Nausea is one of the oldest documented reasons people use cannabis medicinally — and one of the most scientifically validated ones. Two FDA-approved medications already on the market (dronabinol and nabilone) are synthetic cannabinoids prescribed specifically because the antiemetic evidence is strong enough to have cleared clinical approval.
But for patients using whole-plant cannabis through a Pennsylvania dispensary, the question becomes more specific: which strains, which terpenes, and which consumption methods actually work — and why?
This guide answers that question honestly. It covers the science of how cannabis reduces nausea, which terpenes matter most, what strains to look for at PA dispensaries, how to consume for fastest relief, and one critical warning that almost no guide mentions: a condition where cannabis causes nausea instead of treating it.
One important note upfront: Strain names in cannabis are inconsistent — two products labeled the same can have completely different chemical profiles depending on the grower. The practical advice throughout this guide focuses on terpene profiles and cannabinoid ratios, which you can verify through the Certificate of Analysis (COA) at any licensed PA dispensary, rather than strain names alone.
How Cannabis Reduces Nausea: The CB1 Receptor Mechanism
Before picking a strain, it helps to understand why cannabis works for nausea in the first place — because this determines which cannabinoids and terpenes are actually doing the work.
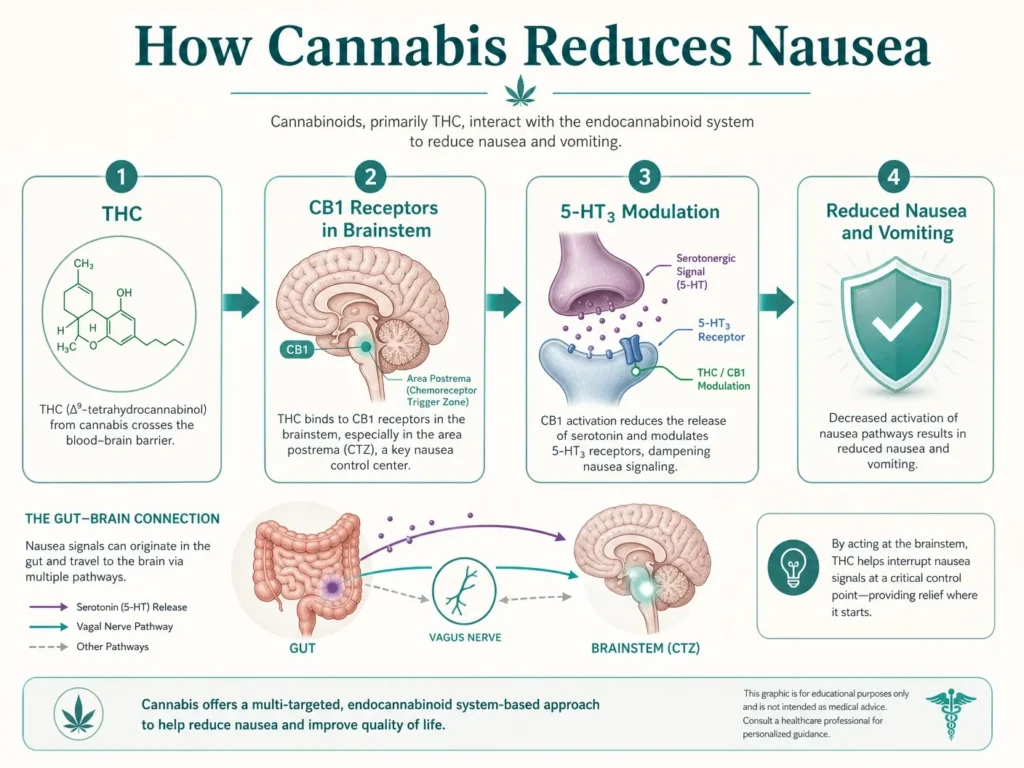
The body’s nausea and vomiting reflex is primarily controlled by a region of the brainstem called the dorsal vagal complex (DVC), which consists of the nucleus tractus solitarius (NTS), the area postrema (AP), and the dorsal motor nucleus of the vagus (DMNX). When emetic signals — from chemotherapy drugs, motion sickness, infection, or other triggers — reach the DVC, they stimulate the vomiting reflex.
CB1 cannabinoid receptors are densely concentrated in the DVC. When THC activates these receptors, it directly inhibits the neuronal activity that triggers nausea and vomiting. A landmark study published in the American Journal of Physiology demonstrated that THC applied directly to the brainstem surface was sufficient to inhibit emesis — confirming the antiemetic mechanism operates at the DVC level, not just peripherally.
A 2025 comprehensive review in Neurogastroenterology & Motility (PMC11872018) confirmed: cannabinoids also act on serotonin 5-HT3 receptors in the DVC — the same receptor pathway targeted by ondansetron (Zofran), one of the most commonly prescribed pharmaceutical antiemetics. This dual mechanism — CB1 activation plus 5-HT3 inhibition — helps explain why cannabis can work even when standard antiemetics have failed, particularly in chemotherapy patients.
The NCBI StatPearls review of cannabinoid antiemetic therapy notes that cannabinoids also act on presynaptic CB1 receptors to reduce serotonin release into the synapse — another layer of antiemetic action.
The practical takeaway: THC is the primary antiemetic cannabinoid. Strains with moderate-to-high THC content, combined with the right terpenes (detailed below), are most supported by the evidence for nausea relief.
The Terpenes That Matter Most for Nausea
THC does the heavy lifting — but specific terpenes amplify its antiemetic effects through complementary mechanisms. When you’re reading a COA at a PA dispensary, these are the terpenes to look for.
| Terpene | Mechanism for Nausea | Also Found In |
|---|---|---|
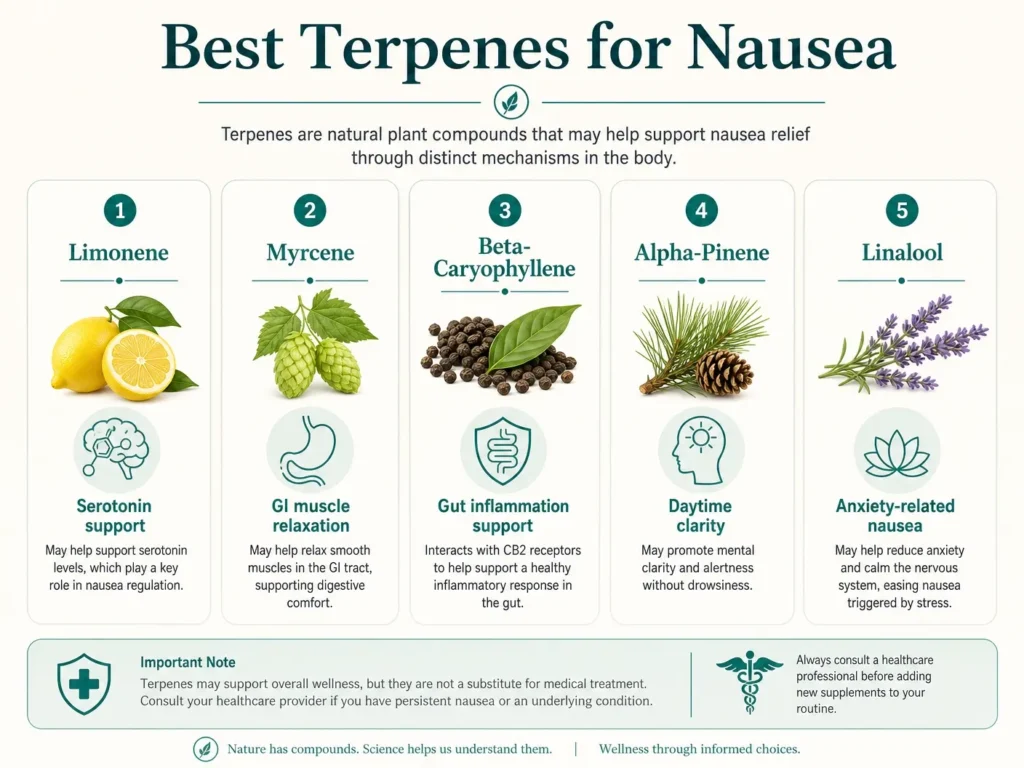
| Limonene | Modulates serotonin pathways in gut and brain; blocks nitric oxide (pro-inflammatory); reduces anxiety-driven nausea | Lemon peel, citrus fruits |
| Myrcene | Relaxes smooth muscle in GI tract; reduces inflammatory cytokines that trigger nausea; anti-inflammatory | Hops, mango, thyme |
| Beta-Caryophyllene | Activates CB2 receptors in GI tract; reduces gut inflammation and protects stomach lining | Black pepper, cloves |
| Alpha-Pinene | Interacts with CB1 receptors; reduces GI inflammation; may support alertness alongside nausea relief | Pine, rosemary |
| Linalool | Calms the nervous system; reduces anxiety that worsens nausea; GABA-A modulation | Lavender, basil |
Research specifically supports limonene for nausea. One study found that lemon inhalation aromatherapy — limonene being the primary compound in lemon essential oil — reduced pregnancy-induced nausea and vomiting. The Elevate Holistics analysis of terpenes for nausea confirms limonene as one of the best-documented terpenes for antiemetic effects across multiple nausea causes.
The most effective terpene combinations for nausea:
- Limonene + beta-caryophyllene — covers both serotonin modulation and GI inflammation (best for daytime, chemo-related nausea)
- Myrcene + beta-caryophyllene — physical relaxation plus GI anti-inflammation (best for evening, nausea with pain)
- Limonene + alpha-pinene — nausea relief with maintained clarity (best for daytime, functional use)
Best Strain Profiles for Nausea by Type
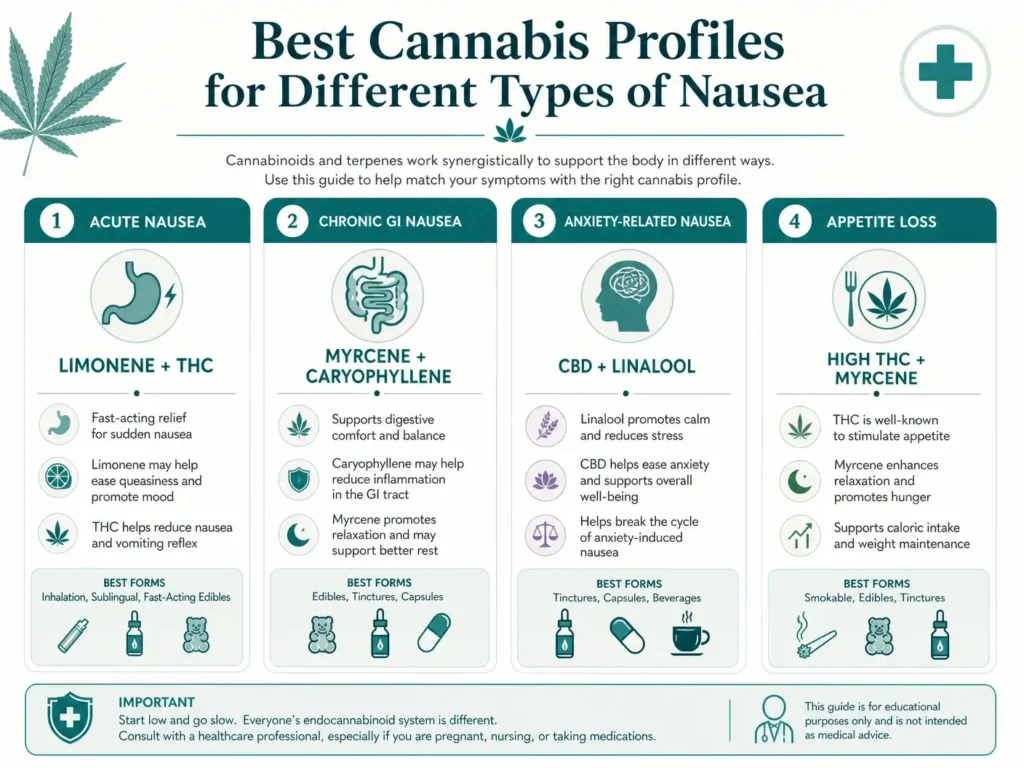
Rather than recommending specific strain names — which vary significantly in actual terpene content between PA growers — this section describes the chemical profiles to look for based on your nausea type. Ask your dispensary pharmacist to match these profiles to current menu products.
For Acute or Moderate Nausea (Motion Sickness, Medication Side Effects, GI Upset)
Profile to look for:
- THC: 15–22%
- Dominant terpenes: Limonene primary, myrcene secondary
- Form: Vaporizable flower or concentrate for fast onset
Strains commonly displaying this profile include Lemon Haze, Jack Herer, and Super Lemon Haze — all sativa-leaning, limonene-forward, and documented for mood-brightening effects that help with anxiety-driven nausea. The citrusy aroma is itself a useful indicator that limonene content is present.
For Severe or Chronic Nausea (Crohn’s, IBD, Terminal Illness)
Profile to look for:
- THC: 18–25%
- Dominant terpenes: Myrcene primary, beta-caryophyllene secondary
- CBD: 1–5% can help reduce psychoactive intensity without compromising antiemetic effect
- Form: Vaporizable flower for acute episodes; tincture sublingual for sustained relief
Strains commonly displaying this profile include OG Kush, Northern Lights, and Granddaddy Purple. These are indica-dominant, body-focused, deeply relaxing, and consistently reported by medical patients managing chronic GI conditions as effective antiemetics.
For Nausea With Anxiety or Mood Disturbance
Profile to look for:
- THC: 12–18% (moderate — higher THC can worsen anxiety-driven nausea)
- CBD: 5–12% for balance
- Dominant terpenes: Linalool and/or limonene
Cannatonic is the most widely cited strain in this category — a balanced THC:CBD hybrid with myrcene, linalool, and caryophyllene as dominant terpenes. It produces minimal psychoactivity while maintaining antiemetic and anxiolytic effects. Consistently recommended for patients who need daytime nausea management without cognitive impairment.
For Nausea With Loss of Appetite
Profile to look for:
- THC: 20–25%
- Dominant terpenes: Myrcene, limonene, caryophyllene
- Form: Vaporizable flower or sublingual tincture
Cannabis’s appetite-stimulating (“munchies”) effect is well-documented and directly mediated by CB1 receptor activation in the hypothalamus — the same system involved in nausea suppression. For patients whose nausea is also suppressing appetite (common in cancer and terminal illness), strains high in THC with a myrcene-dominant profile address both simultaneously.
Best Strains for Chemotherapy-Induced Nausea (CINV)
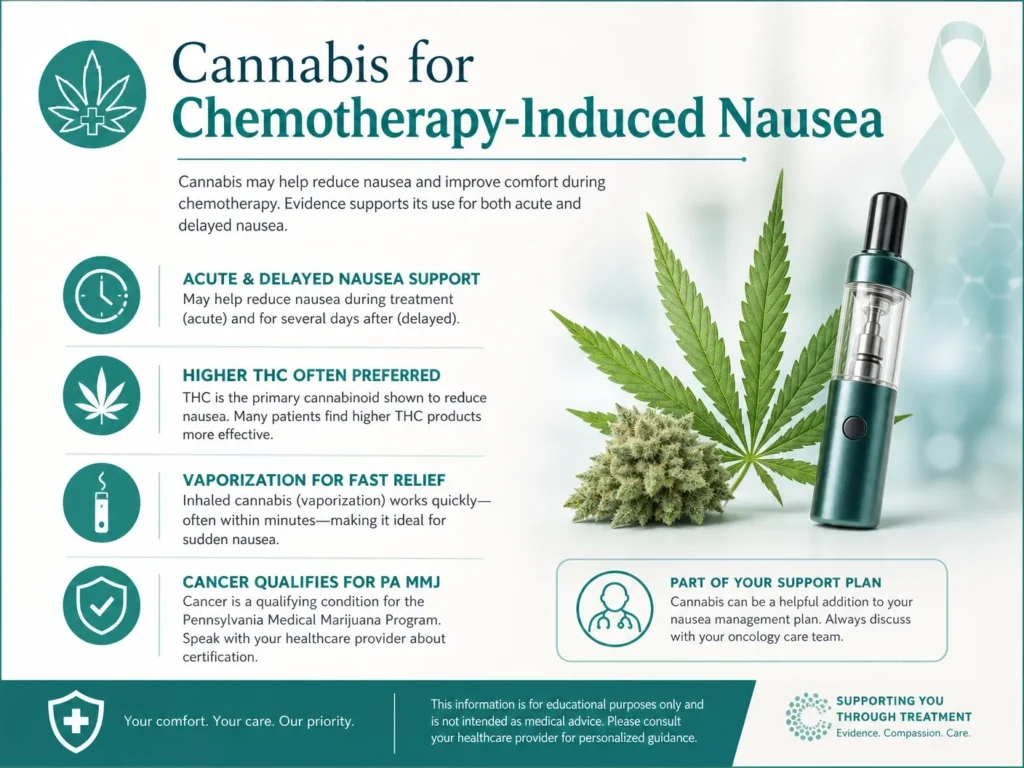
Chemotherapy-induced nausea and vomiting is the most medically urgent and best-researched application of cannabis for nausea. It deserves its own section.
CINV occurs in two phases:
- Acute phase: within 24 hours of chemotherapy
- Delayed phase: 24 hours to 5 days post-treatment
Standard pharmaceutical antiemetics (ondansetron, metoclopramide) control acute-phase vomiting effectively for most patients — but delayed-phase nausea remains a major unmet need. This is where cannabis has shown particular promise.
A comprehensive review published in PMC (PMC4034105) confirmed that cannabinoids — particularly THC — act as broad-spectrum antiemetics against diverse emetic stimuli, including both acute and delayed CINV in both animal models and clinical patients.
The University of Rochester has an active Phase 2 clinical trial (NCT07374939) currently evaluating medical cannabis as an adjunct to standard antiemetic therapy specifically for CINV — a sign of how seriously oncology researchers are now treating this application.
For CINV specifically, the evidence supports:
- Higher THC content (20%+) for maximum CB1 activation
- Limonene + beta-caryophyllene terpene profile — synergistic antiemetic effects
- Vaporization as the preferred delivery method (oral ingestion is problematic when patients are actively nauseated)
- Prophylactic timing — using cannabis before a chemotherapy session, not reactively during peak nausea, produces better outcomes
Pennsylvania recognizes cancer as a qualifying condition for medical marijuana under Act 16 of 2016. Patients undergoing chemotherapy in Pennsylvania can access medical cannabis through a licensed dispensary with a valid PA MMJ card.
Consumption Method: Why It Matters as Much as the Strain
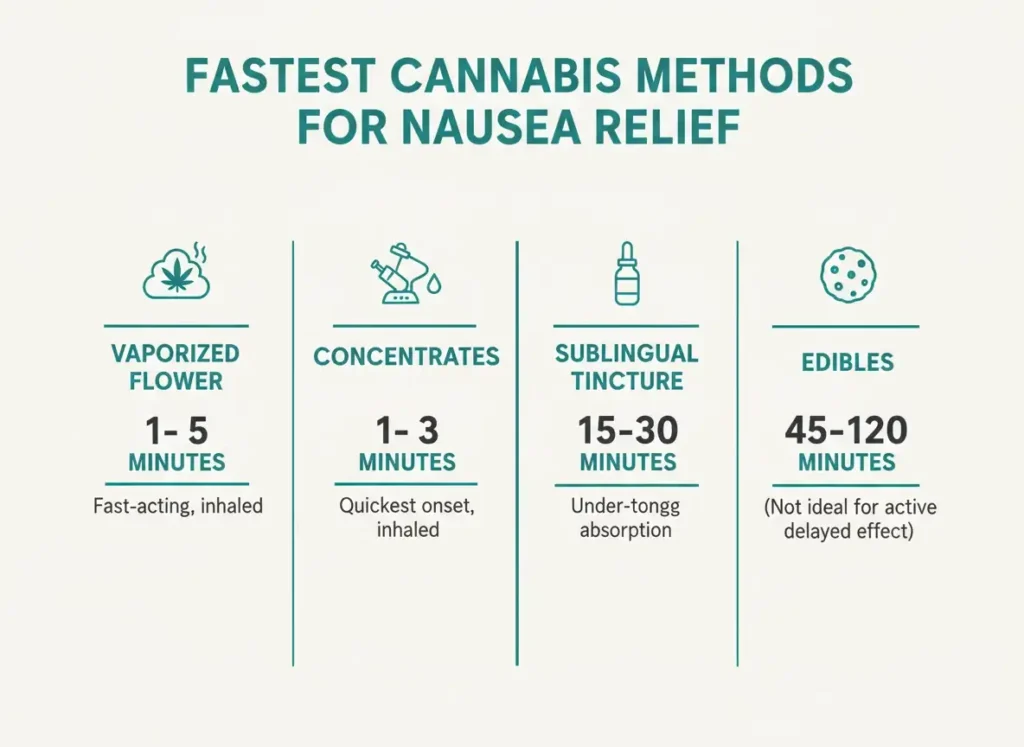
Choosing the right strain is half the equation. How you consume it determines how quickly it works — and for nausea, timing is everything.
| Method | Onset | Duration | Best For |
|---|---|---|---|
| Vaporized flower | 1–5 minutes | 1–3 hours | Acute nausea — fastest relief |
| Concentrate (dab/vape cart) | 1–3 minutes | 2–4 hours | Acute or severe nausea |
| Sublingual tincture | 15–30 minutes | 3–6 hours | Sustained relief, moderate nausea |
| Edibles | 45–120 minutes | 4–8 hours | NOT recommended for active nausea |
| Topicals | N/A (no systemic effect) | N/A | Not effective for nausea |
Why edibles are the wrong choice for active nausea: Edibles require digestion to absorb cannabinoids. A nauseous stomach digests poorly and inconsistently — meaning onset is unpredictable, the dose may not absorb at the expected rate, and patients may vomit before the medication has effect. For chronic nausea management between episodes, low-dose edibles can play a role. For acute nausea relief, vaporization is the evidence-supported method.
For CINV patients: Pennsylvania law permits vaporization of cannabis flower. Smoking is prohibited under state law. Patients should use a vaporizer device — not combust the flower — both for legal compliance and for respiratory health.
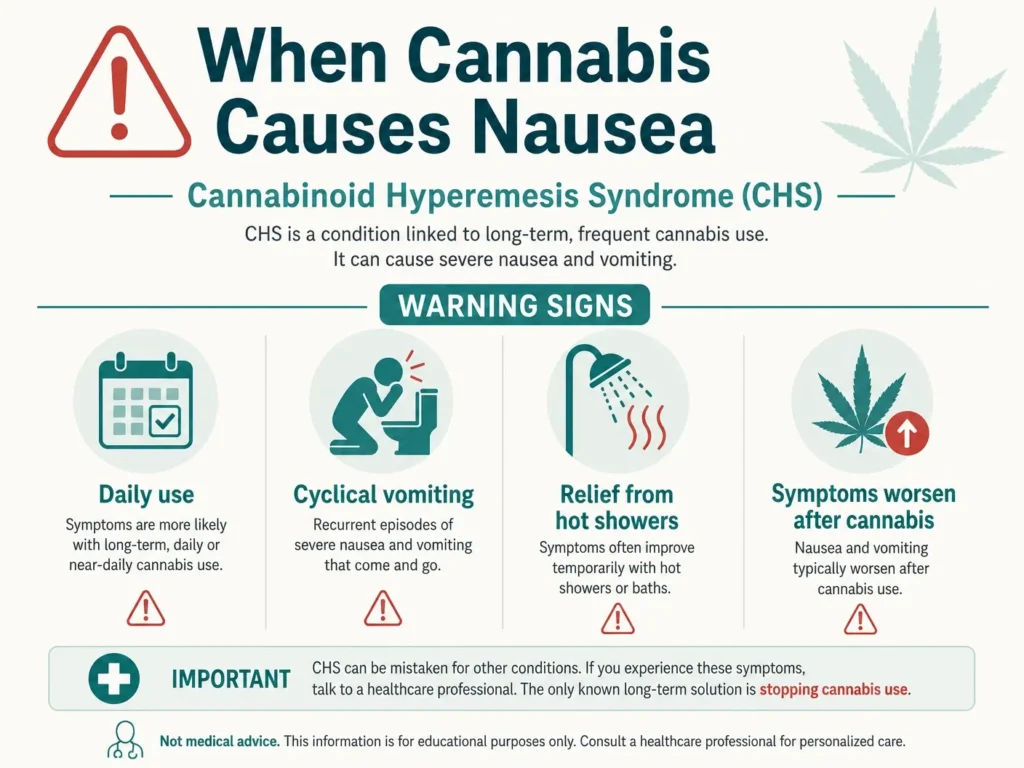
The Critical Warning: Cannabis Can Also Cause Nausea
This is the section that separates genuinely helpful, honest content from promotional fluff — and it could protect a patient from a serious misdiagnosis.
Cannabinoid Hyperemesis Syndrome (CHS) is a real, documented medical condition in which long-term, frequent cannabis use paradoxically causes severe, cyclical nausea, vomiting, and abdominal cramping. It was first documented in 2004 and cases have increased steadily as cannabis potency has risen and use has expanded.
CHS is characterized by three phases:
- Prodromal phase: Morning nausea, mild abdominal discomfort, anxiety about vomiting — can last months to years
- Hyperemetic phase: Severe, persistent vomiting (up to 5 times per hour), abdominal pain, dehydration, weight loss — patients often present to emergency departments
- Recovery phase: Symptoms resolve after cannabis cessation
The hallmark warning signs of CHS (not ordinary nausea):
- Nausea and vomiting that worsen, not improve, after cannabis use
- Temporary relief from hot showers or baths (a distinctive, well-documented feature of CHS)
- Daily or near-daily cannabis use over months or years
- Cyclical episodes that recur weeks to months apart
- Previous use of cannabis for nausea that stopped working
A February 2026 UCHealth Today report confirmed CHS is now the leading cause of marijuana-related emergency department visits. CHS is frequently misdiagnosed as cyclic vomiting syndrome (CVS) or gastroparesis.
The only effective treatment for CHS is complete cannabis cessation. Adding more cannabis — including different strains — will not resolve CHS and may worsen it. If you recognize these symptoms in yourself or a patient, the information in this article does not apply to your situation. Please consult a physician.
A Note on Pregnancy Nausea
Some people searching for the best cannabis strain for nausea may be experiencing pregnancy-related morning sickness. This deserves a direct, unambiguous statement.
Cannabis use during pregnancy is strongly contraindicated. The American College of Obstetricians and Gynecologists (ACOG) advises against all cannabis use during pregnancy. Research has associated prenatal cannabis exposure with small-for-gestational-age infants, preterm birth, and possible neurodevelopmental consequences in the child. The NCBI StatPearls review of cannabinoid antiemetic therapy explicitly states that “cannabinoid use during pregnancy is unsafe.”
This applies regardless of whether the product is labeled medical marijuana, CBD, or hemp-derived. If you are pregnant and experiencing severe nausea (hyperemesis gravidarum), please consult your OB-GYN about evidence-based treatment options.
How Dose Affects Nausea — The Biphasic Effect
Almost no guide mentions this — but it’s clinically important.
Cannabis’s effect on nausea is biphasic — meaning it behaves differently at low versus high doses:
- Low to moderate doses → antiemetic (reduces nausea)
- Very high doses → potentially pro-emetic (can induce or worsen nausea)
This is why a patient who finds 5mg of THC helpful for nausea might find 30mg makes them feel sick. It’s also part of the mechanism behind CHS, where long-term, high-dose exposure shifts the endocannabinoid system’s response from antiemetic to pro-emetic.
The PMC comprehensive review of CHS (PMC11597608) confirms the biphasic mechanism: “Cannabis has anti-emetic properties at low doses; however, at higher doses, it induces vomiting.”
The practical implication: Start low. For nausea management, doses of 2.5–5mg THC are often cited as sufficient for meaningful antiemetic effect. Escalating THC rapidly is not the right approach and may produce the opposite result.
How to Shop for Anti-Nausea Cannabis at a PA Dispensary
Pennsylvania state law requires every licensed dispensary product to have a Certificate of Analysis (COA) before sale — which means you have access to verified terpene and cannabinoid data for every product on the shelf.
Step-by-step dispensary checklist for nausea:
- Tell the pharmacist your situation. PA dispensaries employ licensed pharmacists. Describe your nausea cause (chemo, GI condition, medication side effects, etc.) and whether it’s acute or chronic.
- Request products with verified terpene panels. Ask to see COAs. Look specifically for limonene, myrcene, and beta-caryophyllene as dominant terpenes.
- Choose vaporizable formats for acute relief. Flower or vape cartridges for immediate onset. Tinctures for sustained management.
- Start with moderate THC. 15–20% for most conditions; 20%+ for severe CINV. Avoid jumping straight to the highest-THC products.
- Avoid edibles for active nausea. The digestion requirement makes them unreliable during active symptoms.
- Keep a simple record. Note the product, dominant terpenes, THC%, and your response. Adjust from there.
Does Nausea Qualify for a PA Medical Marijuana Card?
Nausea itself is not a standalone qualifying condition in Pennsylvania — but the underlying conditions that most commonly cause medically significant nausea are. Several qualifying conditions under Pennsylvania’s medical marijuana program specifically include nausea as a documented symptom that cannabis is recognized to treat:
| Qualifying Condition | Nausea Connection |
|---|---|
| Cancer (including remission therapy) | Chemotherapy-induced nausea and vomiting (CINV) is among the most validated uses |
| Crohn’s Disease | Chronic GI inflammation causes persistent nausea |
| Inflammatory Bowel Disease (IBD) | Cannabinoid receptors throughout the gut; nausea is a primary symptom |
| Terminal Illness | Nausea from illness progression and medication side effects |
| Chronic Hepatitis C | Treatment regimens commonly produce severe nausea |
| HIV/AIDS | Medication-induced nausea; wasting syndrome |
If your nausea is associated with any of these conditions, you may qualify for a Pennsylvania medical marijuana card. The certification process is completed entirely online via telehealth with Dr. Johnathon Chance Miller, MD — typically the same day.
| Physician Fee | PA State Fee | Total | |
|---|---|---|---|
| New Patient | $159 | $50 | $209 |
| Renewal | $149 | $50 | $199 |
| MMAP Qualifying Patients (Medicaid, SNAP, WIC, CHIP, PACE, PACENET) | — | $0 (waived) | Physician fee only |
Start your same-day certification here.
Frequently Asked Questions — Best Strain for Nausea
Q: What is the best cannabis strain for nausea?
A: There is no single “best” strain — what matters is the chemical profile. For nausea, look for strains with moderate-to-high THC (15–25%) and dominant terpenes of limonene, myrcene, and beta-caryophyllene. These terpenes work synergistically with THC to suppress nausea through CB1 receptor activation in the brainstem and serotonin modulation in the gut. Limonene-forward strains like Lemon Haze and Jack Herer are documented for daytime nausea. Myrcene-dominant strains like OG Kush and Northern Lights are often preferred for severe or chronic nausea. At Pennsylvania dispensaries, ask the pharmacist to show you the COA terpene panel rather than selecting by strain name alone.
Q: How does cannabis reduce nausea?
A: Cannabis reduces nausea primarily through THC’s activation of CB1 receptors in the dorsal vagal complex (DVC) — the brainstem region that controls the vomiting reflex. THC also acts on serotonin 5-HT3 receptors in the DVC, the same pathway targeted by pharmaceutical antiemetics like ondansetron (Zofran). This dual mechanism explains why cannabis can work for nausea even when standard medications have failed. Certain terpenes — especially limonene and beta-caryophyllene — enhance this antiemetic effect through complementary anti-inflammatory and serotonin-modulating pathways.
Q: Can cannabis make nausea worse?
A: Yes, in certain circumstances. Long-term, frequent cannabis users can develop Cannabinoid Hyperemesis Syndrome (CHS) — a paradoxical condition where cannabis causes severe, cyclical nausea and vomiting rather than relieving it. Warning signs include nausea that worsens after cannabis use, temporary relief from hot showers, and cyclical vomiting episodes that recur over weeks or months. CHS is now the leading cause of marijuana-related emergency department visits according to a February 2026 UCHealth report. The only effective treatment is complete cannabis cessation. Additionally, very high doses of THC can be pro-emetic even in people without CHS — cannabis is antiemetic at low-to-moderate doses but can produce nausea at excessive doses.
Q: Is cannabis safe for pregnancy nausea?
A: No. Cannabis use during pregnancy is strongly contraindicated by the American College of Obstetricians and Gynecologists (ACOG). Research has linked prenatal cannabis exposure to small-for-gestational-age infants, preterm birth, and possible neurodevelopmental consequences. This applies to all cannabis products, including CBD and hemp-derived products. If you are pregnant and experiencing severe nausea, speak with your OB-GYN about evidence-based treatment options rather than using cannabis.
Q: Why are edibles not recommended for active nausea?
A: Edibles require digestion to absorb cannabinoids into the bloodstream. A nauseous or vomiting stomach digests poorly and inconsistently, making absorption unpredictable and onset timing unreliable. In some cases, a patient may vomit before the medication is absorbed at all. For acute nausea relief, vaporizing cannabis flower or using a concentrate provides onset within 1–5 minutes and is the evidence-supported delivery method. Sublingual tinctures (held under the tongue for 60 seconds) offer a middle ground with 15–30 minute onset and are a better option than edibles for patients who prefer not to inhale.
Q: Does nausea qualify for a PA medical marijuana card?
A: Nausea alone is not a standalone qualifying condition in Pennsylvania. However, several PA-recognized qualifying conditions include nausea as a primary symptom that cannabis is documented to treat — including cancer (chemotherapy-induced nausea), Crohn’s disease, inflammatory bowel disease (IBD), terminal illness, HIV/AIDS, and chronic Hepatitis C. Patients whose nausea is associated with any of these conditions may qualify for a Pennsylvania medical marijuana card through an online telehealth certification.
Q: What terpenes are best for nausea?
A: The three best-documented terpenes for nausea relief are limonene, myrcene, and beta-caryophyllene. Limonene modulates serotonin pathways in both the gut and brain and has been studied for antiemetic effects in pregnant women. Myrcene relaxes smooth muscle in the GI tract and reduces inflammatory cytokines that can trigger nausea. Beta-caryophyllene activates CB2 receptors in the gut to reduce GI inflammation and protect the stomach lining. The most effective combinations are limonene + beta-caryophyllene for daytime chemo-related nausea and myrcene + beta-caryophyllene for evening use with pain. These terpene levels are listed on every COA at licensed Pennsylvania dispensaries.
Q: What is the difference between cannabis for nausea and Cannabinoid Hyperemesis Syndrome?
A: Cannabis is an effective antiemetic for most people — working through CB1 and serotonin receptor mechanisms in the brainstem. Cannabinoid Hyperemesis Syndrome (CHS) is a paradoxical condition that affects a subset of long-term, daily cannabis users in which the same receptors are chronically overstimulated, reversing the antiemetic effect and causing severe, cyclical vomiting. The key distinguishing features of CHS are: nausea that worsens after cannabis use (not improves), temporary relief from hot showers or baths, and daily or near-daily use over months or years. The only cure for CHS is stopping cannabis use completely. If nausea is not resolving with cannabis and is getting worse, consult a physician before using more.
Medical Disclaimer
This blog post is intended for general educational purposes only and does not constitute medical advice. Cannabis is not appropriate for everyone experiencing nausea — particularly pregnant individuals, long-term daily users who may have CHS, and patients with conditions that warrant physician supervision. Always consult a licensed physician before using cannabis for medical purposes. The research cited in this article represents the current state of evidence as of April 2026; some studies are preclinical and may not directly translate to human outcomes. Information verified as of April 2026. Medically reviewed by Dr. Johnathon Chance Miller, MD.
Sources
All sources verified as of April 2026.
- Parker et al. — “Cannabinoids Inhibit Emesis Through CB1 Receptors in the Brainstem” — PubMed (PMC, peer-reviewed)
- Darmani et al. — “Delta-9-THC Selectively Acts on CB1 Receptors in Dorsal Vagal Complex to Inhibit Emesis” — American Journal of Physiology (peer-reviewed)
- Vemuri et al. — “Endocannabinoid Signaling in Stress, Nausea, and Vomiting” — Neurogastroenterology & Motility (2025, PMC11872018)
- Darmani — “Mechanisms of Broad-Spectrum Antiemetic Efficacy of Cannabinoids Against CINV” — PMC4034105 (peer-reviewed)
- Cannabinoid Antiemetic Therapy — StatPearls / NCBI Bookshelf (updated August 2025)
- ClinicalTrials.gov — NCT07374939: Medical Cannabis for Nausea in Patients Receiving Moderately or Highly Emetogenic Chemotherapy — University of Rochester (Phase 2, active)
- UCHealth Today — “What Is CHS? The Leading Cause of Marijuana-Related ER Visits” (February 27, 2026)
- Al-Harbi & El-Sakka — “A Comprehensive Review and Update on Cannabis Hyperemesis Syndrome” — PMC11597608 (peer-reviewed)
- Medical Terpenes — “What Are the Best Terpenes for Nausea?” (peer-referenced)
- NuggMD — “Best Terpenes for Nausea” (October 2024)
- Elevate Holistics — “Finding the Perfect Terpenes for Nausea and Inflammation” (September 2025)
- DSS Genetics — “Best Strains for Nausea: Antiemetic Terpene Profiles and Dosing Strategies” (March 2026)