the danger has passed. The physical and psychological experience of anxiety – racing heart, shallow breathing, muscle tension, intrusive worry – is the result of a brain stuck in alarm mode.
This isn’t a metaphor. This is literally what is happening in your nervous system, and neuroscience has mapped it in remarkable detail. The brain structures involved, the chemicals triggering the alarm, and the feedback loops that keep it going are all measurable biological processes.
The Key Brain Structures Involved in Anxiety
Several specific brain regions play central roles in anxiety. Understanding them helps explain why anxiety feels so physical and why it can be so difficult to simply “think your way out of it.”
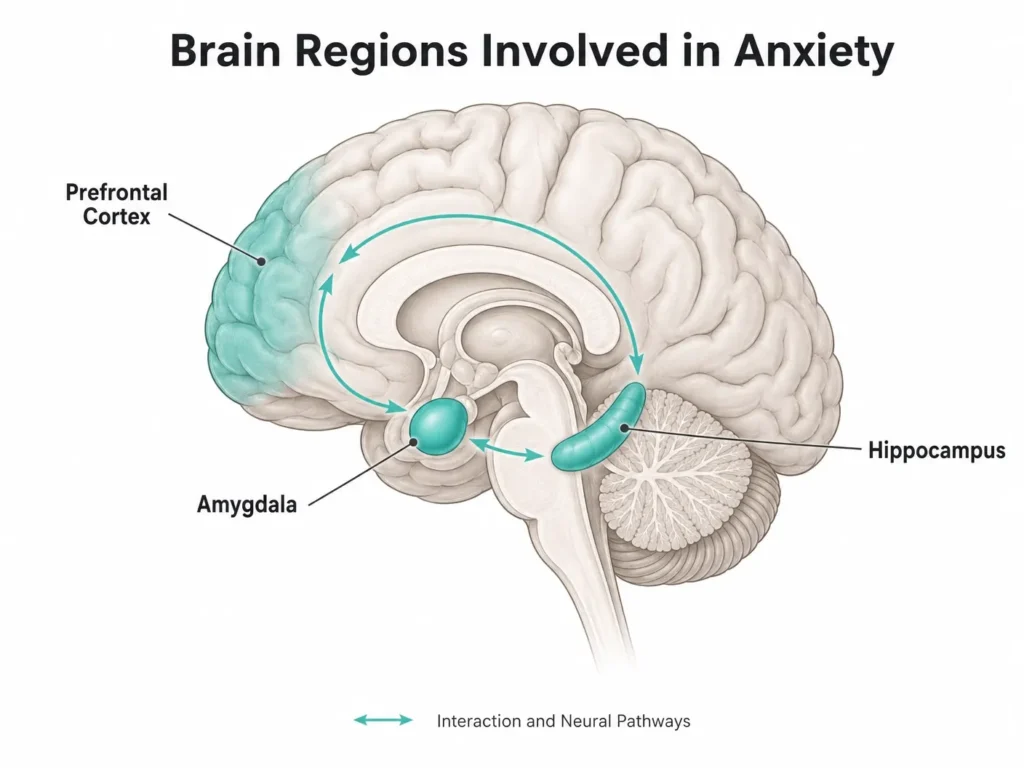
The Amygdala: The Brain’s Alarm Bell
The amygdala is a small, almond-shaped structure deep in the brain that acts as the threat detection and emotional processing center. When your brain perceives danger — real or imagined — the amygdala fires first, triggering the fight-or-flight response before your conscious mind has even registered what’s happening.
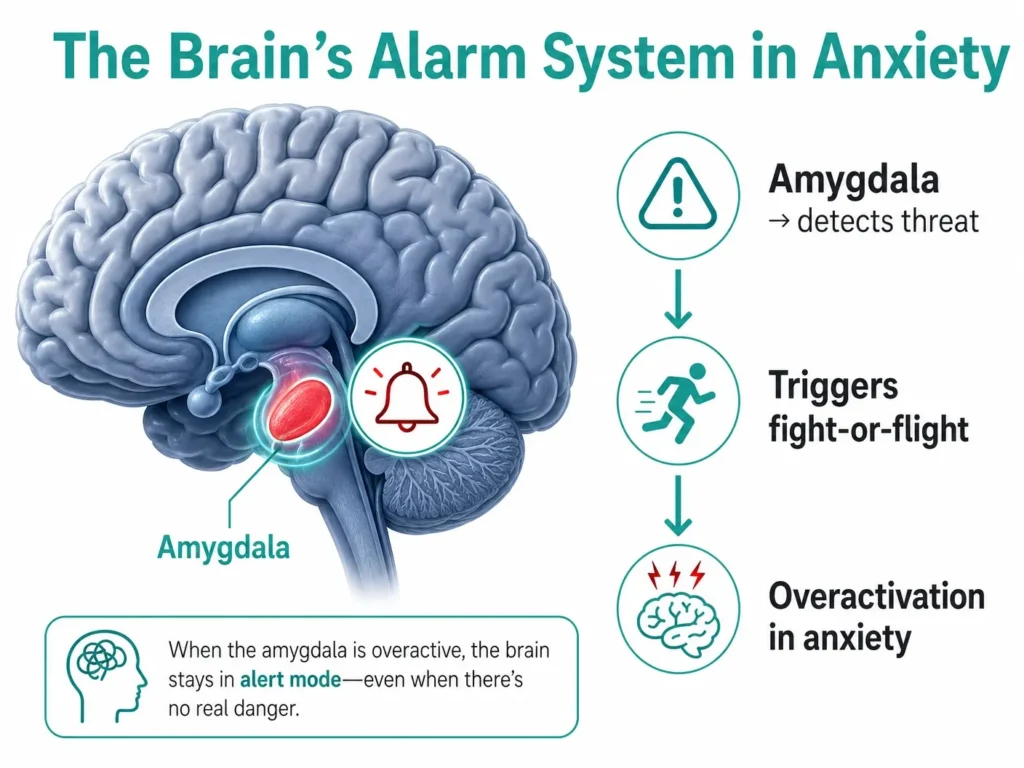
In people with anxiety disorders, research shows the amygdala is hyperreactive — it fires more readily, more intensely, and in response to stimuli that most people’s brains filter out. Studies cited in PMC have found that pediatric patients with GAD show increased amygdala volume — consistent with stress-induced amygdalar changes observed in animal studies.
The Prefrontal Cortex: The Rational Brake
The prefrontal cortex (PFC) is the brain’s executive control center — responsible for rational thinking, decision-making, and regulating emotional responses. In a healthy brain, the PFC acts as a brake on the amygdala’s alarm signals, evaluating whether the threat is real and dialing down the response when it isn’t.
In anxiety disorders, this brake system is impaired. The PFC’s regulatory influence over the amygdala is weakened, allowing the alarm to keep firing even when no real threat exists. This is why logic and reassurance often don’t reduce anxiety in the moment — the rational brain is losing the argument with the emotional brain.
The Hippocampus: Context and Memory
The hippocampus plays a critical role in memory formation and contextual learning. It helps the brain understand when and where a threat is relevant — distinguishing between a dangerous situation and a safe one.
In anxiety disorders, hippocampal function is disrupted. The brain struggles to properly contextualize threats — it may treat a crowded grocery store as dangerous because it resembles a past anxiety-triggering experience, even when objectively safe. Chronic stress and anxiety can also physically reduce hippocampal volume over time, according to research in Frontiers in Neural Circuits.
The Hypothalamus and the HPA Axis
The hypothalamus coordinates the body’s stress response through the HPA axis — triggering the release of cortisol and adrenaline that produce anxiety’s physical symptoms. We’ll cover this in detail in Section 7.
The Neurotransmitters Driving Anxiety
Neurotransmitters are the chemical messengers your brain uses to communicate between neurons. In anxiety disorders, several key neurotransmitter systems are out of balance. This is why medications that target specific neurotransmitters are effective treatments.
GABA: The Brain’s Natural Tranquilizer
GABA (gamma-aminobutyric acid) is the brain’s primary inhibitory neurotransmitter — it slows down neural activity, reduces excitability, and promotes calm. According to ScienceDirect, anxiety disorders are strongly associated with dysfunction in the GABAergic system.
When GABA signaling is insufficient, neurons fire more than they should — producing the heightened alertness, racing thoughts, and physical tension characteristic of anxiety. This is why benzodiazepines (Xanax, Klonopin) work for acute anxiety: they enhance GABA’s effects, essentially turning down the neural noise.
Serotonin: The Mood Stabilizer
Serotonin plays a central role in mood regulation, emotional processing, and the modulation of anxiety. Dysregulation of the serotonergic system is consistently associated with anxiety disorders. This is why SSRIs (Selective Serotonin Reuptake Inhibitors), medications like Zoloft, Lexapro, and Prozac are the most prescribed first-line treatment for anxiety. By increasing serotonin availability, they help stabilize mood and reduce anxiety over time.
Genetic variations in serotonin-related genes, including the serotonin transporter gene (SLC6A4), have been linked to increased susceptibility to anxiety disorders, as noted in the Neurobiology of Anxiety Disorders review.
Norepinephrine: The Arousal Chemical
Norepinephrine (also called noradrenaline) is the chemical that drives the fight-or-flight response — accelerating heart rate, redirecting blood flow, and heightening alertness. In anxiety disorders, norepinephrine signaling is dysregulated, keeping the body in a state of heightened arousal even when no threat is present. This explains anxiety’s physical symptoms: the racing heart, the sweating, the tension.
Glutamate: The Excitatory Accelerator
Glutamate is the brain’s primary excitatory neurotransmitter. Excessive glutamate activity — combined with insufficient GABA to balance it — creates the neural hyperactivity that underlies anxiety. Research in PMC notes that “increased activity in emotion-processing brain regions in patients with anxiety disorders could result from decreased inhibitory signaling by GABA or increased excitatory neurotransmission by glutamate.”
What Brain Imaging Shows About Anxiety
One of the most compelling pieces of evidence for anxiety’s neurological basis is what happens when you put anxious brains in a scanner.
Functional MRI (fMRI) and PET scans have consistently shown distinct patterns of brain activity in people with anxiety disorders compared to people without:
- Heightened amygdala activation in response to emotional stimuli – even neutral or mildly negative images trigger stronger amygdala responses in anxious brains
- Reduced prefrontal-amygdala connectivity – the communication pathway between the rational brain and the emotional alarm system is less effective
- Abnormal resting-state activity – anxious brains show different patterns even at rest, not just during active stress
- Altered white matter – the structural connections between brain regions show measurable differences in people with social anxiety disorder, as confirmed by a 2024 systematic review cited in Nature Reviews Neuroscience
These are not subjective reports. These are measurable biological differences visible on brain scans. The University of Rochester found that anxiety signals persist in the brain even in objectively safe environments — the brain maintains its threat alert long after the stressor has passed.
This is why telling someone with anxiety to “just relax” or “stop worrying” is about as useful as telling someone with a broken leg to “just walk normally.” The brain biology driving anxiety is not fully under conscious control.
The HPA Axis: How Anxiety Hijacks Your Whole Body?
This is where the “neurological” nature of anxiety becomes impossible to ignore: anxiety doesn’t stay in your brain. It recruits your entire body.
The HPA axis (hypothalamic-pituitary-adrenal axis) is the brain-body stress response system. When the amygdala detects a threat, it signals the hypothalamus, which activates the pituitary gland, which triggers the adrenal glands to release cortisol and adrenaline (epinephrine).
These hormones produce every physical symptom you associate with anxiety:
- Accelerated heart rate
- Rapid, shallow breathing
- Muscle tension
- Digestive disruption (the gut has its own nervous system — the enteric nervous system — that responds directly to stress hormones)
- Sweating and trembling
- Heightened sensory alertness
- Suppressed immune and digestive function (the body diverts resources to muscles and heart for “fight or flight”)
In people with anxiety disorders, the HPA axis is chronically over-activated — or fails to properly deactivate after a stress response. The result is a body stuck in a low-level stress state, with elevated cortisol affecting everything from sleep quality to cardiovascular health to immune function.
Research published in Brain Sciences notes that anxiety disorders — including GAD, panic disorder, and PTSD — affect approximately 14–18% of the overall population and produce significant physical health consequences through exactly this mechanism.
The Endocannabinoid System and Anxiety
This section is relevant to understanding why certain treatments work, including some that may surprise you.
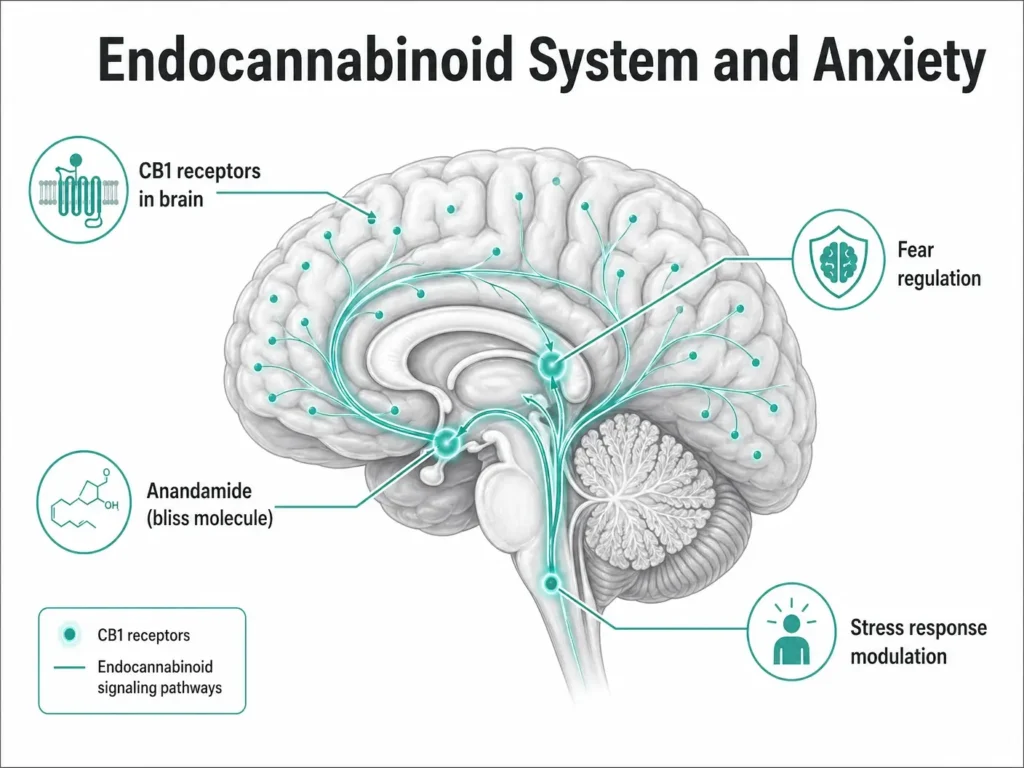
The body has its own endocannabinoid system (ECS), a network of receptors distributed throughout the brain and body that plays a key role in regulating mood, stress responses, fear, and anxiety. The ECS helps the brain learn to suppress fear responses after a threat has passed — a process called fear extinction.
Research cited in IntechOpen confirms that endocannabinoids: including anandamide (sometimes called the “bliss molecule”) are among the neurotransmitters and modulators known to be involved in anxiety regulation in the amygdala.
When the ECS is dysregulated, fear extinction becomes impaired, the brain struggles to “turn off” the anxiety response after the threat is gone. This is one neurological pathway through which cannabis compounds (particularly CBD, and to a more complex degree THC) interact with anxiety. Cannabinoids bind to ECS receptors and modulate the same anxiety-related circuits that are dysregulated in anxiety disorders.
This is not speculation, it is the neurobiological reason that Pennsylvania and 37 other states have recognized anxiety disorders as qualifying conditions for medical marijuana programs.
Does the Classification Matter for Treatment?
Here is the practical question most people reading this actually care about: does it matter whether anxiety is called neurological or psychiatric?
For most patients, the classification affects three things:
1. Which specialist you see: Neurologists treat structural and electrical nervous system conditions. Psychiatrists and psychologists treat anxiety disorders. However, because the brain biology of anxiety is increasingly well-understood, some neurologists do treat anxiety — particularly when it co-occurs with neurological conditions like epilepsy, TBI, or migraine.
2. How your condition is understood and stigmatized: One of the most important implications of understanding anxiety’s neurological basis is destigmatization. When people understand that anxiety is not a character flaw or a failure of willpower but a brain system that is functioning differently, it changes how they seek help and how they talk about their experience. The biology is real. The condition is real.
3. Which treatments make sense: Because anxiety involves specific neurotransmitter systems and brain circuits, treatments that target those systems work. That is why:
- SSRIs and SNRIs work – they restore serotonin balance
- Benzodiazepines work acutely – they enhance GABA signaling
- Beta-blockers work for performance anxiety – they block norepinephrine’s physical effects
- CBT works – it literally rewires prefrontal-amygdala connectivity through repeated practice
- Exercise works – it increases GABA, serotonin, and BDNF (a protein that supports neuronal health)
- Mindfulness works – it strengthens prefrontal regulation of the amygdala
The treatment list is long because anxiety touches so many neurological systems, which is also why treatment is personal and often requires some trial and error.
What This Means for Pennsylvania Residents With Anxiety
Understanding that anxiety has a genuine neurological basis, real brain changes, real neurotransmitter dysregulation, real nervous system involvement — is also part of why Pennsylvania took the step of formally recognizing anxiety disorders as a qualifying condition for a medical marijuana card.
Since July 2019, the Pennsylvania Department of Health has included anxiety disorders among its 24 approved qualifying conditions. This decision was grounded in the same science covered in this article. The recognition that anxiety involves the endocannabinoid system, and that cannabis compounds interact with the neurological pathways underlying anxiety.
According to Spotlight PA’s analysis of over 1.1 million certification records, anxiety disorders appear in approximately 60% of all Pennsylvania MMJ certifications — making it the most common qualifying condition in the state by a significant margin. A patient survey published in Frontiers in Neuroscience found that medical marijuana patients rated cannabis an average of 8.03 out of 10 for managing anxiety symptoms.
This doesn’t mean medical cannabis is right for everyone with anxiety. Like all treatments, it works through specific biological mechanisms — primarily the endocannabinoid system — and is most effective as part of a broader treatment plan. Products lower in THC and higher in CBD are generally better tolerated for anxiety, and starting with low doses under medical guidance is always recommended.
If you have a diagnosed anxiety disorder and live in Pennsylvania, you may qualify for a medical marijuana card. You can learn more on our Anxiety Disorder & Medical Marijuana in Pennsylvania page or review all PA qualifying conditions here.
Frequently Asked Questions
Q: Is anxiety a neurological disorder or a mental disorder?
A: Anxiety is officially classified as a psychiatric (mental health) disorder under both the DSM-5 and ICD-11. However, it has a strong neurological basis — involving measurable changes in brain structure, neurotransmitter function, and nervous system activity. The distinction between “neurological” and “psychiatric” is increasingly seen as a historical artifact rather than a clear biological boundary.
Q: What part of the brain causes anxiety?
A: Multiple brain structures are involved. The amygdala is the primary threat-detection center and is hyperreactive in people with anxiety disorders. The prefrontal cortex normally regulates the amygdala’s alarm signals but is less effective in anxious brains. The hippocampus influences how context is processed and can shrink with chronic anxiety. The hypothalamus coordinates the physical stress response through the HPA axis.
Q: Is anxiety caused by a chemical imbalance?
A: Partially — but “chemical imbalance” is an oversimplification. Anxiety involves dysregulation of multiple neurotransmitter systems, including GABA (the brain’s natural calming signal), serotonin (mood regulation), norepinephrine (arousal and fight-or-flight), and glutamate (excitatory signaling). It also involves structural and functional differences in brain circuits, not just chemistry.
Q: Can anxiety cause neurological symptoms?
A: Yes. Because anxiety activates the nervous system — including the autonomic nervous system and HPA axis — it produces genuinely neurological symptoms: muscle tension, trembling, dizziness, tingling or numbness, heart palpitations, difficulty concentrating, and digestive disruption. These are real physiological events, not “just in your head.”
Q: Do you see a neurologist or psychiatrist for anxiety?
A: Anxiety disorders are typically treated by psychiatrists, psychologists, or primary care physicians — not neurologists. However, if anxiety co-occurs with a neurological condition (epilepsy, TBI, migraine), a neurologist may be part of your care team. For anxiety alone, a psychiatrist handles medication management and a psychologist or therapist handles CBT and other psychological treatments.
Q: Does understanding the neuroscience of anxiety change how it’s treated?
A: Yes, significantly. Understanding which brain circuits and neurotransmitters are involved explains why specific treatments work — SSRIs restore serotonin balance, CBT rewires prefrontal-amygdala connectivity, benzodiazepines enhance GABA signaling. It also opens the door to newer research-backed approaches, including treatments targeting the endocannabinoid system.
Q: Can Pennsylvania residents with anxiety get a medical marijuana card?
A: Yes. Pennsylvania recognizes anxiety disorders as a qualifying condition for a medical marijuana card. The neurobiological basis of anxiety — specifically its involvement of the endocannabinoid system — is part of the scientific rationale behind this recognition. If you have a clinical diagnosis of an anxiety disorder, you may qualify.
The Bottom Line
Is anxiety a neurological disorder? Officially, no — it’s classified as a psychiatric condition. But the neuroscience tells a richer story. Anxiety involves real, measurable changes in brain structure, brain chemistry, and nervous system function. The amygdala fires too readily. The prefrontal brake fails to hold. Neurotransmitter systems fall out of balance. The HPA axis floods the body with stress hormones. The endocannabinoid system loses its ability to quiet the alarm.
This is biology. It is not weakness. It is not a character flaw. And understanding it as a brain-based condition — not simply a “mental” one — is both scientifically accurate and genuinely helpful for the tens of millions of people who live with it.
If you’re a Pennsylvania resident with a diagnosed anxiety disorder and you’re curious about all your treatment options — including medical cannabis — our team is here to help.
Medically reviewed by Dr. Johnathon Chance Miller, MD. This article is for informational and educational purposes only and does not constitute medical advice. For diagnosis and treatment of anxiety disorders, consult a licensed healthcare provider.
Sources:
- NIMH — Any Anxiety Disorder Statistics
- NIMH — Generalized Anxiety Disorder Statistics
- Nature Reviews Neuroscience — Neural Circuit Basis of Pathological Anxiety (2025)
- PMC — Neurobiology of Anxiety Disorders: Brain Imaging, Genetics, and Psychoneuroendocrinology
- PMC — Are Neurological and Psychiatric Disorders Different? British Journal of Psychiatry
- ScienceDirect — Neural Basis of Anxiety
- Open Access Journals — Neurobiology of Anxiety Disorders (2024)
- IntechOpen — The Amygdala and Anxiety
- Brain Sciences — The Anxious Brain (2024)
- Frontiers in Neural Circuits — Neural Circuits Mechanisms of Anxiety (2025)
- ADAA — Anxiety Facts & Statistics
- Spotlight PA — PA MMJ Certifications Analysis
- Frontiers in Neuroscience — Cannabis & Anxiety Patient Study