If you have ever walked into a Pennsylvania dispensary — or searched for sleep advice online — someone has probably told you the same thing: indica is for sleep, sativa is for daytime. It is clean, simple, and easy to remember.
It is also incomplete.
The indica versus sativa distinction, while useful as a rough starting point, tells you far less about what will actually happen when you try to sleep than most dispensary budtenders let on. The research is clear on this — and understanding what actually drives cannabis’s sleep effects will save you from spending money on products that do not work, or worse, ones that keep you wired at midnight wondering what went wrong.
Here is what the science says, what it means practically, and what Pennsylvania patients specifically need to know.
The Indica vs. Sativa Question — and Why It’s More Complicated Than You Think
The conventional wisdom goes like this: indica strains produce a heavy, relaxing body high — “in-da-couch” — while sativa strains are energizing and cerebral. Choose indica for sleep, sativa for creativity and focus.
This framework is not entirely wrong. But it is far less reliable than most people assume.

Ethan Russo, MD — a board-certified neurologist and one of the most cited cannabis researchers in the world — addressed the indica/sativa distinction directly in the journal Cannabis and Cannabinoid Research, describing it as “total nonsense and an exercise in futility.” His argument is straightforward: decades of crossbreeding have made nearly every commercially available strain a hybrid. The genetic lineage of a plant labeled “indica” or “sativa” at a dispensary has little to no predictive value for the compounds that actually drive its pharmacological effects.
A study analyzing the German medical cannabis market confirmed this empirically — researchers found that terpene profiles across sativa, indica, and hybrid strain categories are “quite heterogenous,” with no meaningful relationship between the category label and the compounds that determine how the plant actually affects the body.
What this means practically: a product labeled “indica” with a low myrcene content and high limonene content may actually keep you awake. A product labeled “sativa” rich in myrcene and linalool may put you to sleep. The label is a starting point, not a guarantee.
The real question is not indica or sativa. It is: what is in this specific product?
What Actually Determines Whether Cannabis Makes You Sleepy
Two categories of compounds are responsible for cannabis’s sedative effects:
Terpenes — the aromatic compounds that give cannabis its distinct smell. Different terpenes interact with the nervous system in meaningfully different ways. Some are sedating. Some are stimulating. The ratio and concentration of terpenes in a specific product is a far more reliable predictor of sleepiness than the indica/sativa label.
Cannabinoids — THC, CBD, CBN, and others. Each interacts with the endocannabinoid system differently, and their specific effects on sleep architecture vary considerably depending on dose, ratio, and individual physiology.
Understanding both — and knowing how to read them on a Certificate of Analysis (COA) from a licensed Pennsylvania dispensary — gives you an enormous advantage over simply guessing based on a strain category label.
The Key Terpenes for Sleep — and What to Look for on a Lab Report
Licensed Pennsylvania dispensaries are required to provide lab testing data for all products. When shopping for a sleep-oriented cannabis product, these are the terpenes to look for on that report.

Myrcene
Myrcene is the most abundant terpene in most cannabis cultivars, and it is the primary driver of what people describe as the classic “indica” body effect.
The research on myrcene’s sedative properties is among the strongest available for any cannabis terpene. A study published in Pharmaceuticals found that beta-myrcene exerts sedative-hypnotic effects via the serotonergic synaptic pathway — reducing sleep latency, increasing sleep duration, and increasing the rate of falling asleep in insomnia mouse models. A separate study found that myrcene increased barbiturate-induced sleep time by a factor of 2.6 at a dose of 200mg/kg, alongside muscle-relaxant properties that may help with physical tension that prevents sleep onset.
What to look for: Myrcene above 0.5% total terpene content is generally associated with more pronounced sedative effects. Products with myrcene above 1% will typically produce the heaviest relaxation response.
Linalool
Linalool is the primary terpene in lavender — which is why certain cannabis products produce that floral, calming scent. Its sleep-relevant mechanism is distinct from myrcene’s: linalool enhances GABA receptor function and modulates glutamate activity, creating neurological conditions conducive to deeper relaxation.
Research has shown that linalool’s anxiolytic effects at relevant doses may be comparable to certain prescription sedatives — making it particularly relevant for people whose sleep problems are driven by anxiety or racing thoughts at bedtime.
What to look for: Linalool above 0.2% in a product’s terpene profile. Most effective when combined with myrcene rather than in isolation.
Beta-Caryophyllene
Beta-caryophyllene (BCP) is the only terpene known to directly activate CB2 receptors — giving it a cannabinoid-like action on top of its terpene properties. It carries peppery, spicy notes and has demonstrated pain-relieving and anti-inflammatory effects in preclinical research.
For sleep specifically, BCP addresses the physical discomfort and pain that frequently disrupts sleep — particularly relevant for patients whose sleep problems are linked to chronic pain conditions. It also has an anti-anxiety component through CB2 pathway modulation.
What to look for: BCP above 0.3% is associated with physical comfort and mild anxiolysis. Particularly useful when pain is a contributing factor to poor sleep.
What to Avoid for Sleep: Limonene and Terpinolene
Limonene produces citrus-forward aromas and tends toward energizing, mood-elevating effects. Terpinolene similarly trends stimulating at lower doses. Products heavily weighted toward these terpenes — regardless of whether they are labeled indica or sativa — are less likely to support sleep onset and may actively work against it.
THC and Sleep: Benefits, Risks, and What the Research Actually Shows
THC is the most studied cannabinoid for sleep — and the research tells a nuanced story that most cannabis content glosses over.
The short-term benefit: THC activates CB1 receptors in brain regions that regulate sleep, including areas controlling cholinergic neurons involved in sleep initiation. In the short term, THC has been shown to reduce sleep onset latency — the time it takes to fall asleep. One controlled trial found THC specifically reduced the time to sleep onset compared to placebo.
The long-term concern: At higher doses, and with prolonged use, THC has been associated with suppression of REM sleep — the dream stage of sleep critical for memory consolidation, emotional processing, and cognitive function. A 2025 systematic review and meta-analysis published in ScienceDirect found that while recent therapeutic-dose studies show mixed results on REM suppression, withdrawal from regular cannabis use was consistently associated with REM rebound, reduced total sleep time, and increased sleep onset latency.
This means using high-THC products every night to sleep carries a real risk: over time, the body may become reliant on THC to initiate sleep, and stopping — even briefly — can cause temporarily worse sleep than before. This is not a reason to avoid THC for sleep, but it is a reason to use it thoughtfully, at the lowest effective dose, and not as an every-night permanent solution.
Dosing matters significantly. Research suggests that low-to-moderate THC doses (roughly 5–10mg for most adults) may reduce sleep latency with less impact on sleep architecture than higher doses. Starting low and adjusting gradually is the most responsible approach.
CBD and Sleep: A Different — and Often Better — Role
CBD’s relationship with sleep is dose-dependent in an interesting and counterintuitive way.
At lower doses, CBD tends to be mildly alerting — it may actually reduce drowsiness and support daytime wakefulness. At higher doses, CBD shifts toward a sleep-supportive role. Research published in PMC found that CBD had a positive effect on anxiety-related REM sleep suppression, and that there is a dose-dependent effect on REM sleep latency.
CBD’s most consistent sleep benefit comes through its anxiolytic properties. By reducing pre-sleep anxiety — the racing thoughts and physical tension that keep many people awake — CBD can improve sleep quality indirectly, without the psychoactive effects of THC and with a lower risk of dependence or sleep architecture disruption.
A double-blind, placebo-controlled randomized crossover study published in medRxiv found that a CBD and terpene formulation — including linalool, myrcene, and beta-caryophyllene — produced significant gains in restorative sleep in insomnia patients compared to placebo, with participants averaging 48 additional minutes of rest compared to CBD alone in the terpene-combined condition.
The practical implication: For people whose sleep problems are primarily anxiety-driven — lying awake with a busy mind — a higher-CBD, lower-THC product with sedating terpenes may be more effective than a high-THC indica, and carries significantly less risk of dependence or sleep quality degradation over time.
CBN: The “Sleep Cannabinoid” Worth Knowing About

CBN (cannabinol) is a minor cannabinoid produced when THC oxidizes — essentially, aged or degraded THC. It has developed a strong reputation as a sleep aid, and you will find it prominently marketed in dispensary sleep products.
The honest assessment: CBN’s sleep reputation is based largely on extrapolation and anecdote rather than robust clinical evidence specifically for CBN in isolation. Most of the sedative reputation attributed to CBN historically came from studies on cannabis that also contained THC, myrcene, and other sedating compounds — making it difficult to isolate CBN’s independent contribution.
That said, anecdotal evidence from patients is consistent enough that it warrants attention, and preliminary research suggests CBN may have mild sedative properties. Products combining CBN with THC, CBD, myrcene, and linalool are among the most commonly reported effective sleep formulations by cannabis users.
PA dispensaries carry a range of CBN-containing products — tinctures, capsules, and vaporizer cartridges — that are worth discussing with a dispensary pharmacist if sleep is your primary goal.
The Long-Term Risk Nobody Talks About
Most cannabis sleep content either oversells cannabis as a sleep cure or is so cautious it provides no useful guidance. The honest middle ground is this:
Cannabis — particularly THC — can be genuinely useful for sleep in the short term. But relying on it every night for months or years introduces real risks that deserve clear acknowledgment.
Regular, heavy cannabis use has been associated with altered sleep architecture — specifically reductions in slow-wave and REM sleep that overlap with symptoms of clinical insomnia. When chronic users stop, a “rebound” effect commonly occurs: vivid dreams return intensely (the brain catching up on suppressed REM), sleep onset becomes temporarily difficult, and total sleep time may decrease before normalizing.
A broad review of cannabis and sleep, published across decades of literature, found that while cannabis can improve sleep in some cases, it made sleep worse in others — with one analysis finding improvement in approximately 21% of studied cases and worsening in 48%.
This does not mean cannabis has no place in a sleep strategy. It means it works best as one component of a broader approach — alongside good sleep hygiene, consistent sleep timing, reduced blue light exposure before bed, and, when appropriate, cognitive behavioral therapy for insomnia (CBT-I), which remains the gold-standard treatment for chronic insomnia.
How to Actually Choose a Sleep Product at a PA Dispensary
Armed with the above, here is a practical framework for selecting a sleep-oriented cannabis product at a licensed Pennsylvania dispensary:
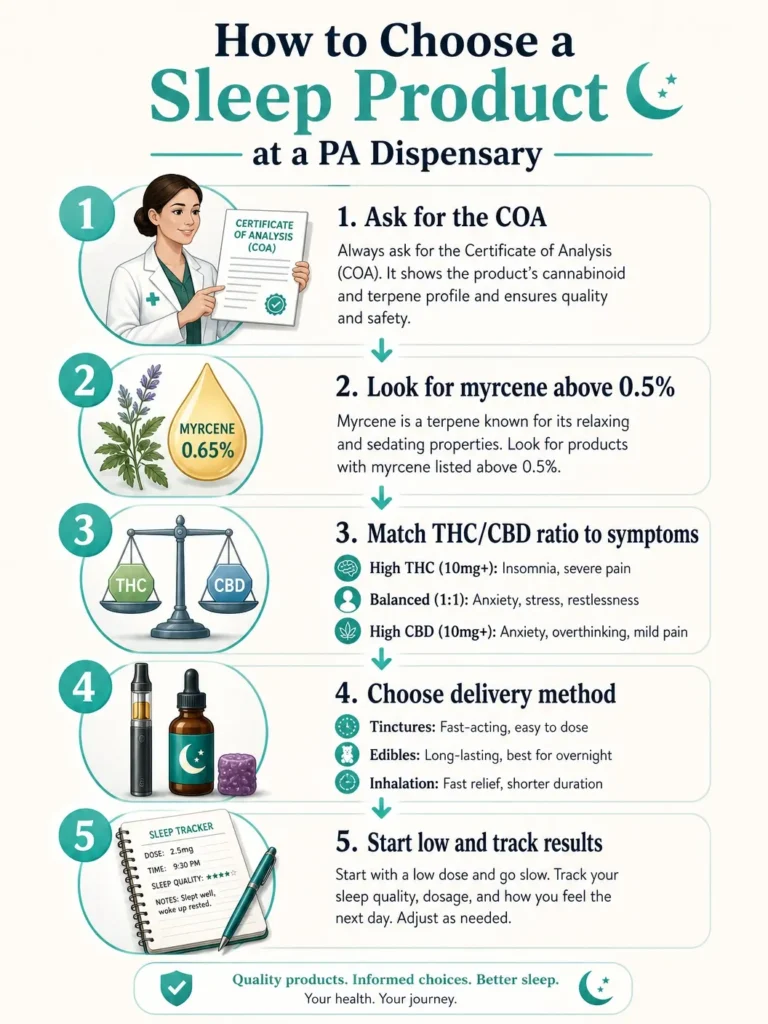
Step 1 — Ask for the Certificate of Analysis (COA). Every product at a PA dispensary has been third-party tested. The COA shows the actual cannabinoid and terpene content. This is far more reliable than the strain name or the indica/sativa label.
Step 2 — Look for myrcene above 0.5% as the lead terpene. If myrcene is not the dominant or co-dominant terpene, the product is less likely to produce the sedating body-heaviness associated with sleep. Linalool and beta-caryophyllene as secondary terpenes strengthen the sleep case.
Step 3 — Match your cannabinoid ratio to your sleep problem.
| Sleep Problem | Suggested Starting Ratio |
|---|---|
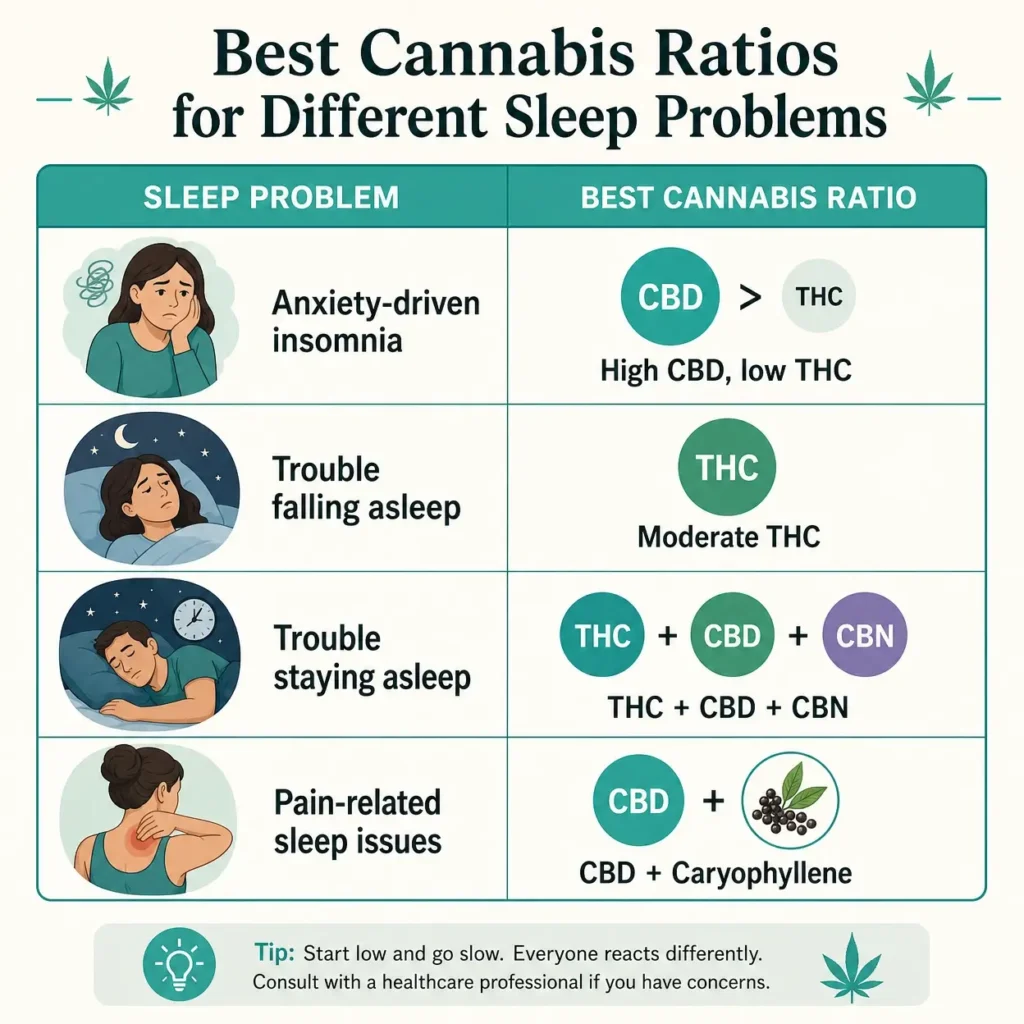
| Trouble falling asleep (anxiety-driven) | High CBD, low THC (10:1 or higher), sedating terpenes |
| Trouble falling asleep (no anxiety) | Moderate THC (5–10mg), myrcene-rich |
| Trouble staying asleep | Balanced THC:CBD with CBN addition, edible or tincture format for longer duration |
| Pain preventing sleep | CBD + BCP-rich product, consider adding low-dose THC |
| PTSD-related nightmares | THC has shown specific promise here — discuss dosing with dispensary pharmacist |
Step 4 — Consider delivery method for timing. Vaporization (legal in PA for MMJ patients) produces onset within minutes and effects lasting 2–3 hours — useful for falling asleep but may not last through the night. Oral products (tinctures, capsules, edibles) take 45–90 minutes to onset but last 4–8 hours — better suited for staying asleep through the night.
Note for PA patients: Pennsylvania medical marijuana law prohibits smoking. Combustion-based consumption is not a legal delivery method for PA MMJ cardholders. Vaporization, oral ingestion, tinctures, and other approved methods are the legal options.
Step 5 — Start low and track your results. Start at the lowest effective dose — especially with THC-containing products. Give a product at least a week of consistent use before evaluating whether it is working. Document how you feel falling asleep, how often you wake during the night, and how you feel in the morning. Adjust based on evidence, not assumption.
Pennsylvania-Specific Context: What You Need to Know
For Pennsylvania residents, there is important context that shapes this entire conversation.
Insomnia alone is not a PA qualifying condition.
This is something many people do not know. The Pennsylvania Medical Marijuana Advisory Board considered adding insomnia to the list of qualifying conditions and voted 7-4 against it. Board members noted that insomnia is often caused by an underlying medical condition and does not always rise to the level of a serious medical condition on its own.
But that is not the end of the story for most people with sleep problems.
A study of Pennsylvania MMJ patients, published in a peer-reviewed journal in 2022, found that 38.6% of PA MMJ patients reported sleep disturbance as a significant symptom — but qualified through other conditions: anxiety disorder (36.7%), chronic pain (48.6%), and PTSD (15.7%).
This matters because the conditions most commonly underlying chronic sleep problems in Pennsylvania — anxiety, chronic pain, PTSD — are three of the top qualifying conditions in the PA MMJ program. If your sleep problems are driven by anxiety that keeps your mind racing, by chronic pain that makes it impossible to get comfortable, or by PTSD-related nightmares, you very likely qualify for a PA medical marijuana card under one of those conditions — and cannabis access that may improve your sleep comes with it.
Pennsylvania-based research from PCOM, published in February 2026, followed 137 PA adults with poor sleep quality for a full year after medical cannabis initiation. Researchers found significant improvement in overall sleep quality within the first three months, and those improvements were sustained across the entire 12-month follow-up — making it one of the most encouraging PA-specific sleep and cannabis studies to date.
Who this is relevant for:
If you are a Pennsylvania resident who struggles with sleep and experiences anxiety, chronic pain, or PTSD — conditions that are causing the sleep disruption — you may already meet the criteria for PA medical marijuana certification. The process is done entirely through telehealth and does not require an in-person visit.
A full list of Pennsylvania’s 24 qualifying conditions is available here. If anxiety is your primary condition — as it is for approximately 60% of PA MMJ patients — you can learn more specifically about how anxiety qualifies here.
Cost breakdown for PA MMJ certification:
| Fee | Amount |
|---|---|
| Physician certification fee (new patient) | $159 |
| PA state registration fee | $50 |
| Total (new patient) | $209 |
| Physician certification fee (renewal) | $149 |
| PA state registration fee | $50 |
| Total (renewal) | $199 |
Patients who qualify for Medicaid, SNAP, WIC, CHIP, PACE, or PACENET may have the $50 state fee waived through Pennsylvania’s MMAP program.
Once certified, you can access lab-tested, accurately labeled cannabis products — including products specifically formulated for sleep — at over 186 licensed PA dispensaries statewide, with guidance from licensed dispensary pharmacists. That is a meaningfully different experience from guessing at a gas station or ordering unlabeled products online.
If you think you may qualify, you can start the process at Pennsylvania Marijuana Cards.
Frequently Asked Questions
Q: Is indica or sativa better for sleep?
A: Indica is generally the better starting point — but the label alone is not reliable. What actually determines whether a cannabis product supports sleep is its terpene and cannabinoid profile, not whether it is classified as indica or sativa. Specifically, products high in myrcene (above 0.5%), linalool, and beta-caryophyllene tend to produce the most sedating effects. A product’s Certificate of Analysis (COA) from a licensed dispensary gives you far more useful information than the strain category label. When in doubt, ask a dispensary pharmacist to help you identify products with sleep-supporting terpene profiles rather than simply picking an “indica.”
Q: Does THC or CBD help more with sleep?
A: It depends on why you are having trouble sleeping. THC reduces sleep onset latency — helping you fall asleep faster — but at higher doses and with long-term use it may suppress REM sleep and create dependence that worsens sleep when stopped. CBD is less likely to cause dependence and works better for anxiety-driven sleep problems, but is dose-dependent — lower doses can be alerting rather than sedating. For most people, a low-dose THC product with sedating terpenes (myrcene, linalool) works well for falling asleep, while CBD-dominant products with those same terpenes work better when anxiety is the primary barrier to sleep. CBN-containing products may add additional sleep support when combined with either.
Q: Can I get a Pennsylvania medical marijuana card for sleep problems?
A: Insomnia by itself is not a qualifying condition in Pennsylvania’s MMJ program — the Medical Marijuana Advisory Board voted against adding it as a standalone condition. However, if your sleep problems are caused by or significantly connected to anxiety disorder, chronic pain, or PTSD — three of Pennsylvania’s top qualifying conditions — you may well qualify for a PA medical marijuana card under one of those conditions. A 2026 Pennsylvania study found that sleep quality improved significantly and sustainably in PA MMJ patients certified for anxiety, pain, and PTSD. If you are unsure whether your underlying condition qualifies, a telehealth consultation with a licensed PA physician is the most reliable way to find out.
Medically reviewed by Dr. Johnathon Chance Miller, MD. This content is for educational purposes only and does not constitute medical advice. Cannabis affects individuals differently and is not a substitute for professional medical treatment of sleep disorders. Cognitive behavioral therapy for insomnia (CBT-I) remains the gold-standard first-line treatment for chronic insomnia. Pennsylvania medical marijuana patients should follow all state laws regarding legal methods of consumption — smoking cannabis is prohibited under PA law. Do not drive after consuming cannabis.
Sources
- Russo EB. “The Case for the Entourage Effect and Conventional Breeding of Clinical Cannabis: No ‘Strain,’ No Gain.” Cannabis and Cannabinoid Research, 2019.
- Hazekamp A. “The Trouble with CBD Oil.” Medical Cannabis and Cannabinoids, 2018. Referenced via ScienceInsights analysis of German cannabis market terpene study.
- Chen H, et al. “Beta-Myrcene as a Sedative–Hypnotic Component from Lavender Essential Oil in DL-4-Chlorophenylalanine-Induced-Insomnia Mice.” Pharmaceuticals, 2024.
- Terpene Belt Farms. “Best Terpenes for Sleep: Top Choices for Sleep Products.” November 2025.
- Twenty One Cannabis. “Best Terpenes for Sleep: Myrcene, Linalool & Caryophyllene Guide.” February 2026.
- PMC / National Library of Medicine. “The Neurotherapeutic Arsenal in Cannabis sativa: Insights into Anti-Neuroinflammatory and Neuroprotective Activity.”
- PMC. “The Effects of Cannabinoids on Sleep.”
- Vaillancourt R, et al. “Cannabis and sleep architecture: A systematic review and meta-analysis.” ScienceDirect, September 2025.
- PMC. “Are Sweet Dreams Made of These? Understanding the Relationship Between Sleep and Cannabis Use.”
- PMC. “Effects of Cannabinoids on Sleep and their Therapeutic Potential for Sleep Disorders.”
- medRxiv. “A Cannabidiol/Terpene Formulation Increases Restorative Sleep in Insomniacs: A Double-Blind, Placebo-controlled, Randomized, Crossover Study.” 2023.
- Sleep Doctor. “Does Marijuana Affect REM Sleep?” January 2024.
- PMC. “Are Sweet Dreams Made of These? Understanding the Relationship Between Sleep and Cannabis Use.”
- Sleep Foundation. “Cannabis for Sleep: Benefits and Risks.” September 2025.
- PMC. “Cannabinoids and Sleep: Exploring Biological Mechanisms and Therapeutic Potentials.”
- PhillyVoice. “Pennsylvania’s Medical Marijuana Advisory board denies insomnia as a qualifying condition.” November 2020.
- ScienceDirect. “Characterizing anxiety, pain, sleep, and quality of life among patients in a state Medical Marijuana Program.” 2022.
- PCOM. “Study Links Medical Cannabis Use to Lasting Improvements in Sleep.” February 2026.
- PhillyVoice. “Pennsylvania’s medical marijuana program has 24 qualifying conditions — anxiety is by far the most common.” July 2025.